Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Zero To Finals MedicineDocument352 pagesZero To Finals MedicinePlay100% (25)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- NBME FORM 26-AnswersDocument52 pagesNBME FORM 26-Answersmed student50% (8)
- Irene Gold Associates - Part II & IIIDocument84 pagesIrene Gold Associates - Part II & IIIAndrew Calderone100% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- Plabverse AllDocument316 pagesPlabverse AllFahad IqbalNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Cardiology Board Review 2E Mar 21 2023 - 1119814944 - Wiley Blackwell Ramdas G Pai Full ChapterDocument51 pagesCardiology Board Review 2E Mar 21 2023 - 1119814944 - Wiley Blackwell Ramdas G Pai Full Chapterdouglas.zimmer226100% (19)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Section 1. True/False Questions: Written Test No.1Document7 pagesSection 1. True/False Questions: Written Test No.1Anonymous fQAeGFNo ratings yet
- Building Our Future by Sharing Our KnowledgeDocument40 pagesBuilding Our Future by Sharing Our KnowledgeAnonymous fQAeGFNo ratings yet
- Air Comp PortDocument1 pageAir Comp PortAnonymous fQAeGFNo ratings yet
- Gear Guide2Document50 pagesGear Guide2Anonymous fQAeGFNo ratings yet
- Torque Is A Force Which Produces, or Tends To Produce Rotation. Power Torque X Speed. Torque Force X Moment ArmDocument4 pagesTorque Is A Force Which Produces, or Tends To Produce Rotation. Power Torque X Speed. Torque Force X Moment ArmAnonymous fQAeGFNo ratings yet
- Gear Guide2Document50 pagesGear Guide2Anonymous fQAeGFNo ratings yet
- Methods Minimize Gear BacklashDocument6 pagesMethods Minimize Gear BacklashAnonymous fQAeGFNo ratings yet
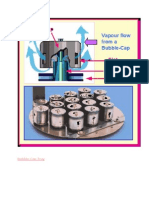
- Bubble Cap TrayDocument3 pagesBubble Cap TrayAnonymous fQAeGFNo ratings yet
- Difference Between Pipe and TubeDocument3 pagesDifference Between Pipe and TubeAnonymous fQAeGFNo ratings yet
- VPDocument7 pagesVPAnonymous fQAeGFNo ratings yet
- Pipes: ASME/ANSI B 36.10 Welded and Seamless Wrought Steel PipeDocument2 pagesPipes: ASME/ANSI B 36.10 Welded and Seamless Wrought Steel PipeAnonymous fQAeGFNo ratings yet
- D. Crowley, 2007Document16 pagesD. Crowley, 2007Anonymous fQAeGFNo ratings yet
- Catalysts in The Petrochemical IndustryDocument6 pagesCatalysts in The Petrochemical IndustryAnonymous fQAeGFNo ratings yet
- IHRDC E-Learning Solutions Detailed CatalogDocument515 pagesIHRDC E-Learning Solutions Detailed CatalogjjelwartNo ratings yet
- SealSDocument63 pagesSealSAnonymous fQAeGFNo ratings yet
- D. Crowley, 2007Document16 pagesD. Crowley, 2007Anonymous fQAeGFNo ratings yet
- Cooling Tower PowerpointDocument17 pagesCooling Tower PowerpointAnonymous fQAeGFNo ratings yet
- Introduction To Synchronous BeltsDocument63 pagesIntroduction To Synchronous BeltsAnonymous fQAeGFNo ratings yet
- Shell and Tube Heat ExchangerDocument23 pagesShell and Tube Heat ExchangerEslam EsooNo ratings yet
- 00 Obs&Gyn Clerkship-1-1Document9 pages00 Obs&Gyn Clerkship-1-1samwel daniel100% (1)
- Ventricular Septal DefectDocument16 pagesVentricular Septal DefectPai PAiNo ratings yet
- Cardiology WorkBookDocument102 pagesCardiology WorkBookCastleKGNo ratings yet
- CHF FC III Ec Mitral StenosisDocument36 pagesCHF FC III Ec Mitral Stenosisbroken18bear100% (1)
- PCU 200 Handbook 2018-19 PDFDocument177 pagesPCU 200 Handbook 2018-19 PDFVica CapatinaNo ratings yet
- April 2009Document19 pagesApril 2009PROGNAS HIV RSBWNo ratings yet
- Gilad Surgery QuestionsDocument96 pagesGilad Surgery Questionsqlrjqlejr100% (1)
- Sample Transes 2Document11 pagesSample Transes 2Sophia SalamatNo ratings yet
- PediatricDocument55 pagesPediatricJade Q Osit100% (6)
- Bates' Guide To Physical Examination and History Taking, 12th EditionDocument14 pagesBates' Guide To Physical Examination and History Taking, 12th EditionmanesNo ratings yet
- Zanki (Complete) + R/medicalschoolanki Microbiology ErrataDocument70 pagesZanki (Complete) + R/medicalschoolanki Microbiology ErrataedNo ratings yet
- Emma Holliday Surgery Notes - Cornell StyleDocument299 pagesEmma Holliday Surgery Notes - Cornell StyleBanana MuffinNo ratings yet
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- Secrets of PacesDocument162 pagesSecrets of PacesMohammadAbdurRahman0% (1)
- 1-7 Levick and Dwight - CardiovascularDocument7 pages1-7 Levick and Dwight - Cardiovascularrahmawati aliwarmanNo ratings yet
- Mnemonic PharmaDocument13 pagesMnemonic Pharmamanoj kumarNo ratings yet
- CHD2 - DR Shirley L ADocument74 pagesCHD2 - DR Shirley L ARaihan Luthfi100% (1)
- CCU Clinical GuidelinesDocument63 pagesCCU Clinical GuidelinesHAMMYER ALROKHAMINo ratings yet
- Sebastian Zeki - The Illustrated MRCP PACES Primer (MasterPass) - CRC Press (2009)Document167 pagesSebastian Zeki - The Illustrated MRCP PACES Primer (MasterPass) - CRC Press (2009)Achyut KanungoNo ratings yet
- Blood Pressure and SoundDocument45 pagesBlood Pressure and SoundRamanathan SunderNo ratings yet
- Cardiac Surgery & Cardiology MCQsDocument18 pagesCardiac Surgery & Cardiology MCQssb medex100% (1)
- Kathynotes PDFDocument103 pagesKathynotes PDFvarrakeshNo ratings yet
- Complete Transposition of Great ArteriesDocument85 pagesComplete Transposition of Great ArteriesRahul AgrawalNo ratings yet
- Deskripsi MurmurDocument3 pagesDeskripsi MurmurLevina Tri RatanaNo ratings yet
- Practice MCQ On Heart Sounds and ECGDocument8 pagesPractice MCQ On Heart Sounds and ECGnithin shenoi100% (2)