Download as docx, pdf, or txt
You might also like
- Pass Nclex IN 30 DAYS!Document9 pagesPass Nclex IN 30 DAYS!Jude olga75% (4)
- The Woman Speaks To The Man Who Has Employed Her SonDocument3 pagesThe Woman Speaks To The Man Who Has Employed Her SonSerena SulawammotNo ratings yet
- Colorectal CancerDocument18 pagesColorectal CancerKimie PanganNo ratings yet
- Tribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns ProgrammeDocument76 pagesTribhuwan University Institute of Medicine Nepalgunj Nursing Campus Bns Programmeone twoNo ratings yet
- Laryngeal Obstruction: Narciso A. CañibanDocument54 pagesLaryngeal Obstruction: Narciso A. Cañibanalexandrajane200767% (3)
- Assessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationDocument10 pagesAssessment Nursing Diagnosis Inference Objectives Nursing Intervention Rationale EvaluationJobelle Acena100% (2)
- NCPDocument1 pageNCPanon-61963867% (3)
- Related NCPDocument5 pagesRelated NCPLara GatbontonNo ratings yet
- Colon Rectal CancerDocument6 pagesColon Rectal Cancerbryantmaroney811No ratings yet
- Cast CareDocument1 pageCast CareCarmelita SaltNo ratings yet
- Anatomy and Physiology-KidneyDocument4 pagesAnatomy and Physiology-KidneySharmaineGuinchomaNo ratings yet
- 4 Corners Gold Rush Lesson PlanDocument3 pages4 Corners Gold Rush Lesson Planapi-267003013No ratings yet
- Fundamentals of Nursing PDFDocument18 pagesFundamentals of Nursing PDFJamaica Manuel Iglesias100% (6)
- Coronary Artery Disease Case StudyDocument7 pagesCoronary Artery Disease Case StudySana RazaNo ratings yet
- Peritoneal Carcinomatosis Grand Case StudyDocument69 pagesPeritoneal Carcinomatosis Grand Case StudyBeverly Joy RubiNo ratings yet
- ColorectalCancer - Case StudyDocument28 pagesColorectalCancer - Case StudyColeen Mae CamaristaNo ratings yet
- Case Study MijaresDocument55 pagesCase Study Mijaresiura echinNo ratings yet
- AppendectomyDocument39 pagesAppendectomyBella IsananNo ratings yet
- Case Study Tension Pneumothorax BSN 4 2 1Document57 pagesCase Study Tension Pneumothorax BSN 4 2 1aaron tabernaNo ratings yet
- A Case Study On Mild Compression Deformity L1Document25 pagesA Case Study On Mild Compression Deformity L1JM UncianoNo ratings yet
- Case StudyDocument12 pagesCase StudyAllan Roy Malibiran BalderamaNo ratings yet
- Case Study On Peptic UlcerDocument11 pagesCase Study On Peptic UlcerFHAMITHA100% (1)
- Case Study Lung Adenocarcinoma PDFDocument43 pagesCase Study Lung Adenocarcinoma PDFFrancis Anthony LoslosoNo ratings yet
- Dental Prob NCPDocument3 pagesDental Prob NCPx483xDNo ratings yet
- CASE Study PTBDocument52 pagesCASE Study PTBbennettchuaNo ratings yet
- Murari Lal Memorial School and College of Nursing, SolanDocument18 pagesMurari Lal Memorial School and College of Nursing, SolanSimran ChauhanNo ratings yet
- Case Study For Colorectal CancerDocument23 pagesCase Study For Colorectal CancerAnjanette ViloriaNo ratings yet
- Ortho Case StudyDocument17 pagesOrtho Case StudyAndrea Sibayan SorianoNo ratings yet
- Multiple SclerosisDocument35 pagesMultiple SclerosisJc SeguiNo ratings yet
- Case Study On Communicable DiseaseDocument15 pagesCase Study On Communicable DiseaseThiradevi BalakrisnanNo ratings yet
- Care PlanDocument4 pagesCare PlangopscharanNo ratings yet
- Skin Cancer: I. Overview of The DisorderDocument3 pagesSkin Cancer: I. Overview of The DisorderSung ChiiNo ratings yet
- Case Study On Ibd17Document2 pagesCase Study On Ibd17api-381128376No ratings yet
- SchistosomiasisDocument5 pagesSchistosomiasisBryan TarrobalNo ratings yet
- Care of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryDocument13 pagesCare of The Client With Pulmonary Tuberculosis Utilizing Orem's TheoryRazel Kinette AzotesNo ratings yet
- Skin Grafting Surgical NursingDocument21 pagesSkin Grafting Surgical NursingHEMMA100% (1)
- Hypovolemic Shock 09Document58 pagesHypovolemic Shock 09Joanne Bernadette Aguilar100% (2)
- Urinary Tract InfectionDocument18 pagesUrinary Tract InfectionljefarrahNo ratings yet
- Liver Cancer Case StudyDocument38 pagesLiver Cancer Case Studyabdellatif100% (2)
- Ineffective Health Management Related To Mrs. Gama: Provide The Client Enough Knowledge About The ProblemDocument5 pagesIneffective Health Management Related To Mrs. Gama: Provide The Client Enough Knowledge About The ProblemAndrea Albester GarinoNo ratings yet
- Acute Renal FailureDocument17 pagesAcute Renal FailureDina Rasmita100% (1)
- Gastrostomy FeedingDocument9 pagesGastrostomy FeedingJamie Luz Tongco0% (1)
- Cancer Case StudyDocument15 pagesCancer Case StudyRobin HaliliNo ratings yet
- A Health Education On PneumoniaDocument3 pagesA Health Education On PneumoniaJoshuaNo ratings yet
- Stealing Innocent Beans: Wilms' Tumor: BSN Iii-FDocument40 pagesStealing Innocent Beans: Wilms' Tumor: BSN Iii-Ffidc_0428100% (3)
- Leptospirosis CaseDocument29 pagesLeptospirosis CaseJp RectraNo ratings yet
- Fluorosis: Fluoride Toxicity: Patient Management & MonitoringDocument24 pagesFluorosis: Fluoride Toxicity: Patient Management & MonitoringdrjriNo ratings yet
- Cardiovascular HealthDocument20 pagesCardiovascular HealthChrrieNo ratings yet
- PoliomyelitisDocument14 pagesPoliomyelitisEzekiel Reyes100% (1)
- Electrolyte Imbalance 1Document3 pagesElectrolyte Imbalance 1Marius Clifford BilledoNo ratings yet
- Anatomy and Physiology PneumoniaDocument4 pagesAnatomy and Physiology PneumoniaJohnson MallibagoNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument76 pagesChronic Obstructive Pulmonary DiseasedidinNo ratings yet
- LARYNGITISDocument13 pagesLARYNGITIStherese BNo ratings yet
- Care of Casts and Splints - OrthoInfo - AAOSDocument2 pagesCare of Casts and Splints - OrthoInfo - AAOSSAIFUL ISLAMNo ratings yet
- Case Scenario - NebulizationDocument2 pagesCase Scenario - NebulizationHilario. Hayascent.Reign.M.No ratings yet
- Vaginal CancerDocument11 pagesVaginal CancerAiko TokunagaNo ratings yet
- Osteosarcoma Case StudyDocument17 pagesOsteosarcoma Case StudyJoeven HilarioNo ratings yet
- Case Analysis Group 1Document47 pagesCase Analysis Group 1bunso padillaNo ratings yet
- 1 - Scope of Critical Care NursingDocument20 pages1 - Scope of Critical Care Nursinghanimozaghi100% (1)
- Ineffective ProtectionDocument7 pagesIneffective Protectionapi-283822730No ratings yet
- NCP - Pulmonary TuberculosisDocument6 pagesNCP - Pulmonary TuberculosisastrijuNo ratings yet
- Care of Unconscious ClientDocument27 pagesCare of Unconscious ClientDonelie Kay Tapel AsanzaNo ratings yet
- Meningitis - Introduction and ManagementDocument27 pagesMeningitis - Introduction and ManagementAmmo KhanNo ratings yet
- Cylone - Lab Report - FinalizeDocument19 pagesCylone - Lab Report - FinalizeSiti Khairunnur LaderlahNo ratings yet
- Columbus CEO Leaderboard - Home Healthcare AgenciesDocument1 pageColumbus CEO Leaderboard - Home Healthcare AgenciesDispatch MagazinesNo ratings yet
- Sentinel Collim Rev1.2 CompressedDocument2 pagesSentinel Collim Rev1.2 CompressedBauyrzhanNo ratings yet
- Electrical and Electronic Troubleshooting For Industrial EnginesDocument25 pagesElectrical and Electronic Troubleshooting For Industrial EnginespanddyanNo ratings yet
- Anti-A, Anti-B o Anti-AB: MonoclonalDocument4 pagesAnti-A, Anti-B o Anti-AB: Monoclonalkonan iqNo ratings yet
- Materials Chemistry A: Journal ofDocument7 pagesMaterials Chemistry A: Journal ofFamiloni LayoNo ratings yet
- Material HPLCDocument19 pagesMaterial HPLCIsmil ImamaNo ratings yet
- OSH SeminarDocument2 pagesOSH SeminarSahar Ulu JeruasNo ratings yet
- Final LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFDocument74 pagesFinal LIST OF IMPORTANT GRID ELEMENTS Updated On May 2020 PDFbhargavNo ratings yet
- Bossing Nicole PDFDocument47 pagesBossing Nicole PDFMark CastilloNo ratings yet
- The Development of A Heat Wave Vulnerability Index For London-2013Document10 pagesThe Development of A Heat Wave Vulnerability Index For London-2013gilberto777No ratings yet
- 00000102Document108 pages00000102Scary CreaturesNo ratings yet
- 1.1 - Monitor de Aterramento - 8030Document2 pages1.1 - Monitor de Aterramento - 8030Denis MarcosNo ratings yet
- PHAS0027 RevisionDocument21 pagesPHAS0027 Revisionunknown.unknown9901No ratings yet
- Sdfsdynamic AuscultationDocument3 pagesSdfsdynamic AuscultationrichardNo ratings yet
- BRAC Annual Report 2017 PDFDocument116 pagesBRAC Annual Report 2017 PDFShoaib AhmedNo ratings yet
- MAC-LAB Assistant 5BDocument38 pagesMAC-LAB Assistant 5BAbdelhakszn SznNo ratings yet
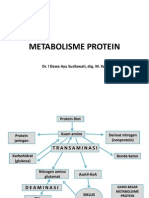
- Metabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesDocument31 pagesMetabolisme Protein: Dr. I Dewa Ayu Susilawati, Drg. M. KesMelisa Novitasari100% (2)
- PDS - CS - Form - No - 212 SHERLADocument8 pagesPDS - CS - Form - No - 212 SHERLASherla Catulay Godinez NautanNo ratings yet
- II 2015 4Document283 pagesII 2015 4tuni santeNo ratings yet
- Natural Rubber WikiDocument9 pagesNatural Rubber WikiMyra Wardati SNo ratings yet
- Screenshot 2022-10-07 at 9.15.02 PMDocument1 pageScreenshot 2022-10-07 at 9.15.02 PMoNo ratings yet
- Learning Activity Sheet Electronics G10 Q3 W1Document5 pagesLearning Activity Sheet Electronics G10 Q3 W1Mark Anthony Discarga JetajobeNo ratings yet
- Muscular Triangles of The NeckDocument3 pagesMuscular Triangles of The NeckSam TagardaNo ratings yet
- Catálogo de Referencias - Power Conversion SystemsDocument60 pagesCatálogo de Referencias - Power Conversion SystemsBENo ratings yet
- Environmental Crisis Causes and ManifestationsDocument26 pagesEnvironmental Crisis Causes and Manifestationsबाजीराव सिंघम0% (1)