Download as pdf or txt
You might also like
- ECG Interpretation Cheat SheetDocument1 pageECG Interpretation Cheat Sheethirsi20051881% (26)
- Cardiac DysrhythmiasDocument3 pagesCardiac DysrhythmiasKatherine Santiago92% (62)
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (239)
- Basic EKG ECG Rhythms CheatsheetDocument1 pageBasic EKG ECG Rhythms CheatsheetAhmad88% (8)
- AHA ACLS Megacode ScenariosDocument6 pagesAHA ACLS Megacode ScenariosVitor Hugo G Correia86% (7)
- Emergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareFrom EverandEmergency Department Resuscitation of the Critically Ill, 2nd Edition: A Crash Course in Critical CareNo ratings yet
- Basic EKG For DummiesDocument133 pagesBasic EKG For Dummieseduardocmoura88% (8)
- EKG Practice TestDocument16 pagesEKG Practice TestAbdul Rohim100% (1)
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationFrom EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationRating: 3 out of 5 stars3/5 (1)
- Basic Arrhythmia RulesDocument3 pagesBasic Arrhythmia Rulesgreenflames0997% (30)
- The 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsFrom EverandThe 12-Lead Electrocardiogram for Nurses and Allied ProfessionalsNo ratings yet
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- Dysrhythmias Cheat SheetDocument2 pagesDysrhythmias Cheat SheetKatie Coughlan100% (2)
- Schaum's Outline of Emergency Nursing: 242 Review QuestionsFrom EverandSchaum's Outline of Emergency Nursing: 242 Review QuestionsRating: 4.5 out of 5 stars4.5/5 (3)
- ECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasFrom EverandECG/EKG Interpretation: An Easy Approach to Read a 12-Lead ECG and How to Diagnose and Treat ArrhythmiasRating: 5 out of 5 stars5/5 (2)
- Ecg StripsDocument39 pagesEcg StripsNursyNurse100% (3)
- EcgDocument57 pagesEcgenii_ta100% (9)
- Ecg Made Ridiculously Easy!Document78 pagesEcg Made Ridiculously Easy!momobelle100% (9)
- ECG InterpretationDocument52 pagesECG InterpretationMarcus, RN98% (45)
- EKG Flash CardsDocument5 pagesEKG Flash CardsRyann Sampino FreitasNo ratings yet
- Haemodynamic Monitoring & Manipulation: an easy learning guideFrom EverandHaemodynamic Monitoring & Manipulation: an easy learning guideNo ratings yet
- Summary of ECG AbnormalitiesDocument8 pagesSummary of ECG AbnormalitiesChristine Nancy NgNo ratings yet
- ECG Master Class-1Document132 pagesECG Master Class-1Shohag ID Center100% (1)
- EKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!From EverandEKG and ECG Interpretation: Learn EKG Interpretation, Rhythms, and Arrhythmia Fast!No ratings yet
- EKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXFrom EverandEKG/ECG Interpretation Made Easy: A Practical Approach to Passing the ECG/EKG Portion of NCLEXRating: 5 out of 5 stars5/5 (2)
- ECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!From EverandECG & EKG Interpretation: How to interpret ECG & EKG, including rhythms, arrhythmias, and more!No ratings yet
- EKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookFrom EverandEKG Interpretation Basics Guide: Electrocardiogram Heart Rate Determination, Arrhythmia, Cardiac Dysrhythmia, Heart Block Causes, Symptoms, Identification and Medical Treatment Nursing HandbookNo ratings yet
- Abnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandAbnormal Slow Heart Beats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ECG InterpretationDocument5 pagesECG InterpretationRichelle Dianne Ramos-Giang100% (3)
- Sinus Bradycardia: o No TX If AsymptomaticDocument3 pagesSinus Bradycardia: o No TX If Asymptomaticelle50% (2)
- EKG Rhythms2 PDFDocument7 pagesEKG Rhythms2 PDFAya KamajayaNo ratings yet
- ECG Made Easy by Mallareddy SripujaDocument46 pagesECG Made Easy by Mallareddy Sripujagrreddy836100% (3)
- A Simplified ECG GuideDocument4 pagesA Simplified ECG Guidejalan_z96% (28)
- ECG InterpretationDocument95 pagesECG InterpretationShiela Mae Lopez100% (11)
- ECG Rhythm Interpretation 2007Document533 pagesECG Rhythm Interpretation 2007user123456798100% (20)
- Boot Camp Hemodynamic MonitoringDocument37 pagesBoot Camp Hemodynamic MonitoringTinaHo100% (8)
- EKG Quick and Dirty - GD v3.0Document2 pagesEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)
- Ecg Taking and Interpretation.... PowerpointDocument37 pagesEcg Taking and Interpretation.... PowerpointJara Maris Moreno BudionganNo ratings yet
- ECG Interpretation - Axis and Conduction AbnormalitiesDocument9 pagesECG Interpretation - Axis and Conduction Abnormalitiesradha1000100% (1)
- ECG InterpretationDocument52 pagesECG InterpretationFranspol50% (2)
- Reading A EKGDocument10 pagesReading A EKGMayer Rosenberg100% (15)
- Cardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCardiac Tamponade, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Bonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!From EverandBonehead Electrocardiography: The Easiest and Best Way to Learn How to Read Electrocardiograms—No Bones About It!Rating: 5 out of 5 stars5/5 (2)
- Advance Cardiac Life Support: Short, Sweet and to the PointFrom EverandAdvance Cardiac Life Support: Short, Sweet and to the PointRating: 3 out of 5 stars3/5 (2)
- Surviving the ICU: A Toolkit for the Critical Care NurseFrom EverandSurviving the ICU: A Toolkit for the Critical Care NurseNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Differences in Morbidity and Mortality in Down Syndrome Are Related To The Type of Congenital Heart DefectDocument10 pagesDifferences in Morbidity and Mortality in Down Syndrome Are Related To The Type of Congenital Heart DefectMaría BonettiNo ratings yet
- Paroxysmal Supraventricular TachycardiasDocument27 pagesParoxysmal Supraventricular TachycardiasTor JaNo ratings yet
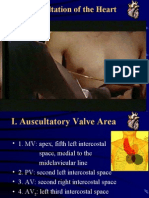
- Auscultation of HeartDocument92 pagesAuscultation of Heartsanjivdas100% (1)
- Athlete's Heart: Dr. Arzalan BaigDocument59 pagesAthlete's Heart: Dr. Arzalan BaigArzalan BaigNo ratings yet
- Ebsteins Anomaly Contemporary Management StrategiDocument13 pagesEbsteins Anomaly Contemporary Management StrategiRJMNo ratings yet
- Rido, Rudini - Paediatric ECGDocument51 pagesRido, Rudini - Paediatric ECGFikriYTNo ratings yet
- Critical Care Dr. Valerie Zarza GeronDocument88 pagesCritical Care Dr. Valerie Zarza GeronDivine Grace FernandezNo ratings yet
- ArrhythmiasDocument53 pagesArrhythmiasRobert MontgomeryNo ratings yet
- Kuliah EkgDocument30 pagesKuliah EkgMuhammad Ari AnugrahNo ratings yet
- Tricuspid Valve DiseaseDocument20 pagesTricuspid Valve Diseasesarguss14100% (1)
- 10 Common EKG Heart Rhythms PDFDocument1 page10 Common EKG Heart Rhythms PDFtashaNo ratings yet
- Cardiovascular DiseaseDocument11 pagesCardiovascular Diseasefrenielyn obananNo ratings yet
- Cardio Quiz 1Document30 pagesCardio Quiz 1Dennis BaluyutNo ratings yet
- Congestive - Cardiac-FailureDocument38 pagesCongestive - Cardiac-FailureAkhil R KrishnanNo ratings yet
- Pericarditis: Dr. Alfredo Gonzales SaavedraDocument38 pagesPericarditis: Dr. Alfredo Gonzales SaavedraSandy Burgos CabanillasNo ratings yet
- Nennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyDocument10 pagesNennyelyaniginting,+7 +Yoani+Maria+Vianney+Bita+AtyBayu IsmoyoNo ratings yet
- Cardiology Step 2 CK NotesDocument5 pagesCardiology Step 2 CK NotesVidur S SinghNo ratings yet
- Pericardial Diseases MCQsDocument3 pagesPericardial Diseases MCQsfeeo8266No ratings yet
- Congestive Heart Failure - PathophysiologyDocument1 pageCongestive Heart Failure - PathophysiologyPong's Teodoro SalvadorNo ratings yet
- Supra Ventricular Tachycardia in PregnancyDocument2 pagesSupra Ventricular Tachycardia in PregnancylulzimkamberiNo ratings yet
- HCM Treatment Italy Ammirati2016Document13 pagesHCM Treatment Italy Ammirati2016xy manNo ratings yet
- Basic ECG For Refresher Course 2014Document116 pagesBasic ECG For Refresher Course 2014Winz DolleteNo ratings yet
- Nurs 5024 Cardiology PP PresentationDocument13 pagesNurs 5024 Cardiology PP Presentationapi-415083061No ratings yet
- Atrial Septal Defect PDFDocument4 pagesAtrial Septal Defect PDFTien Chen TuNo ratings yet
- Cardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Document337 pagesCardiac Resynchronization Therapy (Sep 19 2007) - (1841846376) - (CRC Press)Morozovschi VitalieNo ratings yet
- Arrythmias 2-3Document4 pagesArrythmias 2-3cayla mae carlosNo ratings yet
- MCQDocument20 pagesMCQAhmedabdo AbdoNo ratings yet
- VT Bradycardias AnswDocument128 pagesVT Bradycardias AnswJoshua-Majid ShahbaziNo ratings yet