Download as ppt, pdf, or txt
You might also like
- Grade 8 Lesson - MitosisDocument3 pagesGrade 8 Lesson - MitosisBerliese Frias93% (28)
- Ab Initio Interview QuestionsDocument3 pagesAb Initio Interview QuestionsRatika Miglani MalhotraNo ratings yet
- Med PPT Pneumonia For LectureDocument67 pagesMed PPT Pneumonia For LectureManisanthosh Kumar100% (1)
- Photography + Videography: Pricelist MenuDocument12 pagesPhotography + Videography: Pricelist MenuChacha TasyaNo ratings yet
- Entreprenuership Notes (Full)Document230 pagesEntreprenuership Notes (Full)Izo Serem78% (9)
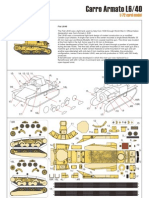
- Kampfflieger Italian AFV'sDocument2 pagesKampfflieger Italian AFV'sLaduss100% (4)
- History of Special EducationDocument5 pagesHistory of Special EducationCyra MandigmaNo ratings yet
- Acute Liver FailureDocument69 pagesAcute Liver FailureAsif.N.IqbalNo ratings yet
- DIABETIC COMA - Clinical Features and ManagementDocument54 pagesDIABETIC COMA - Clinical Features and ManagementRitesh SinghNo ratings yet
- Acute Liver FailureDocument78 pagesAcute Liver FailurePankaj IngleNo ratings yet
- Department of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Document51 pagesDepartment of Internal Medicine III Aortic Stenosis: - Rajkumar Subasaravanan Subgroup "12"Suba Saravanan 12No ratings yet
- Cirrhosis of LiverDocument106 pagesCirrhosis of LiveraahadNo ratings yet
- Cardiogenic Shock: Sparsh Goel 77Document28 pagesCardiogenic Shock: Sparsh Goel 77Sparsh GoelNo ratings yet
- Acute Kidney Injury DR Moses KazevuDocument52 pagesAcute Kidney Injury DR Moses KazevuMoses Jr KazevuNo ratings yet
- Heart Failure With Preserved Ejection FractionDocument19 pagesHeart Failure With Preserved Ejection Fractioncosmin balanNo ratings yet
- Acute Kidney InjuryDocument60 pagesAcute Kidney InjuryAbegail Fermanejo-GeneraoNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart FailureBella Trix PagdangananNo ratings yet
- Hypertension LecturesDocument65 pagesHypertension LecturesAdebisiNo ratings yet
- Pleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicineDocument52 pagesPleural Effusion: Dr.S.Sesha Sai (MD), Pulmonary MedicinevaishnaviNo ratings yet
- I. A. Brief Description: Chakinala, 2015)Document54 pagesI. A. Brief Description: Chakinala, 2015)Kacelyn QuibanNo ratings yet
- Cirrhosis of LiverDocument35 pagesCirrhosis of LiverShazia Parveen100% (1)
- Cerebrovascular AccidentDocument31 pagesCerebrovascular AccidentRam ReddyNo ratings yet
- Atrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhDocument45 pagesAtrial Fibrillation: Discussed by - DR Kunwar Sidharth SaurabhKunwar Sidharth SaurabhNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Asthama & COPDDocument84 pagesAsthama & COPDAbdullah BhattiNo ratings yet
- Chronic Obstructive Disease by HibaDocument38 pagesChronic Obstructive Disease by HibahibaNo ratings yet
- Pulmonary EmbolismDocument70 pagesPulmonary Embolismalhindhy.gNo ratings yet
- Hypokalaemia and HyperkalaemiaDocument39 pagesHypokalaemia and HyperkalaemiaRZ NgNo ratings yet
- Myocardialinfarction 150223043527 Conversion Gate02 PDFDocument22 pagesMyocardialinfarction 150223043527 Conversion Gate02 PDFBhavika Aggarwal100% (1)
- Coronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdDocument99 pagesCoronary Artery Disease-Cad OR Ischaemic Heart Disease - IhdMwanja MosesNo ratings yet
- Pulmonary EmbolismDocument61 pagesPulmonary Embolismjhk0428No ratings yet
- Pulmonary EdemaDocument47 pagesPulmonary Edemamaeliszxc kimNo ratings yet
- Acute Respiratory FailureDocument25 pagesAcute Respiratory FailureDyah Putri0% (1)
- Nephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HDocument60 pagesNephrotic Syndrome: Jaiganesh.M, M.D (General Medicine) Asst. Professor, S.M.C.HJaiganesh MuruganandamNo ratings yet
- Ngaji Arrythmia Cordis 3Document122 pagesNgaji Arrythmia Cordis 3Dhita Dwi NandaNo ratings yet
- Isabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderDocument15 pagesIsabela State University City of Ilagan Campus: Care of The Clients With Endocrine and Metabolic DisorderCharlz ZipaganNo ratings yet
- Acute Liver FailureDocument3 pagesAcute Liver FailureElisabeth F. OjhaNo ratings yet
- The Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiDocument32 pagesThe Lower Respiratory Tract Infection: Pneumonia: Ida Bagus Ngurah RaiFelicia adeline ChristianNo ratings yet
- Cardiomyopathy: Imtiyaz Ali Lecturer, UTARDocument31 pagesCardiomyopathy: Imtiyaz Ali Lecturer, UTARSalman KhanNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- Rheumatoid Arthritis and Acute Rheumatic FeverDocument76 pagesRheumatoid Arthritis and Acute Rheumatic FeverM. O. PHC HOLAVANAHALLYNo ratings yet
- Liver Cirrhosis LectureDocument83 pagesLiver Cirrhosis LectureSheila Regina Tiza100% (1)
- AnemiaDocument71 pagesAnemiaAnsu MaliyakalNo ratings yet
- Glomerulonephritis PresentationDocument23 pagesGlomerulonephritis Presentationjacksonyu1234No ratings yet
- Chronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDDocument32 pagesChronic Kidney Disease: Disampaikan Oleh: Wilda Maula Miftah Nur Aknowledgement: Dr. Mia Melinda, SP - PDErryz JogjuzzNo ratings yet
- The Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocDocument60 pagesThe Pneumonias: Associate Professor Dr. Lauren Ţiu ŞorodocCristina Georgiana CoticăNo ratings yet
- Pathogenesis of Micro and Macrovascular Complications of DiabetesDocument4 pagesPathogenesis of Micro and Macrovascular Complications of DiabetesFrancesca LiNo ratings yet
- Evaluation of Liver FunctionDocument64 pagesEvaluation of Liver FunctionMustafa KhandgawiNo ratings yet
- Nephrotic SyndromeDocument24 pagesNephrotic SyndromeJawad SaleemNo ratings yet
- Normal Sinus RhythmDocument97 pagesNormal Sinus RhythmNatasha LiberisNo ratings yet
- Risk Stratification in CVD Prevention: How To Identify Cardiovascular Risk in The OfficeDocument28 pagesRisk Stratification in CVD Prevention: How To Identify Cardiovascular Risk in The OfficeJuwanto Wakimin100% (1)
- Nephrotic Syndrome 2016Document45 pagesNephrotic Syndrome 2016alaaNo ratings yet
- Pleural EffusionDocument51 pagesPleural EffusionMinhajul IslamNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument161 pagesChronic Obstructive Pulmonary DiseaseClarisse Nicole TanNo ratings yet
- CASE PRESENTATION ON U AnginaDocument40 pagesCASE PRESENTATION ON U AnginaSafoora RafeeqNo ratings yet
- Neurological Manifestations of HIVDocument34 pagesNeurological Manifestations of HIVashuNo ratings yet
- Congestive Heart FailureDocument43 pagesCongestive Heart Failure568563100% (1)
- Haematology Physical ExaminationDocument8 pagesHaematology Physical Examinationrodahlyu100% (1)
- Asthma DR Moses KazevuDocument25 pagesAsthma DR Moses KazevuMoses Jr KazevuNo ratings yet
- Cardiogenic ShockDocument20 pagesCardiogenic Shockanimesh pandaNo ratings yet
- "Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareDocument51 pages"Pulmonary Hypertension": Jimmy Ford, MD Pulmonary and Critical CareSohil ElfarNo ratings yet
- Dr. Sana Bashir DPT, MS-CPPTDocument46 pagesDr. Sana Bashir DPT, MS-CPPTbkdfiesefll100% (1)
- Acute Kidney InjuryDocument64 pagesAcute Kidney InjuryBIAN ALKHAZMARINo ratings yet
- Cardiac TamponadeDocument10 pagesCardiac TamponadeRahmi Fatma SariNo ratings yet
- Preventive CardiologyDocument28 pagesPreventive CardiologyerizonNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Referat Penatalaksanaan Pada Gangguan BipolarDocument1 pageReferat Penatalaksanaan Pada Gangguan BipolarChacha TasyaNo ratings yet
- Maxillofacial Trauma: PG TutorialDocument113 pagesMaxillofacial Trauma: PG TutorialChacha TasyaNo ratings yet
- Valvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityDocument46 pagesValvular Heart Disease: Cardiology Division, Medical Faculty Diponegoro UniversityChacha TasyaNo ratings yet
- Cardiac Rhythm: DR - Dr. Sugiri, SPPD, SPJPDocument16 pagesCardiac Rhythm: DR - Dr. Sugiri, SPPD, SPJPChacha TasyaNo ratings yet
- GA22 API464139 Parts ManualDocument100 pagesGA22 API464139 Parts ManualAlisha Lynn Lacoursiere100% (1)
- Political Economy of Uganda - Course OutlineDocument4 pagesPolitical Economy of Uganda - Course OutlineKISAKYE MOSESNo ratings yet
- Brand Engagement With Brand ExpressionDocument27 pagesBrand Engagement With Brand ExpressionArun KCNo ratings yet
- Prayer MeetingDocument17 pagesPrayer MeetingMerceditha F. LidasanNo ratings yet
- EDQM - 2024 Subscription To The European Pharmacopoeia - Supplements 11.3-11.5 - Direct Clients - Price ListDocument2 pagesEDQM - 2024 Subscription To The European Pharmacopoeia - Supplements 11.3-11.5 - Direct Clients - Price Listbrunekas49No ratings yet
- Operating Systems: Chapter 3 - ProcessesDocument57 pagesOperating Systems: Chapter 3 - ProcessesM Fayez KhanNo ratings yet
- Dan Guerrero's Emails On Steve Alford - Part 2Document479 pagesDan Guerrero's Emails On Steve Alford - Part 2Joe PiechowskiNo ratings yet
- Starting Up Notes (1-2-3-4) .Document2 pagesStarting Up Notes (1-2-3-4) .JHIMY PAREDESNo ratings yet
- Mit Commercial Real Estate Analysis and Investment Online Short Program BrochureDocument9 pagesMit Commercial Real Estate Analysis and Investment Online Short Program BrochureJennifer LeeNo ratings yet
- Big DataDocument20 pagesBig DataBhavnita NareshNo ratings yet
- Hussain Sagar - WikipediaDocument6 pagesHussain Sagar - WikipediaNikhil PallamreddyNo ratings yet
- Temple Architecture Case StudyDocument27 pagesTemple Architecture Case StudySuren Adithyaa (RA1911201010043)100% (1)
- Tranfer PF Anand PDFDocument2 pagesTranfer PF Anand PDFShubham ChoudharyNo ratings yet
- Marketing Research ProcessDocument3 pagesMarketing Research Processadnan saifNo ratings yet
- Factiva 20180604 1444Document131 pagesFactiva 20180604 1444Lucas GodeiroNo ratings yet
- Adobe Fill & SignDocument1 pageAdobe Fill & SignBobby TaysonNo ratings yet
- NET Lab ManualDocument32 pagesNET Lab ManualMadhu Sudan100% (1)
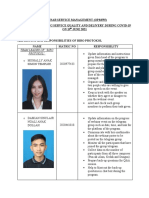
- Report Opm555 - Biro Protokol (Revamped)Document3 pagesReport Opm555 - Biro Protokol (Revamped)shaza noordinNo ratings yet
- HamiltonianRatingScaleforDepression (HAM D)Document2 pagesHamiltonianRatingScaleforDepression (HAM D)Shirley Pigott MDNo ratings yet
- MGBS Plans PDFDocument4 pagesMGBS Plans PDFvivekvardhanNo ratings yet
- D'Herbigny. Vladimir Soloviev - A Russian Newman (1918)Document285 pagesD'Herbigny. Vladimir Soloviev - A Russian Newman (1918)Blaise09No ratings yet
- Manual AirBagDocument36 pagesManual AirBagРоман КабрицкийNo ratings yet
- Exercises Past Simple To Be PDFDocument2 pagesExercises Past Simple To Be PDFGonzaloNo ratings yet
- Bibliografía RazaDocument3 pagesBibliografía RazaJorge Vallejo KazacosNo ratings yet