Download as doc, pdf, or txt
You might also like
- Randall M. Packard - A History of Global Health - Interventions Into The Lives of Other Peoples (2016, JHU Press)Document428 pagesRandall M. Packard - A History of Global Health - Interventions Into The Lives of Other Peoples (2016, JHU Press)Paloma Porto100% (2)
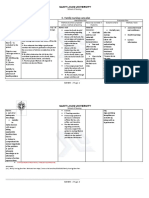
- C. Family Nursing Care Plan: Saint Louis UniversityDocument2 pagesC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Training Manual Hypertensive Disorder in Pregnancy 3rd Edition 2018 PDFDocument140 pagesTraining Manual Hypertensive Disorder in Pregnancy 3rd Edition 2018 PDFJaspreet KaurNo ratings yet
- Delivery Type, Opioid Prescribing, and The Risk ofDocument3 pagesDelivery Type, Opioid Prescribing, and The Risk ofadityoNo ratings yet
- Farquharson 2002Document6 pagesFarquharson 2002Nur Khairani putriNo ratings yet
- APSDocument18 pagesAPSNadya NovianiNo ratings yet
- Iugr PreventionDocument62 pagesIugr PreventionShreedevi KoppadNo ratings yet
- Induction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationDocument6 pagesInduction of Labor With Misoprostol For Premature Rupture of Membranes Beyond Thirty-Six Weeks' GestationFebrinata MahadikaNo ratings yet
- Enoxa en Obesas Post-CesareaDocument5 pagesEnoxa en Obesas Post-CesareaKrmnCruzJiménezNo ratings yet
- A Combination Treatment of Prednisone Aspirin Folate and Progesterone in Women With Idiopathic Recurrent MiscarriageDocument28 pagesA Combination Treatment of Prednisone Aspirin Folate and Progesterone in Women With Idiopathic Recurrent MiscarriagedrnyolNo ratings yet
- Chaemsaithong2019 PDFDocument62 pagesChaemsaithong2019 PDFAdriani HartantoNo ratings yet
- Enoxaparin and AspirinDocument11 pagesEnoxaparin and AspirinFemtom PriyoNo ratings yet
- Jurnal 6Document8 pagesJurnal 6Bayek NgekekNo ratings yet
- A Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeDocument10 pagesA Comparison Between Epidural and IV Tramadol For Painless Labor and Effect On Perinatal OutcomeLibay Villamor IsmaelNo ratings yet
- Csii-Pregnancy in Patients With Mechanical Prosthetic ValvesDocument6 pagesCsii-Pregnancy in Patients With Mechanical Prosthetic Valvesapi-205989841No ratings yet
- Oral Plenary Session I: Results: ResultsDocument2 pagesOral Plenary Session I: Results: ResultsfujimeisterNo ratings yet
- January 2003: East African Medical Journal 51Document5 pagesJanuary 2003: East African Medical Journal 51simoncktNo ratings yet
- Pregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDocument6 pagesPregnancy With Epilepsy - A Retrospective Analysis: Gynetology & ObstetricsDwi Rofiqoh FauzahNo ratings yet
- Piis0002937811009185 PDFDocument24 pagesPiis0002937811009185 PDFLailatuss LelaNo ratings yet
- Malaria Dan KeguguranDocument23 pagesMalaria Dan Keguguranwoouuw0903No ratings yet
- Mihu 2015Document7 pagesMihu 2015Nuryasni NuryasniNo ratings yet
- Early Prediction and Aspirin For Prevention of Pre-Eclampsia (EPAPP) Study: A Randomized Controlled TrialDocument5 pagesEarly Prediction and Aspirin For Prevention of Pre-Eclampsia (EPAPP) Study: A Randomized Controlled TrialTeguh SulistiyantoNo ratings yet
- ASPREDocument5 pagesASPREIvan Gonzalez PintoNo ratings yet
- Ultrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolDocument7 pagesUltrasound in Obstet Gyne - 2021 - Fernlund - Reproductive Outcome After Early Miscarriage Comparing Vaginal MisoprostolPutu Gede WidyatamaNo ratings yet
- High-Dose Versus Low-Dose Oxytocin For Augmentation of Delayed LabourDocument6 pagesHigh-Dose Versus Low-Dose Oxytocin For Augmentation of Delayed LabourAdhitya Pratama SutisnaNo ratings yet
- Chips Trial ReferenceDocument11 pagesChips Trial ReferenceDr.Nilar WinNo ratings yet
- COVID-19 and T2DMDocument3 pagesCOVID-19 and T2DMMarijosse NavarroNo ratings yet
- Progesterone and The Risk of Preterm Birth Among Women With A Short CervixDocument8 pagesProgesterone and The Risk of Preterm Birth Among Women With A Short Cervixangela_karenina_1No ratings yet
- First Trimester Bleeding and Pregnancy Outcomes: Case-Control StudyDocument4 pagesFirst Trimester Bleeding and Pregnancy Outcomes: Case-Control StudyClara Nur RamadhaniNo ratings yet
- 1 s2.0 S1110569015300042 MainDocument5 pages1 s2.0 S1110569015300042 MainAzam alausyNo ratings yet
- Ebp Paper Final Draft2Document38 pagesEbp Paper Final Draft2natalie nodayNo ratings yet
- Poster Session I: Perinatal Outcome of Women With Epilepsy: Results From A Population-Based Cohort StudyDocument1 pagePoster Session I: Perinatal Outcome of Women With Epilepsy: Results From A Population-Based Cohort StudyasfwegereNo ratings yet
- Prevention of Pre-Eclampsia by Low-Molecular-Weight Heparin in Addition To Aspirin: A Meta-AnalysisDocument7 pagesPrevention of Pre-Eclampsia by Low-Molecular-Weight Heparin in Addition To Aspirin: A Meta-AnalysisAnonymous 9OHpuvNo ratings yet
- GineDocument9 pagesGineJorge PeralesNo ratings yet
- Antepartum Transabdominal Amnioinfusion in Oligohydramnios - A Comparative StudyDocument4 pagesAntepartum Transabdominal Amnioinfusion in Oligohydramnios - A Comparative StudyVashti SaraswatiNo ratings yet
- Influence of Acupuncture Stimulation On Pregnancy Rates For Women Undergoing Embryo TransferDocument7 pagesInfluence of Acupuncture Stimulation On Pregnancy Rates For Women Undergoing Embryo TransferFerry DimyatiNo ratings yet
- Comparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialDocument5 pagesComparison of Two Different Antibiotic Regimens For The Prophylaxisis of Cases With Preterm Premature Rupture of Membranes: A Randomized Clinical TrialVindee VictoryNo ratings yet
- The NeoUpdates - DecDocument7 pagesThe NeoUpdates - DecDr Satish MishraNo ratings yet
- Terapi Relaksasi Akupresur Untuk Mengatasi Keluhan Mual Dan Muntah Pada Ibu HamilDocument5 pagesTerapi Relaksasi Akupresur Untuk Mengatasi Keluhan Mual Dan Muntah Pada Ibu HamilfikriaNo ratings yet
- AmniotomiDocument8 pagesAmniotomibidan22No ratings yet
- Jri 15 147 PDFDocument5 pagesJri 15 147 PDFNabeel KhanNo ratings yet
- Recurrent Pregnancy Loss With AntiphospholipidDocument10 pagesRecurrent Pregnancy Loss With Antiphospholipidparekh.pravin1961No ratings yet
- Provider Resources Obstetrics Late Preterm Steroids July2016Document10 pagesProvider Resources Obstetrics Late Preterm Steroids July2016Pediatrics SLCM-WHQMNo ratings yet
- Sectio Pada Preeclampsia BeratDocument4 pagesSectio Pada Preeclampsia BeratJosepb SimarmataNo ratings yet
- Low Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665Document5 pagesLow Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665GayathriMaranNo ratings yet
- Ect Pregnancy Review LiteratureDocument6 pagesEct Pregnancy Review Literaturec5e4jfpn100% (1)
- Picot AnalysisDocument4 pagesPicot AnalysisLittle StarNo ratings yet
- Laparoscopic ClomipenDocument5 pagesLaparoscopic ClomipenHar YudhaNo ratings yet
- Gaviscon ClinicalDocument7 pagesGaviscon ClinicalMuhammad Nadzri NoorhayatuddinNo ratings yet
- Content ServerDocument7 pagesContent ServerRoni WahyudiNo ratings yet
- Magpie TrialDocument14 pagesMagpie TrialadammzjinNo ratings yet
- Ijpr 13 299Document6 pagesIjpr 13 299Iene Dhiitta PramudNo ratings yet
- Aspirin Plus Heparin or Aspirini Alone in WomanDocument20 pagesAspirin Plus Heparin or Aspirini Alone in WomanYafet Yanri SirupangNo ratings yet
- 2012 Article 61Document5 pages2012 Article 61Al MubartaNo ratings yet
- Antenatal Betamethasone For Women at RiskDocument10 pagesAntenatal Betamethasone For Women at RiskThapakorn JalearnyingNo ratings yet
- Immunoglobulin Therapy in Recurrent Pregnancy LossDocument6 pagesImmunoglobulin Therapy in Recurrent Pregnancy Lossdoctor wajihaNo ratings yet
- Menstrual Cycle..Wisdom ExtractionDocument4 pagesMenstrual Cycle..Wisdom ExtractionAL-Khawaldeh HamzaNo ratings yet
- Prediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery DopplerDocument6 pagesPrediction of Recurrent Preeclampsia Using First-Trimester Uterine Artery Dopplerganesh reddyNo ratings yet
- Mjiri 32 104Document5 pagesMjiri 32 104Nur ChusnulNo ratings yet
- 08-Premature ThelarcheDocument6 pages08-Premature ThelarcheBruno SantanaNo ratings yet
- Isx No EffectDocument6 pagesIsx No EffectThomas Regina PutraNo ratings yet
- NEJM Mifepristone Pretreatment For The Medical Management 2018Document10 pagesNEJM Mifepristone Pretreatment For The Medical Management 2018Federico López BidartNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- College Information Profama - CompressedDocument122 pagesCollege Information Profama - CompressedmaruthaiNo ratings yet
- Hepatitis 1Document6 pagesHepatitis 1DmpsNo ratings yet
- Drug: Audenz: 1 / 1 5 / 2 1 Principles of ToxicologyDocument16 pagesDrug: Audenz: 1 / 1 5 / 2 1 Principles of ToxicologyMaria PriorNo ratings yet
- Daftar Pustaka PertusisDocument1 pageDaftar Pustaka PertusisErica PuteriNo ratings yet
- NEBOSH Lesson PlanDocument2 pagesNEBOSH Lesson PlanShezi Bhatti100% (1)
- MARK HENDERSON HWWS UNICEF Mark Henderson NewDocument17 pagesMARK HENDERSON HWWS UNICEF Mark Henderson Newash amenNo ratings yet
- Food, Health and NutritionDocument18 pagesFood, Health and NutritionMaschil VilchesNo ratings yet
- Breast Cancer KelseyDocument12 pagesBreast Cancer Kelseyapi-3802092No ratings yet
- Get Rid of All Whites in UsDocument6 pagesGet Rid of All Whites in UsYLNDNo ratings yet
- AstraZeneca Vaccination Fact Sheet FINALDocument2 pagesAstraZeneca Vaccination Fact Sheet FINALAnaesthesia Intensive Care LecturerNo ratings yet
- 627 1196 1 PBDocument7 pages627 1196 1 PBannisa dian zizianiNo ratings yet
- Reading Comprehension: 1. Are The Following Statements True or False ? Justify!Document2 pagesReading Comprehension: 1. Are The Following Statements True or False ? Justify!anaNo ratings yet
- Handwashing Lesson LogDocument4 pagesHandwashing Lesson LogJoseph Bahian-AbangNo ratings yet
- Typhoid Vaccines: What You Need To KnowDocument2 pagesTyphoid Vaccines: What You Need To KnowRohit KohliNo ratings yet
- Meeting Briefing DocumentDocument53 pagesMeeting Briefing DocumentErin O'BrienNo ratings yet
- Demon in The Freezer Final QuestionsDocument3 pagesDemon in The Freezer Final QuestionseddfungusNo ratings yet
- Daftar Pustaka: Raka, L, 2010Document2 pagesDaftar Pustaka: Raka, L, 2010dnoksNo ratings yet
- Barangay Pulo: Republic of The Philippines City of ValenzuelaDocument3 pagesBarangay Pulo: Republic of The Philippines City of ValenzuelaBarangay Pulo ValenzuelaNo ratings yet
- TSA WinS Booklet Sanitation FINAL WEB 20181105Document68 pagesTSA WinS Booklet Sanitation FINAL WEB 20181105Reg Sevilla SibalNo ratings yet
- Interior Services - Ii: Plumbing and SanitationDocument17 pagesInterior Services - Ii: Plumbing and Sanitationrose2006No ratings yet
- Bibliography Sexual Health Issues WTDDocument4 pagesBibliography Sexual Health Issues WTDndoybbx65No ratings yet
- Emerging and Reemerging Infectious DiseasesDocument25 pagesEmerging and Reemerging Infectious DiseasesNorberto Francisco BaldiNo ratings yet
- Unit 613 Level 3 Monitor and Maintain Health and Safety Practice in The Salon - Taught ContentDocument2 pagesUnit 613 Level 3 Monitor and Maintain Health and Safety Practice in The Salon - Taught ContentbbjoyweNo ratings yet
- Audit Program Ppi (Mariani, SKM, Mha)Document23 pagesAudit Program Ppi (Mariani, SKM, Mha)Dedy HartantyoNo ratings yet
- 1.20.22 - Inspection Report - GinosDocument3 pages1.20.22 - Inspection Report - GinosKristina KoppeserNo ratings yet
- REQUEST FOR ASSESSMENT EIM NC II - Dec 19, 2020 NEW PDFDocument39 pagesREQUEST FOR ASSESSMENT EIM NC II - Dec 19, 2020 NEW PDFChe MoralesNo ratings yet
- Final Health Care Associated InfectionDocument23 pagesFinal Health Care Associated Infectionramanand chaudharyNo ratings yet