Download as ppt, pdf, or txt
You might also like
- BIO102 Practice ExamDocument10 pagesBIO102 Practice ExamKathy YuNo ratings yet
- Steel Works Inc - Case StudyDocument24 pagesSteel Works Inc - Case Studymwaqasiqbal100% (1)
- CaseanalysisDocument2 pagesCaseanalysisChrislyn Dian Pene100% (1)
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Running Head: CASE STUDY PAPER 1Document14 pagesRunning Head: CASE STUDY PAPER 1Issaiah Nicolle CeciliaNo ratings yet
- ManKiw Chapter 11 Solutions ProblemsDocument3 pagesManKiw Chapter 11 Solutions ProblemsKev10767% (3)
- Aplastic Anemia Lecture 1aDocument39 pagesAplastic Anemia Lecture 1aniaaseta100% (2)
- Anemia 101-Case StudiesDocument20 pagesAnemia 101-Case StudiesZamharira MuslimNo ratings yet
- Pancytopenia and Aplastic Anemia OkDocument33 pagesPancytopenia and Aplastic Anemia OkIrina MoldovanNo ratings yet
- Aplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreDocument26 pagesAplastic Anaemia: DR Sandeep M R Physician Jayanagar General Hospial BangaloreSandeep m rNo ratings yet
- Myelodysplastic Syndrome (MDS)Document61 pagesMyelodysplastic Syndrome (MDS)Tusabe FredNo ratings yet
- 9a. Red Cell DisordersDocument46 pages9a. Red Cell DisordersMuhammad DaviqNo ratings yet
- Keganasan HematologiDocument69 pagesKeganasan HematologiRuki HartawanNo ratings yet
- Aplastic AnemiaDocument29 pagesAplastic AnemiaAshish SoniNo ratings yet
- Hemolytic UpdatedDocument48 pagesHemolytic UpdatedRamses GamingNo ratings yet
- Acute Leukemia C2Document67 pagesAcute Leukemia C2ahmed mohammedNo ratings yet
- Anemia Workshop1Document80 pagesAnemia Workshop1api-3762917No ratings yet
- Aplastic AnemiaDocument21 pagesAplastic AnemiaMichelle Vera GabunNo ratings yet
- Catastrophic APSDocument24 pagesCatastrophic APSJiayu YangNo ratings yet
- Handout 2 1522436248 PDFDocument82 pagesHandout 2 1522436248 PDFHarnadi WonogiriNo ratings yet
- Aplastic Anemia: A Case Study OnDocument10 pagesAplastic Anemia: A Case Study OnVidge GrospeNo ratings yet
- 5 Myeloproliferative NeoplasmsDocument49 pages5 Myeloproliferative NeoplasmsEliza Stanescu100% (1)
- Frequency of Hypersplenism in Chronic Liver Disease Patients Presenting With PancytopeniaDocument3 pagesFrequency of Hypersplenism in Chronic Liver Disease Patients Presenting With Pancytopeniaamal johnsonNo ratings yet
- Dr. Yusra Rashid Haematology Department University of Health SciencesDocument40 pagesDr. Yusra Rashid Haematology Department University of Health SciencesMahmood AtharNo ratings yet
- Acute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllDocument64 pagesAcute Myelogenous Leukemia-Aml Acute Lymphoblastic Leukemia - AllSiraj ShiferawNo ratings yet
- Thrombocytopenia Sarah WalterDocument49 pagesThrombocytopenia Sarah WalterSupicha VichaiditNo ratings yet
- Churg-Strauss Syndrome: Dispelling The MythsDocument18 pagesChurg-Strauss Syndrome: Dispelling The MythsJoss VaNo ratings yet
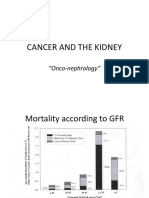
- Cancer and The KidneyDocument29 pagesCancer and The Kidney[ qιlα ]No ratings yet
- The Management of Pulmonary Small Vessel VasculitidesDocument61 pagesThe Management of Pulmonary Small Vessel VasculitidesJindal Chest ClinicNo ratings yet
- Hemolytic Uremic Syndrome: Prof. Pediatric Nephrology Sindh Institute of Urology & Transplanatation PakistanDocument111 pagesHemolytic Uremic Syndrome: Prof. Pediatric Nephrology Sindh Institute of Urology & Transplanatation PakistanDr. Mir Uzair HashmiNo ratings yet
- Case 11 Presentation - FinalDocument47 pagesCase 11 Presentation - FinalKristin HarrisNo ratings yet
- Autoimmune HepatitisDocument41 pagesAutoimmune HepatitisMigi Pradysta100% (1)
- Acute Myeloid LeukemiaDocument29 pagesAcute Myeloid LeukemiaMohammad Fadel Satriansyah100% (1)
- Leukopenia and Bone Marrow TransplantationDocument20 pagesLeukopenia and Bone Marrow Transplantationdhanya jayanNo ratings yet
- Antiphospholipid Syndrome Nephropathy in Patients With Systemic Lupus Erythematosus and Antiphospholipid AntibodiesDocument11 pagesAntiphospholipid Syndrome Nephropathy in Patients With Systemic Lupus Erythematosus and Antiphospholipid AntibodiesdhineyNo ratings yet
- Klinis Anemia PpdgsDocument48 pagesKlinis Anemia PpdgsSuryaAtmajayaNo ratings yet
- MyelomaDocument40 pagesMyelomaHula HulahulagNo ratings yet
- Plasma Cell NeoplasmsDocument36 pagesPlasma Cell Neoplasmsdrafq2000No ratings yet
- Leukamia and Transfusion MedicineDocument26 pagesLeukamia and Transfusion MedicineSamuel kuriaNo ratings yet
- Kidney CancerDocument31 pagesKidney CancerEfren Elico VenguaNo ratings yet
- Aplastic AnemiaDocument16 pagesAplastic Anemiairfan fadilahNo ratings yet
- Case Study - Leukemia2Document4 pagesCase Study - Leukemia2shaiya08No ratings yet
- Bone Marrow Failure 2008-09Document15 pagesBone Marrow Failure 2008-09Karan BhattNo ratings yet
- Solid Organ Transplantation - Basic ConceptsDocument41 pagesSolid Organ Transplantation - Basic Conceptsmxg3merNo ratings yet
- Anemia and Critical CareDocument77 pagesAnemia and Critical Carehunter_axl010% (1)
- Acute Kidney InjuryDocument42 pagesAcute Kidney Injurymedpedshospitalist100% (1)
- 5.15 SepsisDocument44 pages5.15 SepsisOnSolomonNo ratings yet
- Mod9Week2 - PA 3306 - Aug 28& Sept1Document46 pagesMod9Week2 - PA 3306 - Aug 28& Sept1komal sheikhNo ratings yet
- Anemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewDocument15 pagesAnemias Aplastic Anemia Is A Condition Where Bone Marrow Does Not Produce Sufficient NewZoreyca RiveraNo ratings yet
- ASH Hematology Review Series - AML - Sallman D - 6-2022Document60 pagesASH Hematology Review Series - AML - Sallman D - 6-2022Иван НегарэNo ratings yet
- Acute LeukemiasDocument48 pagesAcute LeukemiaslaibaNo ratings yet
- AML Pita DR MardiahDocument71 pagesAML Pita DR MardiahSarly Puspita AriesaNo ratings yet
- Leucemias Agudas: Kenny Mauricio Galvez HematologiaDocument62 pagesLeucemias Agudas: Kenny Mauricio Galvez HematologiaMichelle Ocampo ValenciaNo ratings yet
- Hypoalbuminemia and LymphocytopeniaDocument5 pagesHypoalbuminemia and LymphocytopeniaAleksandar VučićNo ratings yet
- Case Study Output Aplastic AnemiaDocument7 pagesCase Study Output Aplastic AnemiaColeen Angelique MontenegroNo ratings yet
- USMLE Step 3 Answers To ARCHER Q Bank 1-25Document15 pagesUSMLE Step 3 Answers To ARCHER Q Bank 1-25rashmiajNo ratings yet
- Acute Renal Failure: Anthony R Mato, MDDocument81 pagesAcute Renal Failure: Anthony R Mato, MDasad_channa1No ratings yet
- Null 1Document49 pagesNull 1ImamAbdyNo ratings yet
- Journal Reading: "Aplastic Anemia: Current Concepts in Diagnosis and Management"Document21 pagesJournal Reading: "Aplastic Anemia: Current Concepts in Diagnosis and Management"Nurfadilah SyamNo ratings yet
- Anemia Aplastik: Presentan: Tika Adilistya Pembimbing: Prof. Dr. Riadi Wirawan, SPPK (K)Document36 pagesAnemia Aplastik: Presentan: Tika Adilistya Pembimbing: Prof. Dr. Riadi Wirawan, SPPK (K)Tika AdilistyaNo ratings yet
- Kuliah Path Clin MSK 2017Document26 pagesKuliah Path Clin MSK 2017LioraNo ratings yet
- PBL Vii Fix BeetDocument33 pagesPBL Vii Fix BeetNUR AFRI NINGSIHNo ratings yet
- 1 Plasmapheresis - 1Document61 pages1 Plasmapheresis - 1sayednour100% (1)
- SQL CommandDocument2 pagesSQL CommandA Rah ULNo ratings yet
- 1 - DS SATK Form - Initial Application of LTO 1.2Document4 pages1 - DS SATK Form - Initial Application of LTO 1.2cheska yahniiNo ratings yet
- CVAsikin (Project Engineer)Document13 pagesCVAsikin (Project Engineer)Anonymous j6AXjDKNo ratings yet
- Greek Lentil and Spinach SoupDocument3 pagesGreek Lentil and Spinach SouppudroNo ratings yet
- BIMDocument15 pagesBIMAhmed AbdelMaksoud100% (1)
- Guidelinefor CentreSuperintendentPrac9.02.2013Document120 pagesGuidelinefor CentreSuperintendentPrac9.02.2013JasmineNo ratings yet
- Drama 30 Year Plan RittingerDocument2 pagesDrama 30 Year Plan Rittingerapi-490177257No ratings yet
- Principles of Marketing: Creating and Capturing Customer ValueDocument17 pagesPrinciples of Marketing: Creating and Capturing Customer ValueBusiswa MsiphanyanaNo ratings yet
- MonographDocument38 pagesMonographNicolocoNo ratings yet
- QM ZG528 Ec-2r Second Sem 2021-2022Document1 pageQM ZG528 Ec-2r Second Sem 2021-2022shahul hameedNo ratings yet
- Declaration Form Autocop PDFDocument3 pagesDeclaration Form Autocop PDFAman DeepNo ratings yet
- SHS Sy2021-2022 Q3law W1-2 General-Chemistry-ValidatedDocument8 pagesSHS Sy2021-2022 Q3law W1-2 General-Chemistry-Validatedjohnrobertdeocampo84No ratings yet
- Basic Electrical Installation Work Four TDocument2 pagesBasic Electrical Installation Work Four TNimas AfinaNo ratings yet
- Iso 30400-2016Document12 pagesIso 30400-2016Shekhar100% (3)
- Navya MVH HCQDocument13 pagesNavya MVH HCQhosur mvNo ratings yet
- Power Supply ATX Enclosed 250 Watt 3.3VDCDocument8 pagesPower Supply ATX Enclosed 250 Watt 3.3VDCsiogNo ratings yet
- Telecom Resource Planning Tool - Brochure - Apr 09Document12 pagesTelecom Resource Planning Tool - Brochure - Apr 09brajesh_er1709No ratings yet
- Piping Material Specification - Tsmto 99fu M 99 Pt0 001 Rev0!3!65Document64 pagesPiping Material Specification - Tsmto 99fu M 99 Pt0 001 Rev0!3!65epbamdad100% (1)
- The Implementation of FOC For PMSM Drive Based On TMS320F28035 DSP ControllerDocument5 pagesThe Implementation of FOC For PMSM Drive Based On TMS320F28035 DSP ControllerJashan BelagurNo ratings yet
- PNC Infratech Limited Bags Rs.233 Crore PWD Road Project in UP (Company Update)Document2 pagesPNC Infratech Limited Bags Rs.233 Crore PWD Road Project in UP (Company Update)Shyam SunderNo ratings yet
- GTNetS ManualDocument148 pagesGTNetS ManualJatin JaniNo ratings yet
- Daihatsu Gensets Diesel EngineDocument20 pagesDaihatsu Gensets Diesel Enginexyz1002100% (1)
- Date - 1 - 9 - 2024 Time - 8 - 42 - 56 - 850Document1 pageDate - 1 - 9 - 2024 Time - 8 - 42 - 56 - 850ANKUSH 87205312No ratings yet
- Astm D4Document3 pagesAstm D4Vijayan Munuswamy100% (1)
- Pricerfileinterfacespecification Pfi4Document34 pagesPricerfileinterfacespecification Pfi4nthgrNo ratings yet
- Honda DAXDocument12 pagesHonda DAXFranco CondeNo ratings yet