Download as ppt, pdf, or txt
You might also like
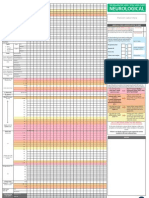
- Adult Early Warning Score Observation Chart For Neurosurgical UnitDocument1 pageAdult Early Warning Score Observation Chart For Neurosurgical UnitalexipsNo ratings yet
- The Breuss Cancer Cure PDF Ebook Free Download - Rudolf BreussDocument140 pagesThe Breuss Cancer Cure PDF Ebook Free Download - Rudolf Breusspdf ebook free download90% (21)
- Medicine in Brief: Name the Disease in Haiku, Tanka and ArtFrom EverandMedicine in Brief: Name the Disease in Haiku, Tanka and ArtRating: 5 out of 5 stars5/5 (1)
- Malt MINI Neuropsychiatric InterviewDocument31 pagesMalt MINI Neuropsychiatric Interviewelvinegunawan50% (2)
- Valvular Heart Disease Medical Surgical NursingDocument75 pagesValvular Heart Disease Medical Surgical NursingGodfrey Franco88% (8)
- Bush-Francis Catatonia Rating ScaleDocument2 pagesBush-Francis Catatonia Rating ScalePsiquiatria PraticaNo ratings yet
- PEBC Evaluating Exam Mustpass Misbah 2016 PDFDocument437 pagesPEBC Evaluating Exam Mustpass Misbah 2016 PDFKathryn Mitchell100% (3)
- Congenital Heart DefectsDocument73 pagesCongenital Heart DefectsStaen KisNo ratings yet
- PAEDs - CVS-1Document44 pagesPAEDs - CVS-1Priscah bhokeNo ratings yet
- Inflammatory and Valvular DisordersDocument43 pagesInflammatory and Valvular DisordersRifqi Hary ZulfikarNo ratings yet
- Congenital Heart DiseasesDocument121 pagesCongenital Heart DiseasesJayvee V. De GuzmanNo ratings yet
- Penyakit Jantung KongenitalDocument30 pagesPenyakit Jantung KongenitalrintiikNo ratings yet
- Congenital Heart DiseasesDocument27 pagesCongenital Heart DiseasesJumar ValdezNo ratings yet
- Lecture 17a VHDDocument70 pagesLecture 17a VHDKishan ArrumugamNo ratings yet
- Valvular Heart Disease. KulDocument67 pagesValvular Heart Disease. KulDebyAntatifaniRitongaNo ratings yet
- Cardio 2024Document42 pagesCardio 2024Salameh AtrashNo ratings yet
- Penyakit Jantung Kongenital - TikaDocument43 pagesPenyakit Jantung Kongenital - Tikatika martikaNo ratings yet
- Cardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134Document38 pagesCardiovascular Function: Marquez, Spencer T. BSN Iii, Block Iv NCM 114, N134hayascent hilarioNo ratings yet
- Week 6 Disturbances in CirculationDocument83 pagesWeek 6 Disturbances in CirculationHans CortezNo ratings yet
- Ebstein's Anomaly: Department of Cardiovascular and Thoracic Surgery Sarit Levinsky Group M1656Document36 pagesEbstein's Anomaly: Department of Cardiovascular and Thoracic Surgery Sarit Levinsky Group M1656Sarit LevinskyNo ratings yet
- Valvular Heart DiseaseDocument42 pagesValvular Heart DiseaseareeparambilNo ratings yet
- Valvular Heart DiseaseDocument55 pagesValvular Heart Diseaseapi-19916399No ratings yet
- Valvular & Inflammatory HDDocument33 pagesValvular & Inflammatory HDSinam SinghaNo ratings yet
- Cardiovascular Diseases VSD Asd 2022 1Document16 pagesCardiovascular Diseases VSD Asd 2022 1Boyu GrtrNo ratings yet
- Acyanotic CHD-obstructiveDocument39 pagesAcyanotic CHD-obstructiveEbuka AniNo ratings yet
- 01 Cardiovascular IDocument72 pages01 Cardiovascular IcoriezaNo ratings yet
- ucu-CHDs 240114 230618Document68 pagesucu-CHDs 240114 230618BrianNo ratings yet
- #5 Neonatal Cardiac AnomaliesDocument93 pages#5 Neonatal Cardiac AnomaliesSittie Hania100% (2)
- Adult Congenital Heart Disease Board ReviewDocument76 pagesAdult Congenital Heart Disease Board ReviewOQAB13No ratings yet
- Cvs BCMDocument117 pagesCvs BCMjaniceli0207No ratings yet
- Congenital Heart Diseases Practical Approach in Children With Heart MurmurDocument51 pagesCongenital Heart Diseases Practical Approach in Children With Heart Murmurdennyyy175No ratings yet
- 9, CHF BestDocument43 pages9, CHF BestauNo ratings yet
- Neonatology #30-41Document36 pagesNeonatology #30-41Daanish KhorasaniNo ratings yet
- Heart FailureDocument77 pagesHeart FailureJudy Anne PatricioNo ratings yet
- Penyakit Jantung Bawaan - IDocument44 pagesPenyakit Jantung Bawaan - IEkisliefvirjou Adelihira HidraNo ratings yet
- Heart DefectDocument41 pagesHeart Defectdevutty 123No ratings yet
- Cyanotic Heart DiseaseDocument66 pagesCyanotic Heart DiseasePrasanth SankarNo ratings yet
- CardiologyDocument43 pagesCardiologyhasanatiya41No ratings yet
- CARDIOMYOPATHIESDocument80 pagesCARDIOMYOPATHIESNadun MethwadaneNo ratings yet
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Adult Congenital Heart Disease Board ReviewDocument79 pagesAdult Congenital Heart Disease Board ReviewKhajornsak Som-UnNo ratings yet
- Congenital Heart DiseaseDocument60 pagesCongenital Heart DiseaseBonfaceNo ratings yet
- Acyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianDocument98 pagesAcyanotic Heart Disease& Fetal Circulation: Guided By, Dr.K.Sivakanthan Consultant PaediatricianVijayakanth VijayakumarNo ratings yet
- Cardiovascular PathologyDocument182 pagesCardiovascular PathologyPavan chowdaryNo ratings yet
- Cardio-Comprehensive: - AnatomyDocument51 pagesCardio-Comprehensive: - AnatomyAshamdeep AntaalNo ratings yet
- Valvular Heart Disease. KulDocument60 pagesValvular Heart Disease. KulIntan Kumalasari RambeNo ratings yet
- Pda TofDocument56 pagesPda TofPritam PanigrahiNo ratings yet
- Ductus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCDocument28 pagesDuctus Arteriosus Dependent Congenital Heart Disease: Amjad Kouatli MD. FAAP. FACCKartik KumarasamyNo ratings yet
- Peripheral Arterial DiseaseDocument38 pagesPeripheral Arterial DiseaseRessy HastoprajaNo ratings yet
- Cardio-Respiratory Conditions: by DR Priscus MushiDocument73 pagesCardio-Respiratory Conditions: by DR Priscus MushiMusaNo ratings yet
- Fitz Cardiology Paces NotesDocument26 pagesFitz Cardiology Paces NotesMuhammad BilalNo ratings yet
- 7 MCC Cianogene - Medici PDFDocument101 pages7 MCC Cianogene - Medici PDFAnca MehedintuNo ratings yet
- Congenital Heart DiseaseDocument135 pagesCongenital Heart DiseaseMahmudahNo ratings yet
- Ischemic Heart Disease and Myocardial InfarctionDocument73 pagesIschemic Heart Disease and Myocardial InfarctionAngelEduardoVillarrealGiraldoNo ratings yet
- Pediatric Congenital Heart DiseaseDocument95 pagesPediatric Congenital Heart DiseaseShikya AbnasNo ratings yet
- Valvular Heart Disease: Joko AnggoroDocument53 pagesValvular Heart Disease: Joko AnggoroReza SatriaNo ratings yet
- Pericarditis: Dr. Alfredo Gonzales SaavedraDocument38 pagesPericarditis: Dr. Alfredo Gonzales SaavedraSandy Burgos CabanillasNo ratings yet
- Critical Congenital Heart Disease: Early Detection and ManagementDocument29 pagesCritical Congenital Heart Disease: Early Detection and ManagementtyesNo ratings yet
- Cardiovascular Diseases FinalDocument119 pagesCardiovascular Diseases FinalabhieghailNo ratings yet
- AnginaDocument43 pagesAnginaMuhammad Ashraf AhmadNo ratings yet
- Congenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekDocument43 pagesCongenital Heart Diseases: Charles University of Prague 2 Faculty of Medicine Filip KoubekAdel HamzicNo ratings yet
- Cardiovascular DisorderDocument40 pagesCardiovascular DisorderAmy Del CarmenNo ratings yet
- 3 - Valvular Heart DiseasesDocument31 pages3 - Valvular Heart DiseasesLobna ElkilanyNo ratings yet
- #2 Headache DestroyerDocument47 pages#2 Headache DestroyerBruce rNo ratings yet
- Research Article: ISSN: 0975-833XDocument6 pagesResearch Article: ISSN: 0975-833XMd Byzed AhmedNo ratings yet
- B. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseDocument4 pagesB. 11 Situation - Care of Client With Problems in Inflammatory & Immunologic ResponseSOLEIL LOUISE LACSON MARBAS100% (1)
- Tumour Markers: An Overview: T. MalatiDocument15 pagesTumour Markers: An Overview: T. Malatigoretushar1No ratings yet
- Kode Penyakit BPJS 2020Document3 pagesKode Penyakit BPJS 2020norma yanaNo ratings yet
- Health Teaching PlanDocument3 pagesHealth Teaching PlanJoshua Villarba100% (2)
- 4 5920472882638490310 Removed RemovedDocument97 pages4 5920472882638490310 Removed Removedsameena vNo ratings yet
- Allergic RhinitisDocument19 pagesAllergic RhinitisNicole Villaflor FabicoNo ratings yet
- Acute Respiratory InfectionsDocument34 pagesAcute Respiratory InfectionssafiebuttNo ratings yet
- NCP Colon CancerDocument8 pagesNCP Colon CancerSkyla FiestaNo ratings yet
- Lung AbscessDocument2 pagesLung Abscessoxidalaj100% (1)
- Cervical Lymphoepithelial CystDocument6 pagesCervical Lymphoepithelial CystAhmed Al-jumailiNo ratings yet
- Study of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)Document2 pagesStudy of Coagulation Profile in Type 2 Diabetes Mellitus Patients in Correlation With Long Term Glycemic Control (Hba1c)IJAR JOURNALNo ratings yet
- Anaplastic Sarcoma of The Kidney With Chromosomal AbnormalityDocument5 pagesAnaplastic Sarcoma of The Kidney With Chromosomal AbnormalityJose Alejandro InciongNo ratings yet
- 23coronary Artery DiseaseDocument10 pages23coronary Artery DiseaseZiedTrikiNo ratings yet
- H ': P P C N - GCNC: Irschsprung S Disease Re and Ostoperative Are in EonatesDocument12 pagesH ': P P C N - GCNC: Irschsprung S Disease Re and Ostoperative Are in EonatesAnonymous 18GsyXbNo ratings yet
- Pediatric NursinggDocument13 pagesPediatric NursinggShalina RizalNo ratings yet
- KRDXDocument3 pagesKRDXMark John Dela CruzNo ratings yet
- Acute Pulmonaryl Edema, Hypotension, Shock AlgorithmDocument2 pagesAcute Pulmonaryl Edema, Hypotension, Shock AlgorithmTrustia RizqandaruNo ratings yet
- Conjunctivitis - UpToDateDocument18 pagesConjunctivitis - UpToDateu201416371No ratings yet
- Classification of Chronic PainDocument238 pagesClassification of Chronic PainFebyan Abot100% (1)
- Phlebothrombosis: Azole, I. (2021) - PHLEBOTHROMBOSIS. - PPT Download. Retrieved 25 October 2021, FromDocument1 pagePhlebothrombosis: Azole, I. (2021) - PHLEBOTHROMBOSIS. - PPT Download. Retrieved 25 October 2021, FromSureen RegularNo ratings yet
- Disorders of The Vulva - Common Causes of Vulvar Pain, Burning, and Itching - ACOGDocument7 pagesDisorders of The Vulva - Common Causes of Vulvar Pain, Burning, and Itching - ACOGAYI NURHIDAYAHNo ratings yet
- Lewis Heart Failure Care PlanDocument4 pagesLewis Heart Failure Care Plansarahbearcoups100% (1)
- DocumentDocument6 pagesDocumentkrishcelNo ratings yet