Download as ppt, pdf, or txt
You might also like
- Unit Plan MSN OtDocument5 pagesUnit Plan MSN OtShivani Tiwari100% (1)
- Brigham 2019 MCQsDocument13 pagesBrigham 2019 MCQsfarex100% (1)
- StomatitisDocument44 pagesStomatitisNessa Layos Morillo100% (1)
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- STOMATITISDocument17 pagesSTOMATITISTeguh Adi PartamaNo ratings yet
- STOMATITISDocument12 pagesSTOMATITISninroseNo ratings yet
- MSN Question Bank-Unit 1 - Ent: Long Essay 5MDocument31 pagesMSN Question Bank-Unit 1 - Ent: Long Essay 5Mkiran kumarNo ratings yet
- Hookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilDocument5 pagesHookworm Disease: Ancylostoma Duodenale-Are Anthropophilic Human Hookworms Transmitted From Infected SoilBrix Valdriz100% (1)
- Glossitis: Farida Ulfa 15-057Document10 pagesGlossitis: Farida Ulfa 15-057farida ulfa100% (1)
- Checklist Exam of EarDocument4 pagesChecklist Exam of EarCes Melisse DNo ratings yet
- Hand Out - MalDocument11 pagesHand Out - MalRoona JayanNo ratings yet
- Osteomyelitis: ClassificationDocument5 pagesOsteomyelitis: Classificationthanuja mathewNo ratings yet
- Elimination NeedsDocument52 pagesElimination NeedsKhadija JaraNo ratings yet
- Otalgia (Ear Pain)Document43 pagesOtalgia (Ear Pain)Suzzane MNo ratings yet
- 12 Otitis MediaDocument19 pages12 Otitis MediaCabdiNo ratings yet
- Universal Immunization ProgrammeDocument3 pagesUniversal Immunization ProgrammeAmy Lalringhluani ChhakchhuakNo ratings yet
- Role of Food and Exercise in Polycystic Ovarian SyndromeDocument3 pagesRole of Food and Exercise in Polycystic Ovarian SyndromeInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Epidemiology of Non Communicable DiseaseDocument16 pagesEpidemiology of Non Communicable DiseaseAparna AbyNo ratings yet
- Esophageal CancerDocument25 pagesEsophageal CancerK poojithaNo ratings yet
- Orthopedic InjuriesDocument24 pagesOrthopedic Injuriesamber tariqNo ratings yet
- Bone Tumor: A. Nithya 1 Year M.SC (Nursing)Document46 pagesBone Tumor: A. Nithya 1 Year M.SC (Nursing)nithya nithyaNo ratings yet
- Universal Immunization ProgramDocument15 pagesUniversal Immunization Programsmruti ranjanNo ratings yet
- Case Study On Lung CancerDocument54 pagesCase Study On Lung CancerQusai BassamNo ratings yet
- Barrier NursingDocument2 pagesBarrier NursingDrPreeti Thakur Chouhan100% (1)
- SyphilisDocument54 pagesSyphilisYeyeh SantosNo ratings yet
- Assesment For Burns and Fluid Calculation PDFDocument10 pagesAssesment For Burns and Fluid Calculation PDFRagaviNo ratings yet
- Preventing Neonatal InfectionsDocument27 pagesPreventing Neonatal Infectionsmadimadi11No ratings yet
- BlepharitisDocument20 pagesBlepharitisNorshahidah IedaNo ratings yet
- Universal Immunization ProgrammeDocument8 pagesUniversal Immunization ProgrammeNagaraj ReddyNo ratings yet
- TracheostomyDocument4 pagesTracheostomySuchismita SethiNo ratings yet
- Government of Karnataka: para Medical BoardDocument40 pagesGovernment of Karnataka: para Medical BoardSrikutty DevuNo ratings yet
- SCABIESDocument14 pagesSCABIESNom Kumar Naik Rathod100% (1)
- Management of Hypersensitivity ReactionDocument6 pagesManagement of Hypersensitivity Reactionmbeng bessonganyiNo ratings yet
- CSOM TreatmentDocument21 pagesCSOM TreatmentSarwinder SinghNo ratings yet
- DiabetesDocument59 pagesDiabetesshiv gautamNo ratings yet
- Community Health One LinersDocument30 pagesCommunity Health One LinersRatan YadavNo ratings yet
- Allergic RhinitisDocument22 pagesAllergic RhinitissuciNo ratings yet
- Conjunctiva: Fourth Year Omar Al-Mukhtar Univercity 2019-2020Document55 pagesConjunctiva: Fourth Year Omar Al-Mukhtar Univercity 2019-2020Helene AlawamiNo ratings yet
- Seizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HDocument70 pagesSeizure Disorder: Presented By: Rohini Rai MSC Nursing Student College of Nursing, N.B.M.C.HRohini RaiNo ratings yet
- Riaz Gul AHN Unit 1Document106 pagesRiaz Gul AHN Unit 1Riaz Gul RindNo ratings yet
- PBBN 1St Yr Child Health Nursing CBIMNCIDocument29 pagesPBBN 1St Yr Child Health Nursing CBIMNCIcopy smart100% (1)
- Acute Suppurative Otitis MediaDocument41 pagesAcute Suppurative Otitis Mediarani suwadjiNo ratings yet
- Thalassemia: DR Husain AlmukharraqDocument9 pagesThalassemia: DR Husain AlmukharraqUm HamoOdNo ratings yet
- Normal Newborn PP Final-1Document97 pagesNormal Newborn PP Final-1ettevyviNo ratings yet
- Renal CalculiDocument9 pagesRenal Calculimehreen.alina35No ratings yet
- Cleft Lip and Cleft PalateDocument27 pagesCleft Lip and Cleft Palatenamah odatNo ratings yet
- National Aids Control ProgrammeDocument7 pagesNational Aids Control ProgrammeMUTHUKUMARANNo ratings yet
- Ophthalmia NeonatorumDocument19 pagesOphthalmia NeonatorumJisha Annie JohnNo ratings yet
- Descriptive EpidemiologyDocument7 pagesDescriptive EpidemiologyVineeta JoseNo ratings yet
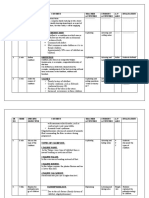
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- Oral Hygiene Word FileDocument13 pagesOral Hygiene Word FileManoj DongarwarNo ratings yet
- Esophageal ObstructionDocument18 pagesEsophageal ObstructionArun Murali50% (2)
- Kala AzarDocument37 pagesKala AzarMamata ManandharNo ratings yet
- Cogan Syndrome Surger 4, AnkitDocument18 pagesCogan Syndrome Surger 4, AnkitAnkit Tonger AnkyNo ratings yet
- History Taking and Examination of EarDocument75 pagesHistory Taking and Examination of EarShisam PoudelNo ratings yet
- ASEPSISDocument28 pagesASEPSISDeborah AmpongNo ratings yet
- Arthritis PPT For ClassDocument62 pagesArthritis PPT For ClassSaya Menang100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Stomatitis CollegeDocument14 pagesStomatitis CollegedivyaaryalNo ratings yet
- StomatitisDocument17 pagesStomatitis4A - Hazel Ann G. EspinolNo ratings yet
- Medicine: Most Recent QuestionsDocument11 pagesMedicine: Most Recent QuestionsskNo ratings yet
- What Is An Eating DisorderDocument2 pagesWhat Is An Eating Disorderthurai_rajaNo ratings yet
- Maharastra University of Health Sciences, Nashik: III M.B.B.S. MedicineDocument96 pagesMaharastra University of Health Sciences, Nashik: III M.B.B.S. Medicineanant_nimkar9243No ratings yet
- Avlosef PDFDocument4 pagesAvlosef PDFAdnan Al MahmudNo ratings yet
- Swim Class Final Exam: Mary Donahue Welcomes You To Her Home PageDocument9 pagesSwim Class Final Exam: Mary Donahue Welcomes You To Her Home PageArk KnightNo ratings yet
- Differential Diagnosis of Head and SwellingDocument41 pagesDifferential Diagnosis of Head and Swellingmachine318No ratings yet
- Eyes - Ears - Mouth - Nose (Lecture 5)Document50 pagesEyes - Ears - Mouth - Nose (Lecture 5)اسامة محمد السيد رمضانNo ratings yet
- Case Report: Large Nabothian Cyst: A Rare Cause of Nulliparous ProlapseDocument3 pagesCase Report: Large Nabothian Cyst: A Rare Cause of Nulliparous ProlapseRz Latiep Jr.No ratings yet
- Diagnosis Penyakit Dalam Bahasa InggrisDocument10 pagesDiagnosis Penyakit Dalam Bahasa InggrisPutri Sulung WidodoNo ratings yet
- Name: Melinda Hani M NIM: 2001862 Class: 1A Draft 2 Cause-Effect Mental Disorders in AdolescentsDocument7 pagesName: Melinda Hani M NIM: 2001862 Class: 1A Draft 2 Cause-Effect Mental Disorders in AdolescentsMelinda Hani MaulanaNo ratings yet
- Integrated Therapeutics IiiDocument11 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Akc and CKC Registration Certificates-MergedDocument20 pagesAkc and CKC Registration Certificates-Mergedapi-370468914No ratings yet
- EN + EosinofiliaDocument3 pagesEN + EosinofiliaAna Flavia BaptistaNo ratings yet
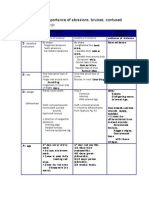
- Medico-Legal Importance of WoundsDocument3 pagesMedico-Legal Importance of Woundsapi-383014680% (5)
- Miliaria, Leucoplakia, PPPDocument44 pagesMiliaria, Leucoplakia, PPPcuteNo ratings yet
- 2003 World Health Organization (WHO) /international Society of Hypertension (ISH) Statement On Management of HypertensionDocument10 pages2003 World Health Organization (WHO) /international Society of Hypertension (ISH) Statement On Management of HypertensionGhina NisrinaNo ratings yet
- Facial PainDocument4 pagesFacial Painjaffar mahNo ratings yet
- BVGH-University of Rwanda Virtual Gynecologic Oncology CourseDocument43 pagesBVGH-University of Rwanda Virtual Gynecologic Oncology CourseEmmanuel NdikuryayoNo ratings yet
- Mastitis Presented by Bishal BhattachanDocument20 pagesMastitis Presented by Bishal BhattachanRabinNo ratings yet
- Path GitDocument18 pagesPath Gitvnair112No ratings yet
- Cambridge English For Nursing Medical Technology Intermediate Unit8 WorksheetDocument2 pagesCambridge English For Nursing Medical Technology Intermediate Unit8 WorksheetJernej LapanjeNo ratings yet
- Neurological Assessment ChartDocument5 pagesNeurological Assessment ChartshodhgangaNo ratings yet
- Short Case 1 PterygiumDocument15 pagesShort Case 1 PterygiumAnmol KhadkaNo ratings yet
- Drug Study ErythhropoietinDocument1 pageDrug Study ErythhropoietinAkiraMamoNo ratings yet
- MicrobiologyDocument5 pagesMicrobiologylamasaguiNo ratings yet
- CellulitisDocument18 pagesCellulitismuthia saniNo ratings yet
- Sigtrans20162 7608Document9 pagesSigtrans20162 7608Emalaith BlackburnNo ratings yet
- Q-NCOV-01D STANDARD Q COVID-19 IgM-IgG Duo Test INSERTODocument2 pagesQ-NCOV-01D STANDARD Q COVID-19 IgM-IgG Duo Test INSERTOechegarayNo ratings yet
- Komplikasi 2Document2 pagesKomplikasi 2Ayu PuspitaNo ratings yet