Download as pptx, pdf, or txt
You might also like
- Medical Background - Cerebral PalsyDocument10 pagesMedical Background - Cerebral PalsyMervyn Orbe100% (1)
- Cervical MusculatureDocument3 pagesCervical Musculaturesimone dumbrellNo ratings yet
- Upper Limb: Organization FunctionDocument33 pagesUpper Limb: Organization FunctionAhmed Nabiel El-Jaliel100% (1)
- Lower Limb: Muscle Charts: Cheat Sheet (English Terminology)Document9 pagesLower Limb: Muscle Charts: Cheat Sheet (English Terminology)yinose7198No ratings yet
- MC Case PDFDocument20 pagesMC Case PDFShivani KarkeraNo ratings yet
- 120lab Report 3Document4 pages120lab Report 3Valerie Mae Librero Areño100% (2)
- BBS Book (PT 14) NeglyDocument7 pagesBBS Book (PT 14) Neglyapi-3871208No ratings yet
- Cranial Nerve 6, 7 and 8 (Short Presentation)Document33 pagesCranial Nerve 6, 7 and 8 (Short Presentation)3uvpNo ratings yet
- The Upper Extremity: Sufitni Megasari SitorusDocument37 pagesThe Upper Extremity: Sufitni Megasari SitorusFakhrur RaziNo ratings yet
- Table of Lower Limb MusclesDocument7 pagesTable of Lower Limb MusclesAmirah Balqis Muhammad IzaniNo ratings yet
- Vertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar ArteryDocument6 pagesVertebral Arteries, and Their Divisions. Arteries Fuse To Form The Basilar Arterymurali_bharadwazNo ratings yet
- Cerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiDocument71 pagesCerebellum and Brain Stem: DR Asim Shrestha SRCC Ped Neuro Fellow MumbaiAsim ShresthaNo ratings yet
- Lab 14Document14 pagesLab 14Lueshen Wellington100% (1)
- Triangles of Neck (Anatomy)Document36 pagesTriangles of Neck (Anatomy)Dr Tahira Nihal100% (1)
- List of Muscles and ActionsDocument8 pagesList of Muscles and ActionsGiacen0% (1)
- კუნთებიDocument6 pagesკუნთებიPlay ListNo ratings yet
- Upper LimbDocument31 pagesUpper LimbNandhana Kattuparambil SunojNo ratings yet
- Anatomy Digestive SystemDocument6 pagesAnatomy Digestive Systempearl042008No ratings yet
- Elbow JointDocument12 pagesElbow Jointbpt2No ratings yet
- Anatomy of The SpineDocument61 pagesAnatomy of The SpineAnonymous 9XDi2Yqa0% (2)
- Brain CisternsDocument44 pagesBrain CisternsRam Kirubakar Thangaraj100% (1)
- Hip Joint: Important PointsDocument4 pagesHip Joint: Important PointsNamrah AfzalNo ratings yet
- PONSDocument40 pagesPONSveegeer100% (1)
- Arm and ForearmDocument4 pagesArm and ForearmANIS MUNIRAH BINTI MOHD ARSHAD -No ratings yet
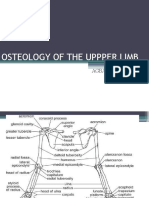
- Osteology of Upper LimbDocument63 pagesOsteology of Upper LimbAkomolede AbosedeNo ratings yet
- Muscles of The Back PDFDocument4 pagesMuscles of The Back PDFjsdlzjNo ratings yet
- Anterior Triangle of The Neck IIDocument49 pagesAnterior Triangle of The Neck IIvrajNo ratings yet
- D. Brainstem: PONS (Ventral Metencephalon) 1. External Consideration A. Ventral ViewDocument39 pagesD. Brainstem: PONS (Ventral Metencephalon) 1. External Consideration A. Ventral ViewMarvic SueltoNo ratings yet
- Upper Limb Muscle AttachmentDocument7 pagesUpper Limb Muscle Attachmenterwilli5No ratings yet
- Nerve Injuries of Upper Limb: Dr. Mujahid KhanDocument41 pagesNerve Injuries of Upper Limb: Dr. Mujahid KhanElton Ndhlovu100% (1)
- MUSCLES OINA LavarnDocument20 pagesMUSCLES OINA LavarnStray KidsNo ratings yet
- Anatomy MnemonicsDocument51 pagesAnatomy MnemonicsDrKhawarfarooq SundhuNo ratings yet
- Thorax AllDocument174 pagesThorax Allravindra sharmaNo ratings yet
- Gross Anatomy of Posterior Compartment of The ThighDocument20 pagesGross Anatomy of Posterior Compartment of The ThighOnah ArinzeNo ratings yet
- Upper ExtremityDocument216 pagesUpper ExtremityChester VergilNo ratings yet
- Blood Supply of The BrainDocument55 pagesBlood Supply of The BrainueumanaNo ratings yet
- Dr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyDocument55 pagesDr. Reynaldo V. Lopez Senior Lecturer Department of AnatomyMohammad AliNo ratings yet
- Upper Limb, Pectoral RegionDocument24 pagesUpper Limb, Pectoral Regiongtaha80No ratings yet
- Lower Limb & HipDocument9 pagesLower Limb & HipENo ratings yet
- Abdomen: By: DR Tegene Gizaw (MD)Document202 pagesAbdomen: By: DR Tegene Gizaw (MD)abdishakurNo ratings yet
- Anatomy of AbdomenDocument15 pagesAnatomy of AbdomenarunmptNo ratings yet
- Oculomotor Nerve: Components Main Action SuppliesDocument10 pagesOculomotor Nerve: Components Main Action Suppliesdisha1990No ratings yet
- Sensations and Sensory Pathways General Senses Test Procedure Normal Result Abnormal Result Clinical InterpretationDocument5 pagesSensations and Sensory Pathways General Senses Test Procedure Normal Result Abnormal Result Clinical InterpretationAbby MataNo ratings yet
- Anatomy of Knee JointDocument17 pagesAnatomy of Knee JointSiti AisyahNo ratings yet
- Lower Limb MusclesDocument8 pagesLower Limb Musclesbilal_kmu020% (1)
- Anatomy RevisionDocument172 pagesAnatomy RevisionHannah KarlNo ratings yet
- Orbit - AnatomyDocument41 pagesOrbit - Anatomysamuelpnrj25100% (2)
- Elbow JointDocument64 pagesElbow JointolumNo ratings yet
- Blood Supply of The BrainDocument11 pagesBlood Supply of The Brainneleh grayNo ratings yet
- Brainstem (Yuni)Document34 pagesBrainstem (Yuni)Ayi Abdul Basith100% (2)
- Rom MMT Trunk Study Sheet 1Document3 pagesRom MMT Trunk Study Sheet 1api-242889989No ratings yet
- Joint of Lower LimbDocument16 pagesJoint of Lower LimbZA ID100% (1)
- Brainstem (Pons, Medulla, Midbrain) : Dr. MariaDocument23 pagesBrainstem (Pons, Medulla, Midbrain) : Dr. MariaMuhammad Mustaqeem100% (1)
- PONS: NeuroanatomyDocument20 pagesPONS: NeuroanatomyHassan IlyasNo ratings yet
- Nerve Injury of Upper LimbDocument41 pagesNerve Injury of Upper LimbbashirjnmcNo ratings yet
- Spinal Cord LesionsDocument110 pagesSpinal Cord Lesionsgtaha80100% (1)
- Nerves of Upper LimbDocument24 pagesNerves of Upper LimbShimmering MoonNo ratings yet
- Lecture On The Histology of Cerebrum and Meninges by Dr. RoomiDocument20 pagesLecture On The Histology of Cerebrum and Meninges by Dr. RoomiMudassar Roomi100% (1)
- Flashcards - Lower LimbDocument6 pagesFlashcards - Lower LimbKhanNo ratings yet
- Brachial Plexus: Summary Mnemonics Clinical RelationsDocument19 pagesBrachial Plexus: Summary Mnemonics Clinical RelationsGulmehr NoorNo ratings yet
- @CNSMedicalBook ThoraxDocument103 pages@CNSMedicalBook ThoraxGemechis Merga100% (1)
- A Simple Guide to Cerebral Aneurysm, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Cerebral Aneurysm, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Thyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandThyroglossal Duct Cysts, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- UntitledDocument14 pagesUntitlednaresh kumarNo ratings yet
- Functional Specification For Deck CraneDocument31 pagesFunctional Specification For Deck Craneaiyubi20% (1)
- HT Billing System - May'2022Document2 pagesHT Billing System - May'2022V.Sampath RaoNo ratings yet
- Perdev Module 3Document13 pagesPerdev Module 3Renelyn JacoNo ratings yet
- Air Track Gizmo - ExploreLearningDocument4 pagesAir Track Gizmo - ExploreLearningJeremy Gomez-RojasNo ratings yet
- Gennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's IndianDocument130 pagesGennady Nesis, Leonid Shulman, Malcolm Gesthuysen - Tactics in The King's Indiancodonauta100% (1)
- Behaviour of Hollow Core Slabs Under Point LoadsDocument17 pagesBehaviour of Hollow Core Slabs Under Point LoadsVálter LúcioNo ratings yet
- Intensifying AdjectivesDocument2 pagesIntensifying AdjectivesReena JimmyNo ratings yet
- Describe Physical and Chemical Change OperationallyDocument2 pagesDescribe Physical and Chemical Change OperationallyMaria Anna GraciaNo ratings yet
- Business Presentation YAKULTDocument12 pagesBusiness Presentation YAKULTJosuaNo ratings yet
- BDA 542 V3 - powerCON TRUE 1 TOP - NAC3MX-W-TOPDocument2 pagesBDA 542 V3 - powerCON TRUE 1 TOP - NAC3MX-W-TOPluis manuelNo ratings yet
- Jayvee Dime,,,,project in Physics Light and SoundDocument25 pagesJayvee Dime,,,,project in Physics Light and SoundJayvee DimeNo ratings yet
- Mouser TestsectionDocument33 pagesMouser TestsectionalltheloveintheworldNo ratings yet
- BEL PE Question Papers For ECE With Answers - 6 Knowledge AddaDocument14 pagesBEL PE Question Papers For ECE With Answers - 6 Knowledge AddaVishwanand ThombareNo ratings yet
- Da0bl7mb6d0 Rev DDocument44 pagesDa0bl7mb6d0 Rev DFerreira da CunhaNo ratings yet
- TSB-1139 8SC Wiring DiagramDocument2 pagesTSB-1139 8SC Wiring Diagramxavier marsNo ratings yet
- Question: Consider A Point in A Structural Member That Is Subjected To PLDocument1 pageQuestion: Consider A Point in A Structural Member That Is Subjected To PLTekin EnerjiNo ratings yet
- Kohima Nagaland LBDocument1 pageKohima Nagaland LBIndia TreadingNo ratings yet
- (A) Design - Introduction To Transformer DesignDocument16 pages(A) Design - Introduction To Transformer DesignZineddine BENOUADAHNo ratings yet
- Hybrid Vehicle A Study On Technology IJERTV3IS120917 PDFDocument8 pagesHybrid Vehicle A Study On Technology IJERTV3IS120917 PDFAshish MathurNo ratings yet
- CSC 2701 - CalculusDocument5 pagesCSC 2701 - CalculusMd Rubaiyat BhuiyanNo ratings yet
- Ultimate GuideDocument11 pagesUltimate GuideIgor SucevicNo ratings yet
- Hillfoot Data Sheets V5 1Document4 pagesHillfoot Data Sheets V5 1Kristijan IlicNo ratings yet
- TDS 0033 FlexoTop 202003Document3 pagesTDS 0033 FlexoTop 202003Mearg NgusseNo ratings yet
- Minireview: C-Reactive ProteinDocument4 pagesMinireview: C-Reactive ProteinFernando Amblódegui GarcíaNo ratings yet
- Straumann Product Catalogue 2018 2019Document260 pagesStraumann Product Catalogue 2018 2019kllasikalleNo ratings yet
- AbseilingDocument12 pagesAbseilingMurah Rezeki Cikgu WafiNo ratings yet