Download as docx, pdf, or txt
You might also like
- Deep Pressure Proprioceptive ProtocolsDocument6 pagesDeep Pressure Proprioceptive Protocolsnss100% (1)
- Reading Process Worksheet PalenciaDocument4 pagesReading Process Worksheet PalenciaFranz PalenciaNo ratings yet
- THERMO KING TK 61377-18-MM TKV500 and TKV600 Maintenance Manual Rev. A 01-19Document108 pagesTHERMO KING TK 61377-18-MM TKV500 and TKV600 Maintenance Manual Rev. A 01-19Vincent Marmande100% (1)
- Muscles of The Upper Limb Made EasyDocument7 pagesMuscles of The Upper Limb Made Easynss93% (27)
- Strategic Change - 2006 - Greener - Managing Change Before Change ManagementDocument8 pagesStrategic Change - 2006 - Greener - Managing Change Before Change ManagementdanaNo ratings yet
- Coding BreakdownDocument2 pagesCoding BreakdownAlex SouzaNo ratings yet
- Multifidus ExercicesDocument2 pagesMultifidus Exercicesjo21cu100% (1)
- Weir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Document8 pagesWeir Et Al. (2019) - Approaching Groin Pain in Athletics 'The Falcon's Perspective'Tom StevensNo ratings yet
- Case Study: Mulligan Concept Management of "Tennis Elbow"Document3 pagesCase Study: Mulligan Concept Management of "Tennis Elbow"noonoons100% (1)
- Presenting Your FindingsDocument11 pagesPresenting Your FindingsnssNo ratings yet
- 314Document65 pages314dim4erema100% (3)
- Tests of Examination of CervicalDocument10 pagesTests of Examination of CervicalAde Yahya NasutionNo ratings yet
- Muscles of Gait (Biomechanics)Document25 pagesMuscles of Gait (Biomechanics)Rory CocksNo ratings yet
- Passive MovementsDocument1 pagePassive MovementsomhreemaimhreemNo ratings yet
- Muscoli BiarticolariDocument2 pagesMuscoli Biarticolarielpibedeoro1993No ratings yet
- Cap. 5 Kinesiology and Functional Characteristics of The Upper LimbDocument30 pagesCap. 5 Kinesiology and Functional Characteristics of The Upper LimbLuis EstradaNo ratings yet
- Neck Pain Exercise SheetDocument2 pagesNeck Pain Exercise Sheetkang soon cheolNo ratings yet
- Screenshot - Ankle and Foot ComplexDocument4 pagesScreenshot - Ankle and Foot Complexno nameNo ratings yet
- Flexed Arm Hang TestDocument3 pagesFlexed Arm Hang TestAriff MohamedNo ratings yet
- Cardiac RehabilitationDocument44 pagesCardiac RehabilitationadnanNo ratings yet
- Anatomical Variation of Sciatic Nerve Course in Saudi Population A Magnetic Resonance Imaging StudyDocument8 pagesAnatomical Variation of Sciatic Nerve Course in Saudi Population A Magnetic Resonance Imaging StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Functional Evaluative Tests RevisedDocument4 pagesFunctional Evaluative Tests RevisedaocannonNo ratings yet
- Walking Impairment QuestionnairDocument2 pagesWalking Impairment QuestionnaircpradheepNo ratings yet
- Kinesio GoldDocument9 pagesKinesio GoldHenrique AthadeuNo ratings yet
- De Quervain S TenosynovitisDocument13 pagesDe Quervain S TenosynovitisPremaKurniaNo ratings yet
- Ankle SprainDocument24 pagesAnkle SprainPrisca AngelinaNo ratings yet
- Deep Tissue MassageDocument5 pagesDeep Tissue MassageNanokoSanchezOrtizNo ratings yet
- Osgood Schlatter Disease With Exercises ChocDocument4 pagesOsgood Schlatter Disease With Exercises ChocJoni MokodoNo ratings yet
- Shockwave Therapy MZUEDocument21 pagesShockwave Therapy MZUELove & HumanityNo ratings yet
- Gait Analysis: - Study of Human Locomotion - Walking and Running - Walking Is A Series of Gait CyclesDocument41 pagesGait Analysis: - Study of Human Locomotion - Walking and Running - Walking Is A Series of Gait CyclesSonu SinghNo ratings yet
- What Is Dry Needling MaDocument6 pagesWhat Is Dry Needling MaElanghovan ArumugamNo ratings yet
- Strength Prehabilitation For The Shoulder ComplexDocument35 pagesStrength Prehabilitation For The Shoulder ComplexvalentinNo ratings yet
- Proprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionDocument10 pagesProprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionAlejandra VasquezNo ratings yet
- Motor Learning Applications For Agility Pt2Document5 pagesMotor Learning Applications For Agility Pt2hmimezNo ratings yet
- Normal Human LocomotionDocument16 pagesNormal Human LocomotionWendy NgNo ratings yet
- Axis and Plane of ThumbDocument3 pagesAxis and Plane of Thumbraveena rajput100% (1)
- The Mayo Elbow Performance Score PDFDocument1 pageThe Mayo Elbow Performance Score PDFwahyu_sitaNo ratings yet
- LGS Capita Selecta: by Indira Vidiari & M YusufDocument30 pagesLGS Capita Selecta: by Indira Vidiari & M YusufniekoNo ratings yet
- Shoulder Kines (Autosaved)Document86 pagesShoulder Kines (Autosaved)niekoNo ratings yet
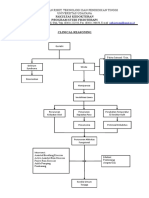
- Clinical ReasoningDocument1 pageClinical ReasoningIda Bagus Gde Dharma DhyaksaNo ratings yet
- Shoulder Pain Impingement SyndromeDocument30 pagesShoulder Pain Impingement SyndromeAfifah NurNo ratings yet
- Arm, Forearm, Hand MuscleDocument18 pagesArm, Forearm, Hand MusclerabeyaNo ratings yet
- MMT 6-1Document20 pagesMMT 6-1Mughal ZadiiNo ratings yet
- Pelvic GirdleDocument21 pagesPelvic GirdlecptconsultingNo ratings yet
- Cervical Spondylosis and Neck PainDocument5 pagesCervical Spondylosis and Neck PainIsaac AlemanNo ratings yet
- Assessment of KneeDocument113 pagesAssessment of KneeIqra Iftikhar100% (1)
- New Techniques in Physical TherapyDocument61 pagesNew Techniques in Physical TherapyMohamed Magdy El MeligieNo ratings yet
- Bio Mechanics and Motor Control of Human Movement 4editionDocument13 pagesBio Mechanics and Motor Control of Human Movement 4editionStanko.Stuhec8307100% (2)
- Medical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)Document41 pagesMedical Rehabilitation in Musculoskeletal Trauma - Prof. Dr. Dr. Angela BM Tulaar SPKFR (K)YanuarNo ratings yet
- Hip MusclesDocument31 pagesHip MusclesvinaymanNo ratings yet
- Rom PDFDocument6 pagesRom PDFPrivat EtavirpNo ratings yet
- Nebraska CoreDocument42 pagesNebraska CoreGreg MarsoNo ratings yet
- PNF TechniquesDocument26 pagesPNF Techniquesabdul haseebNo ratings yet
- Low Back Exam PDFDocument2 pagesLow Back Exam PDFDeeea1991No ratings yet
- Cervical FlexibilityDocument3 pagesCervical Flexibilitymec17No ratings yet
- Biomechanic of Gait AnalysisDocument42 pagesBiomechanic of Gait AnalysisTonny N. Firmansyah100% (1)
- Lower Crossed Syndrome - LPHCDDocument3 pagesLower Crossed Syndrome - LPHCDLauren PatelNo ratings yet
- Sop Muskulo (Tennis Elbow)Document15 pagesSop Muskulo (Tennis Elbow)Melissa Erjani Adam100% (2)
- Jaspal R Singh, M.D.: Department of Rehabilitation MedicineDocument2 pagesJaspal R Singh, M.D.: Department of Rehabilitation MedicineshikhaNo ratings yet
- Dry Needling Article SRF JournalDocument3 pagesDry Needling Article SRF JournalObreNo ratings yet
- Low Back Pain ICM 1 RHWDocument53 pagesLow Back Pain ICM 1 RHWchloeNo ratings yet
- Algoritma Neck PainDocument12 pagesAlgoritma Neck PainAri SudarsonoNo ratings yet
- Biomechanics of Knee - FinalDocument68 pagesBiomechanics of Knee - FinalDr. Sabari ManokaranNo ratings yet
- Goniometry 2Document18 pagesGoniometry 2Sai RamNo ratings yet
- Biomechanics of The Knee During Closed Kinetic Chain ExercisesDocument31 pagesBiomechanics of The Knee During Closed Kinetic Chain ExercisesJean SantosNo ratings yet
- Rotator Cuff Tears Orthoinfo - Aaos.org TopicDocument7 pagesRotator Cuff Tears Orthoinfo - Aaos.org TopicMontserrat LandaNo ratings yet
- Gallop: Gait and Lower Limb Observation of Paediatrics - Standardised Recording Template (Addendum)Document3 pagesGallop: Gait and Lower Limb Observation of Paediatrics - Standardised Recording Template (Addendum)stevo69No ratings yet
- Gordon S Functional Health Pattern Assessment ToolDocument10 pagesGordon S Functional Health Pattern Assessment ToolMiguel VicenteNo ratings yet
- Asymmetric Patterns in The Cranial Skeleton of Zebra FishDocument7 pagesAsymmetric Patterns in The Cranial Skeleton of Zebra FishnssNo ratings yet
- Minimal Detectable Change (MDC)Document21 pagesMinimal Detectable Change (MDC)nssNo ratings yet
- A Question of Foot DominanceDocument8 pagesA Question of Foot Dominancenss100% (1)
- Oswestry Low Back Disability QuestionnaireDocument4 pagesOswestry Low Back Disability QuestionnairenssNo ratings yet
- Choosing An Appropriate Statistical Test: Abc of Research MethodologyDocument4 pagesChoosing An Appropriate Statistical Test: Abc of Research MethodologynssNo ratings yet
- Exercise Program For Total Knee Replacement: North Shore/Coast Garibaldi, Vancouver and RichmondDocument12 pagesExercise Program For Total Knee Replacement: North Shore/Coast Garibaldi, Vancouver and RichmondnssNo ratings yet
- Sample Follow-Up LettersDocument2 pagesSample Follow-Up LettersMhira AlmeroNo ratings yet
- Throwing EventsDocument11 pagesThrowing Eventsrovel shelieNo ratings yet
- Lecture 3 Early Embryonic DevelopmentDocument40 pagesLecture 3 Early Embryonic DevelopmentZari Sofia LevisteNo ratings yet
- Industrial Crops & ProductsDocument10 pagesIndustrial Crops & ProductsShield YggdrasilNo ratings yet
- Sports and Entertainment Marketing: Sample Role PlaysDocument36 pagesSports and Entertainment Marketing: Sample Role PlaysTAHA GABRNo ratings yet
- Diagrama 950H PDFDocument1 pageDiagrama 950H PDFDaniel Castillo PeñaNo ratings yet
- Arduino Robot Arm TFCDDocument10 pagesArduino Robot Arm TFCDNelson MendivelsoNo ratings yet
- Pizza Maker & Kitche N Crew Evaluations: Type of EvaluationDocument3 pagesPizza Maker & Kitche N Crew Evaluations: Type of Evaluationhari juharaNo ratings yet
- The GiantDocument4 pagesThe GiantBug BeeNo ratings yet
- How To Analyse Non-Fictional Texts-1Document5 pagesHow To Analyse Non-Fictional Texts-1chaymaelmeknassi2No ratings yet
- Sooceal ProjectDocument40 pagesSooceal ProjectSushil ShresthaNo ratings yet
- Be Project Work BookDocument44 pagesBe Project Work BookCASTING DEPARTMENTNo ratings yet
- COD Testing in Environmental Laboratory of Environmental Engineering Diponegoro UniversityDocument10 pagesCOD Testing in Environmental Laboratory of Environmental Engineering Diponegoro UniversityTasha RifantiNo ratings yet
- Gas Bill AprilDocument4 pagesGas Bill AprilMozhie OicangiNo ratings yet
- TRANSITIONS 5 WebDocument40 pagesTRANSITIONS 5 WebCARDONA CHANG Micaela AlessandraNo ratings yet
- Repair-Training Quotation: Dododo Medical Equipment Service Co.,LtdDocument1 pageRepair-Training Quotation: Dododo Medical Equipment Service Co.,LtdPhong DoNo ratings yet
- Manual Armado 960E-1 Serial Number A30003-A30024 CEAW005502Document338 pagesManual Armado 960E-1 Serial Number A30003-A30024 CEAW005502Joel Carvajal ArayaNo ratings yet
- Classification of FinishesDocument5 pagesClassification of FinishesOjasvee Kashyap100% (1)
- TXVs - All You Need To KnowDocument4 pagesTXVs - All You Need To KnowOmar ArdilaNo ratings yet
- Meng 310 Exam 01 Spring 2010Document4 pagesMeng 310 Exam 01 Spring 2010Abdulrahman AlzahraniNo ratings yet
- Dissertation Topics On Banking SectorDocument6 pagesDissertation Topics On Banking SectorWriteMyPaperIn3HoursCanada100% (1)
- (20-58) Charging Case Firmware Update Guide For R180 - Rev1.1Document6 pages(20-58) Charging Case Firmware Update Guide For R180 - Rev1.1Brandon CifuentesNo ratings yet
- Loksewa Monthly Report of Baisakh 2077Document26 pagesLoksewa Monthly Report of Baisakh 2077Ritu ConsultantsNo ratings yet
- Worksheet MAPEH Arts Q4-W3Document4 pagesWorksheet MAPEH Arts Q4-W3Hezel Mercado EdrozoNo ratings yet
- GloverDocument272 pagesGlovermidialaoropesaNo ratings yet