Download as pdf
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Role of Fate in Oedipus RexDocument8 pagesThe Role of Fate in Oedipus Rexshaharbano2000100% (5)
- From Research To Solution: The Legal CaseDocument1 pageFrom Research To Solution: The Legal CasealiasnetworkNo ratings yet
- ALIAS Conference 2015 ProgrammeDocument4 pagesALIAS Conference 2015 ProgrammealiasnetworkNo ratings yet
- ALIAS Products FlyerDocument2 pagesALIAS Products FlyeraliasnetworkNo ratings yet
- ALIAS Headed PaperDocument1 pageALIAS Headed PaperaliasnetworkNo ratings yet
- SESAR Magazine Issue12 Oct2014Document16 pagesSESAR Magazine Issue12 Oct2014aliasnetworkNo ratings yet
- The ALIAS BrochureDocument12 pagesThe ALIAS BrochurealiasnetworkNo ratings yet
- The ALIAS CalendarDocument2 pagesThe ALIAS CalendaraliasnetworkNo ratings yet
- 065, G. Contissa Et Al., Automation and Liability in ATM As Fundamental Issues in Socio-Technical SystemsDocument3 pages065, G. Contissa Et Al., Automation and Liability in ATM As Fundamental Issues in Socio-Technical SystemsaliasnetworkNo ratings yet
- The UAS Scenario - Conflicting PurposesDocument9 pagesThe UAS Scenario - Conflicting PurposesaliasnetworkNo ratings yet
- LDCE Notes/Notes For LDCE-LGS/25Document3 pagesLDCE Notes/Notes For LDCE-LGS/25R Sathish KumarNo ratings yet
- NTCC Project 1Document14 pagesNTCC Project 1sameer aliNo ratings yet
- Assignment Strategic ManagementDocument18 pagesAssignment Strategic ManagementDarmmini MiniNo ratings yet
- Disaster Plan: CommunityDocument1 pageDisaster Plan: CommunityJace MyouiNo ratings yet
- Hurricane Katrina Research Paper TopicsDocument8 pagesHurricane Katrina Research Paper Topicstog0filih1h2100% (1)
- 22 SURVIV SALES-LETTER - Do You Have What It Takes To Survive If A Disaster OccursDocument8 pages22 SURVIV SALES-LETTER - Do You Have What It Takes To Survive If A Disaster OccursALEX.TAWIAHNo ratings yet
- Industrial Accidents Triggered by Earthquakes, Floods and Lightning: Lessons Learned From A Database AnalysisDocument16 pagesIndustrial Accidents Triggered by Earthquakes, Floods and Lightning: Lessons Learned From A Database AnalysismaheshNo ratings yet
- LEO Quiz No. 3 - Google FormsDocument8 pagesLEO Quiz No. 3 - Google FormsSenen Sean100% (1)
- Playbook - GM - SpreadsDocument13 pagesPlaybook - GM - SpreadsFinkFrozenNo ratings yet
- Constituent Violence 1947-1950 - Ariella's CargoDocument3 pagesConstituent Violence 1947-1950 - Ariella's CargomangsilvaNo ratings yet
- 2 VocabularyDocument1 page2 VocabularysauvaNo ratings yet
- Basing 24 MaretDocument3 pagesBasing 24 MaretDewi Aphrodite100% (1)
- Disaster-Risk-Reduction Final Exam 2020 Grade11 The OrigDocument2 pagesDisaster-Risk-Reduction Final Exam 2020 Grade11 The OrigelmerdlpNo ratings yet
- Ncu B1plus Extra Tasks Extension U7Document2 pagesNcu B1plus Extra Tasks Extension U7Patritsia KozhukharNo ratings yet
- Checklist MD 11Document4 pagesChecklist MD 11José Alberto CamachoNo ratings yet
- Global Warming and Climate ChangeDocument9 pagesGlobal Warming and Climate ChangeJohan Joe PaulNo ratings yet
- Disaster Readiness and Risk Reduction: Disasters From Different PerspectivesDocument27 pagesDisaster Readiness and Risk Reduction: Disasters From Different PerspectivesKayla TiquisNo ratings yet
- Disaster Preparedness and Level of AwareDocument26 pagesDisaster Preparedness and Level of AwareMerryjoy100% (1)
- How A Tsunami HappensDocument2 pagesHow A Tsunami HappensVarel ArjunaNo ratings yet
- Natural Disaster in Indonesia: Risty Khoirunisa Presentation SkillDocument11 pagesNatural Disaster in Indonesia: Risty Khoirunisa Presentation SkillRisty KhoirunisaNo ratings yet
- Pembukaan Pelatihan Inspektur Pipa PenyalurDocument9 pagesPembukaan Pelatihan Inspektur Pipa PenyaluradityaromasNo ratings yet
- Nepal Part2 Final Report 20111024044135Document125 pagesNepal Part2 Final Report 20111024044135Dinesh PoudelNo ratings yet
- Types of Disasters: Disaster ManagementDocument1 pageTypes of Disasters: Disaster ManagementqqqNo ratings yet
- Positive & Negative Effect of SocietyyyyyDocument9 pagesPositive & Negative Effect of SocietyyyyyKrize Anne CornejaNo ratings yet
- Volcanic HazardDocument28 pagesVolcanic HazardMarcus MatanguihanNo ratings yet
- BDRRMC Organizational ChartDocument1 pageBDRRMC Organizational ChartJean LebiosNo ratings yet
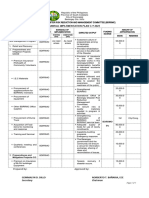
- BDRRMC 2023 Ppa 2 3 23Document2 pagesBDRRMC 2023 Ppa 2 3 23Glenn Ryan CatenzaNo ratings yet
- FTS IntroDocument2 pagesFTS IntroShreeNo ratings yet
- Icomos-Iccrom Guidance 12012024Document64 pagesIcomos-Iccrom Guidance 12012024Ipek DurukanNo ratings yet