
MND
MND
You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Basic Movement Disorder ApproachDocument96 pagesBasic Movement Disorder ApproachSurat Tanprawate100% (18)
- Microbiology Chapter 17 Spring 07Document3 pagesMicrobiology Chapter 17 Spring 07fallingupward312No ratings yet
- חומר לימודי נוירולוגיה ParaparesisDocument19 pagesחומר לימודי נוירולוגיה ParaparesisAnonymous w3vYureNo ratings yet
- Spinal CordDocument7 pagesSpinal CordRemelou Garchitorena AlfelorNo ratings yet
- Medback - Cerebral PalsyDocument47 pagesMedback - Cerebral Palsyyreshgem100% (2)
- Neurology Multiple Choice Questions With Explanations: Volume IIIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIIRating: 4.5 out of 5 stars4.5/5 (6)
- Motor Neuron Disease 1Document95 pagesMotor Neuron Disease 1La Ode Rinaldi100% (1)
- Motor Neuron Diseases-Dr. IyagbaDocument29 pagesMotor Neuron Diseases-Dr. IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Tues 10-20 Peripheral Nerve Disorders - A Practical OverviewDocument37 pagesTues 10-20 Peripheral Nerve Disorders - A Practical OverviewfatehmaanNo ratings yet
- Approach To Neurological EmergenciesMAY2013Document69 pagesApproach To Neurological EmergenciesMAY2013PhaimNo ratings yet
- Tues 10-20 Peripheral Nerve Disorders - A Practical OverviewDocument36 pagesTues 10-20 Peripheral Nerve Disorders - A Practical OverviewGery FirmansyahNo ratings yet
- MOTOR NEURON DISEASE-4th Yr EU-refDocument26 pagesMOTOR NEURON DISEASE-4th Yr EU-refMalueth AnguiNo ratings yet
- Motor Neuron DiseaseDocument23 pagesMotor Neuron DiseaseNaman MishraNo ratings yet
- Current Concepts About Motr Neuron DiseaseDocument68 pagesCurrent Concepts About Motr Neuron DiseaseMuhammad MuaazNo ratings yet
- LMNL Vs UmnlDocument49 pagesLMNL Vs UmnlLohshini ManickavasagamNo ratings yet
- Peripheral Nervous System Disorders Author EknygosDocument25 pagesPeripheral Nervous System Disorders Author EknygosPredrag NikolicNo ratings yet
- Als Overview enDocument71 pagesAls Overview enkharaNo ratings yet
- Cauda-Conus SyndromesDocument28 pagesCauda-Conus Syndromessruthimeena6891No ratings yet
- Flaccid ParaparesisDocument7 pagesFlaccid ParaparesisPraptiwi 'tiw'No ratings yet
- Neuromuscular Disorders 2016Document68 pagesNeuromuscular Disorders 2016Alberto MayorgaNo ratings yet
- Lec. 2 - Spinal CordDocument14 pagesLec. 2 - Spinal CordYounus MohammedNo ratings yet
- Spinal InfectionDocument104 pagesSpinal InfectionSyarifNo ratings yet
- Diseases of The Spinal Cord by Dr. WongelDocument51 pagesDiseases of The Spinal Cord by Dr. Wongelmogesie1995No ratings yet
- Peripheral NeuropathyDocument61 pagesPeripheral NeuropathyBIAN ALKHAZMARINo ratings yet
- Penyakit Saraf TepiDocument165 pagesPenyakit Saraf TepiNasayu Nadia Santika AyuNo ratings yet
- Multiple SclerosisDocument76 pagesMultiple SclerosisAdyata DaveNo ratings yet
- Low Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTDocument41 pagesLow Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTNia Anggreni100% (1)
- Lesi Medula Spinalis Khronis AaDocument49 pagesLesi Medula Spinalis Khronis AaNisha AnggiaNo ratings yet
- Low Back Pain: Aldy S. RambeDocument40 pagesLow Back Pain: Aldy S. RambeHatta Diana TariganNo ratings yet
- EPS and Cerebellum 20Document67 pagesEPS and Cerebellum 20Шеікх АбрарNo ratings yet
- 7 Peripheral Neuropathy MyopathyDocument83 pages7 Peripheral Neuropathy Myopathymuhammadridhwan100% (1)
- Spinal Cord SyndromeDocument36 pagesSpinal Cord SyndromeSarath ChandranNo ratings yet
- Myelopathy: Dr. Astra Dea Simanungkalit, SpsDocument24 pagesMyelopathy: Dr. Astra Dea Simanungkalit, SpspppkkkNo ratings yet
- Neuro Tract Lesions Ps230114Document16 pagesNeuro Tract Lesions Ps230114সোমনাথ মহাপাত্রNo ratings yet
- Saraf Perifer: Dr. Gea Pandhita S, M.Kes, SpsDocument28 pagesSaraf Perifer: Dr. Gea Pandhita S, M.Kes, Spsludoy1No ratings yet
- STROKEDocument108 pagesSTROKELorelie Asis75% (4)
- SPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDocument84 pagesSPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- Kuliah Penyakit Sistem SARAFDocument36 pagesKuliah Penyakit Sistem SARAFAnonymous U9KX2cMNo ratings yet
- Amyotrophic Lateral SclerosisDocument15 pagesAmyotrophic Lateral Sclerosisyamie sulongNo ratings yet
- Spinal Deformities (Congenital)Document27 pagesSpinal Deformities (Congenital)deathmetal017No ratings yet
- Neuropathy Peroneal Neuropathy: Lily Runtuwene SMF Saraf Rsud Ulin BanjarmasinDocument44 pagesNeuropathy Peroneal Neuropathy: Lily Runtuwene SMF Saraf Rsud Ulin Banjarmasincici chairunisaNo ratings yet
- Kelainan Saraf KongenitalDocument35 pagesKelainan Saraf KongenitalTitisNo ratings yet
- Spinal Cord DisordersDocument50 pagesSpinal Cord DisordersIsaac Mwangi100% (1)
- Multiple Sclerosis OfficialDocument20 pagesMultiple Sclerosis OfficialJerin XavierNo ratings yet
- Radicular Syndrome Kuliah BlokDocument32 pagesRadicular Syndrome Kuliah BlokChRist LumingkewasNo ratings yet
- Radicular Syndrome Kuliah BlokDocument32 pagesRadicular Syndrome Kuliah BlokNisha AnggiaNo ratings yet
- How To Localize Neurological LesionDocument25 pagesHow To Localize Neurological LesionBeenish IqbalNo ratings yet
- Radicular SyndromeDocument40 pagesRadicular Syndromeainulhawa89No ratings yet
- Cerebral Palsy BrieflyDocument50 pagesCerebral Palsy BrieflymeenoNo ratings yet
- Peripheral Neuropathy HandoutDocument16 pagesPeripheral Neuropathy HandoutTatiana IonascuNo ratings yet
- Motor Neuron DiseasesDocument103 pagesMotor Neuron DiseasesJamil AhmadNo ratings yet
- Ataxia: Pediatric Neurology Quick TalksDocument18 pagesAtaxia: Pediatric Neurology Quick TalksAlex GasnasNo ratings yet
- Neurology XXXXDocument13 pagesNeurology XXXXAmeer AslamNo ratings yet
- LocalizationDocument38 pagesLocalizationWilson HannahNo ratings yet
- Motor Neuron Disease Afrath AbdullahDocument20 pagesMotor Neuron Disease Afrath AbdullahfidaNo ratings yet
- NeuropatiDocument19 pagesNeuropatiBochand CoolNo ratings yet
- Low Back Pain: Dr. Suherman, SP.SDocument27 pagesLow Back Pain: Dr. Suherman, SP.SArmiya MiaowNo ratings yet
- Low Back Pain: Dr. Suherman, SP.SDocument27 pagesLow Back Pain: Dr. Suherman, SP.Sنذر الدينNo ratings yet
- Extrapyramidal System and CerebellumDocument52 pagesExtrapyramidal System and CerebellumVictoriiaNo ratings yet
- ANATOMY PHYSIOLOGY Cardiovascular SystemDocument12 pagesANATOMY PHYSIOLOGY Cardiovascular SystemPuji PrisylNo ratings yet
- Nervous SystemDocument34 pagesNervous SystemAlmiah Alfarouk100% (1)
- Fetal Morphological and Physiological Development PDFDocument10 pagesFetal Morphological and Physiological Development PDFKim RamosNo ratings yet
- Pex 09 02Document4 pagesPex 09 02Haleigh TomaselloNo ratings yet
- Respiration NotesDocument4 pagesRespiration NotesJana AldourNo ratings yet
- General Arrangement of The Abdominal VisceraDocument30 pagesGeneral Arrangement of The Abdominal Visceraapi-249972919100% (2)
- U4 L4 LessonPlan 0Document19 pagesU4 L4 LessonPlan 0Joe Marie A MendozaNo ratings yet
- AO Spine PDFDocument4 pagesAO Spine PDFGabriela Ballestero ContrerasNo ratings yet
- Histology of Female Reproductive SystemDocument11 pagesHistology of Female Reproductive SystemYoshua AdhisaktiNo ratings yet
- 3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFDocument151 pages3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFMauzoom Ali100% (2)
- Maxillary Transverse DeficiencyDocument4 pagesMaxillary Transverse DeficiencyCarlos Alberto CastañedaNo ratings yet
- Brain AnatomyDocument22 pagesBrain AnatomyMédecin Adrian TGNo ratings yet
- Impression Techniques For Implant Dentistry (Part 2) : Open Tray TechniquesDocument5 pagesImpression Techniques For Implant Dentistry (Part 2) : Open Tray TechniquesIJAR JOURNALNo ratings yet
- Science 5 DLP 1 Human Reproductive SystemDocument12 pagesScience 5 DLP 1 Human Reproductive SystemDyaan TrajicoNo ratings yet
- Biology (Excretion Nephron)Document12 pagesBiology (Excretion Nephron)7a4374 hisNo ratings yet
- The Physiological Changes of PregnancyDocument16 pagesThe Physiological Changes of PregnancycchaitukNo ratings yet
- Post Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistryDocument5 pagesPost Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistrySharon LawNo ratings yet
- Removable Appliances Author DR Lamis Khidher MohammedDocument11 pagesRemovable Appliances Author DR Lamis Khidher MohammedRuxandra FitaNo ratings yet
- Transportation in Animals and Plants 1 2Document15 pagesTransportation in Animals and Plants 1 2DEVMONo ratings yet
- Generic Name Brand Name Drug Class Mechanism of Action StructureDocument4 pagesGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoNo ratings yet
- Nephrology - Dr. Allam 2021Document42 pagesNephrology - Dr. Allam 2021Alokh Saha RajNo ratings yet
- Cosmetic Dentistry CSD 2013Document3 pagesCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNo ratings yet
- Rat DissectionDocument7 pagesRat Dissectionapi-236289588No ratings yet
- External Carotid ArteryDocument80 pagesExternal Carotid Arterybaba bunnyNo ratings yet
- FSG332 Cardiovascular Pathophysiology 3 - 2Document39 pagesFSG332 Cardiovascular Pathophysiology 3 - 2Huzaifa KhanNo ratings yet
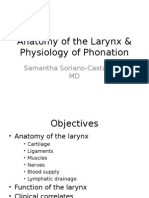
- 05.12 Anatomy of The Larynx & Physiology of PhonationDocument30 pages05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNo ratings yet
- Komatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop ManualDocument22 pagesKomatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop Manualmorganthomas160591ekr100% (66)
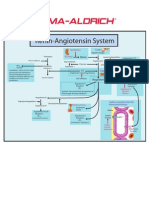
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Alpacas Physical Exam PosterDocument1 pageAlpacas Physical Exam PosterJesse LindellNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- Neurology Multiple Choice Questions With Explanations: Volume IFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IRating: 4 out of 5 stars4/5 (7)
- Basic Movement Disorder ApproachDocument96 pagesBasic Movement Disorder ApproachSurat Tanprawate100% (18)
- Microbiology Chapter 17 Spring 07Document3 pagesMicrobiology Chapter 17 Spring 07fallingupward312No ratings yet
- חומר לימודי נוירולוגיה ParaparesisDocument19 pagesחומר לימודי נוירולוגיה ParaparesisAnonymous w3vYureNo ratings yet
- Spinal CordDocument7 pagesSpinal CordRemelou Garchitorena AlfelorNo ratings yet
- Medback - Cerebral PalsyDocument47 pagesMedback - Cerebral Palsyyreshgem100% (2)
- Neurology Multiple Choice Questions With Explanations: Volume IIIFrom EverandNeurology Multiple Choice Questions With Explanations: Volume IIIRating: 4.5 out of 5 stars4.5/5 (6)
- Motor Neuron Disease 1Document95 pagesMotor Neuron Disease 1La Ode Rinaldi100% (1)
- Motor Neuron Diseases-Dr. IyagbaDocument29 pagesMotor Neuron Diseases-Dr. IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Tues 10-20 Peripheral Nerve Disorders - A Practical OverviewDocument37 pagesTues 10-20 Peripheral Nerve Disorders - A Practical OverviewfatehmaanNo ratings yet
- Approach To Neurological EmergenciesMAY2013Document69 pagesApproach To Neurological EmergenciesMAY2013PhaimNo ratings yet
- Tues 10-20 Peripheral Nerve Disorders - A Practical OverviewDocument36 pagesTues 10-20 Peripheral Nerve Disorders - A Practical OverviewGery FirmansyahNo ratings yet
- MOTOR NEURON DISEASE-4th Yr EU-refDocument26 pagesMOTOR NEURON DISEASE-4th Yr EU-refMalueth AnguiNo ratings yet
- Motor Neuron DiseaseDocument23 pagesMotor Neuron DiseaseNaman MishraNo ratings yet
- Current Concepts About Motr Neuron DiseaseDocument68 pagesCurrent Concepts About Motr Neuron DiseaseMuhammad MuaazNo ratings yet
- LMNL Vs UmnlDocument49 pagesLMNL Vs UmnlLohshini ManickavasagamNo ratings yet
- Peripheral Nervous System Disorders Author EknygosDocument25 pagesPeripheral Nervous System Disorders Author EknygosPredrag NikolicNo ratings yet
- Als Overview enDocument71 pagesAls Overview enkharaNo ratings yet
- Cauda-Conus SyndromesDocument28 pagesCauda-Conus Syndromessruthimeena6891No ratings yet
- Flaccid ParaparesisDocument7 pagesFlaccid ParaparesisPraptiwi 'tiw'No ratings yet
- Neuromuscular Disorders 2016Document68 pagesNeuromuscular Disorders 2016Alberto MayorgaNo ratings yet
- Lec. 2 - Spinal CordDocument14 pagesLec. 2 - Spinal CordYounus MohammedNo ratings yet
- Spinal InfectionDocument104 pagesSpinal InfectionSyarifNo ratings yet
- Diseases of The Spinal Cord by Dr. WongelDocument51 pagesDiseases of The Spinal Cord by Dr. Wongelmogesie1995No ratings yet
- Peripheral NeuropathyDocument61 pagesPeripheral NeuropathyBIAN ALKHAZMARINo ratings yet
- Penyakit Saraf TepiDocument165 pagesPenyakit Saraf TepiNasayu Nadia Santika AyuNo ratings yet
- Multiple SclerosisDocument76 pagesMultiple SclerosisAdyata DaveNo ratings yet
- Low Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTDocument41 pagesLow Back Pain: Dr. Andi Dhedie P. Sam, M.Kes, SP - OTNia Anggreni100% (1)
- Lesi Medula Spinalis Khronis AaDocument49 pagesLesi Medula Spinalis Khronis AaNisha AnggiaNo ratings yet
- Low Back Pain: Aldy S. RambeDocument40 pagesLow Back Pain: Aldy S. RambeHatta Diana TariganNo ratings yet
- EPS and Cerebellum 20Document67 pagesEPS and Cerebellum 20Шеікх АбрарNo ratings yet
- 7 Peripheral Neuropathy MyopathyDocument83 pages7 Peripheral Neuropathy Myopathymuhammadridhwan100% (1)
- Spinal Cord SyndromeDocument36 pagesSpinal Cord SyndromeSarath ChandranNo ratings yet
- Myelopathy: Dr. Astra Dea Simanungkalit, SpsDocument24 pagesMyelopathy: Dr. Astra Dea Simanungkalit, SpspppkkkNo ratings yet
- Neuro Tract Lesions Ps230114Document16 pagesNeuro Tract Lesions Ps230114সোমনাথ মহাপাত্রNo ratings yet
- Saraf Perifer: Dr. Gea Pandhita S, M.Kes, SpsDocument28 pagesSaraf Perifer: Dr. Gea Pandhita S, M.Kes, Spsludoy1No ratings yet
- STROKEDocument108 pagesSTROKELorelie Asis75% (4)
- SPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDocument84 pagesSPINAL CORD SYNDROMES by Dr. Monday Jacob ZaccheausDr. Amb. Monday ZaccheausNo ratings yet
- Kuliah Penyakit Sistem SARAFDocument36 pagesKuliah Penyakit Sistem SARAFAnonymous U9KX2cMNo ratings yet
- Amyotrophic Lateral SclerosisDocument15 pagesAmyotrophic Lateral Sclerosisyamie sulongNo ratings yet
- Spinal Deformities (Congenital)Document27 pagesSpinal Deformities (Congenital)deathmetal017No ratings yet
- Neuropathy Peroneal Neuropathy: Lily Runtuwene SMF Saraf Rsud Ulin BanjarmasinDocument44 pagesNeuropathy Peroneal Neuropathy: Lily Runtuwene SMF Saraf Rsud Ulin Banjarmasincici chairunisaNo ratings yet
- Kelainan Saraf KongenitalDocument35 pagesKelainan Saraf KongenitalTitisNo ratings yet
- Spinal Cord DisordersDocument50 pagesSpinal Cord DisordersIsaac Mwangi100% (1)
- Multiple Sclerosis OfficialDocument20 pagesMultiple Sclerosis OfficialJerin XavierNo ratings yet
- Radicular Syndrome Kuliah BlokDocument32 pagesRadicular Syndrome Kuliah BlokChRist LumingkewasNo ratings yet
- Radicular Syndrome Kuliah BlokDocument32 pagesRadicular Syndrome Kuliah BlokNisha AnggiaNo ratings yet
- How To Localize Neurological LesionDocument25 pagesHow To Localize Neurological LesionBeenish IqbalNo ratings yet
- Radicular SyndromeDocument40 pagesRadicular Syndromeainulhawa89No ratings yet
- Cerebral Palsy BrieflyDocument50 pagesCerebral Palsy BrieflymeenoNo ratings yet
- Peripheral Neuropathy HandoutDocument16 pagesPeripheral Neuropathy HandoutTatiana IonascuNo ratings yet
- Motor Neuron DiseasesDocument103 pagesMotor Neuron DiseasesJamil AhmadNo ratings yet
- Ataxia: Pediatric Neurology Quick TalksDocument18 pagesAtaxia: Pediatric Neurology Quick TalksAlex GasnasNo ratings yet
- Neurology XXXXDocument13 pagesNeurology XXXXAmeer AslamNo ratings yet
- LocalizationDocument38 pagesLocalizationWilson HannahNo ratings yet
- Motor Neuron Disease Afrath AbdullahDocument20 pagesMotor Neuron Disease Afrath AbdullahfidaNo ratings yet
- NeuropatiDocument19 pagesNeuropatiBochand CoolNo ratings yet
- Low Back Pain: Dr. Suherman, SP.SDocument27 pagesLow Back Pain: Dr. Suherman, SP.SArmiya MiaowNo ratings yet
- Low Back Pain: Dr. Suherman, SP.SDocument27 pagesLow Back Pain: Dr. Suherman, SP.Sنذر الدينNo ratings yet
- Extrapyramidal System and CerebellumDocument52 pagesExtrapyramidal System and CerebellumVictoriiaNo ratings yet
- ANATOMY PHYSIOLOGY Cardiovascular SystemDocument12 pagesANATOMY PHYSIOLOGY Cardiovascular SystemPuji PrisylNo ratings yet
- Nervous SystemDocument34 pagesNervous SystemAlmiah Alfarouk100% (1)
- Fetal Morphological and Physiological Development PDFDocument10 pagesFetal Morphological and Physiological Development PDFKim RamosNo ratings yet
- Pex 09 02Document4 pagesPex 09 02Haleigh TomaselloNo ratings yet
- Respiration NotesDocument4 pagesRespiration NotesJana AldourNo ratings yet
- General Arrangement of The Abdominal VisceraDocument30 pagesGeneral Arrangement of The Abdominal Visceraapi-249972919100% (2)
- U4 L4 LessonPlan 0Document19 pagesU4 L4 LessonPlan 0Joe Marie A MendozaNo ratings yet
- AO Spine PDFDocument4 pagesAO Spine PDFGabriela Ballestero ContrerasNo ratings yet
- Histology of Female Reproductive SystemDocument11 pagesHistology of Female Reproductive SystemYoshua AdhisaktiNo ratings yet
- 3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFDocument151 pages3600+ Review Questions For Anatomy & Physiology Volume 2 - (4th Edition) PDFMauzoom Ali100% (2)
- Maxillary Transverse DeficiencyDocument4 pagesMaxillary Transverse DeficiencyCarlos Alberto CastañedaNo ratings yet
- Brain AnatomyDocument22 pagesBrain AnatomyMédecin Adrian TGNo ratings yet
- Impression Techniques For Implant Dentistry (Part 2) : Open Tray TechniquesDocument5 pagesImpression Techniques For Implant Dentistry (Part 2) : Open Tray TechniquesIJAR JOURNALNo ratings yet
- Science 5 DLP 1 Human Reproductive SystemDocument12 pagesScience 5 DLP 1 Human Reproductive SystemDyaan TrajicoNo ratings yet
- Biology (Excretion Nephron)Document12 pagesBiology (Excretion Nephron)7a4374 hisNo ratings yet
- The Physiological Changes of PregnancyDocument16 pagesThe Physiological Changes of PregnancycchaitukNo ratings yet
- Post Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistryDocument5 pagesPost Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistrySharon LawNo ratings yet
- Removable Appliances Author DR Lamis Khidher MohammedDocument11 pagesRemovable Appliances Author DR Lamis Khidher MohammedRuxandra FitaNo ratings yet
- Transportation in Animals and Plants 1 2Document15 pagesTransportation in Animals and Plants 1 2DEVMONo ratings yet
- Generic Name Brand Name Drug Class Mechanism of Action StructureDocument4 pagesGeneric Name Brand Name Drug Class Mechanism of Action StructurenoelkiddoNo ratings yet
- Nephrology - Dr. Allam 2021Document42 pagesNephrology - Dr. Allam 2021Alokh Saha RajNo ratings yet
- Cosmetic Dentistry CSD 2013Document3 pagesCosmetic Dentistry CSD 2013Rodrigo Daniel Vela RiveraNo ratings yet
- Rat DissectionDocument7 pagesRat Dissectionapi-236289588No ratings yet
- External Carotid ArteryDocument80 pagesExternal Carotid Arterybaba bunnyNo ratings yet
- FSG332 Cardiovascular Pathophysiology 3 - 2Document39 pagesFSG332 Cardiovascular Pathophysiology 3 - 2Huzaifa KhanNo ratings yet
- 05.12 Anatomy of The Larynx & Physiology of PhonationDocument30 pages05.12 Anatomy of The Larynx & Physiology of PhonationReg LagartejaNo ratings yet
- Komatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop ManualDocument22 pagesKomatsu Hydraulic Excavator Pc4000 11 t4 Deu Gzeam08246 1 Shop Manualmorganthomas160591ekr100% (66)
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Alpacas Physical Exam PosterDocument1 pageAlpacas Physical Exam PosterJesse LindellNo ratings yet