
Practical Approach To Common Electrolyte Emergencies
Practical Approach To Common Electrolyte Emergencies
You might also like
- Fertiglobal KatalogDocument65 pagesFertiglobal KatalogDavid Gluhić100% (1)
- Behavioral FinalsDocument28 pagesBehavioral FinalsKofiBNo ratings yet
- G24 Fragility FracturesDocument38 pagesG24 Fragility FracturesDeep Katyan DeepNo ratings yet
- Central Sensitisation Another Label or Useful DiagnosisDocument4 pagesCentral Sensitisation Another Label or Useful DiagnosisMohamed ElMeligieNo ratings yet
- HF Heart Failure: Kat BoardmanDocument8 pagesHF Heart Failure: Kat BoardmankkathrynannaNo ratings yet
- Extra Practice Predicting Products PDFDocument2 pagesExtra Practice Predicting Products PDFCollano M. Noel RogieNo ratings yet
- Localizing The LesionDocument30 pagesLocalizing The LesionTracy NwanneNo ratings yet
- Transfusion For ChildrenDocument5 pagesTransfusion For ChildrenKristine Mae AbrasaldoNo ratings yet
- Wilson S DiseaseDocument28 pagesWilson S DiseasemichaelcylNo ratings yet
- Sameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonDocument179 pagesSameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonNessreen JamalNo ratings yet
- DM CBLDocument18 pagesDM CBLbpt2No ratings yet
- Internal OSCE All Past Years QuestionsDocument17 pagesInternal OSCE All Past Years QuestionsOmar Nayef TaaniNo ratings yet
- Approach To Stroke PatientDocument16 pagesApproach To Stroke PatientNEuRoLoGisT CoFFeeCuP100% (2)
- Weakness B WDocument62 pagesWeakness B WKhan A RehNo ratings yet
- Endocarditis PediatricDocument56 pagesEndocarditis Pediatricfarzzana100% (1)
- Inflammatory Muscle Diseases NEJM 2015 Marinos DalakasDocument14 pagesInflammatory Muscle Diseases NEJM 2015 Marinos DalakasWalther Seven VGNo ratings yet
- Helping Baby To BreathDocument49 pagesHelping Baby To BreathmohdmaghyrehNo ratings yet
- Pathophysiology of Acute PainDocument12 pagesPathophysiology of Acute PainMuhammad Ghilman NurizzanNo ratings yet
- 1a-Introduction To MedicineDocument156 pages1a-Introduction To MedicineEshetu BizunehNo ratings yet
- Cranial Nerve ExaminationDocument45 pagesCranial Nerve ExaminationTanat AsavisanuNo ratings yet
- Bds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsDocument5 pagesBds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsJavariya AshrafNo ratings yet
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocument50 pagesSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanNo ratings yet
- Engine Assembly (3Zz Fe/4Zz Fe) : InspectionDocument4 pagesEngine Assembly (3Zz Fe/4Zz Fe) : Inspectionพลูโตเนียม สองสามเก้าNo ratings yet
- Transfusion RXNDocument17 pagesTransfusion RXNbeautifulbeastNo ratings yet
- TT PLANNING 4th Yr 29th Oct - BDS 4th Yr-1Document48 pagesTT PLANNING 4th Yr 29th Oct - BDS 4th Yr-1Andreea-Georgiana BălanNo ratings yet
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 pagesN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNo ratings yet
- A Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Document23 pagesA Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Lft Ediel PiñaNo ratings yet
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDocument49 pagesShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- Chronic Inflammatory Demyelinating PolyneuropathyDocument7 pagesChronic Inflammatory Demyelinating PolyneuropathyApriliaNo ratings yet
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocument80 pagesStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisNo ratings yet
- CBL 101Document446 pagesCBL 101YS NateNo ratings yet
- Learning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationDocument6 pagesLearning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationFrancisco Ahumada MéndezNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Acid - Base Balance & Abg AnalysisDocument71 pagesAcid - Base Balance & Abg AnalysisMohan KrishnaNo ratings yet
- PPTDocument61 pagesPPTRheal P EsmailNo ratings yet
- PruritusDocument10 pagesPruritusdikka ayuniNo ratings yet
- Osteoarthritis of The KneeDocument8 pagesOsteoarthritis of The Kneeas3syamut649250% (2)
- Anticoagulation in OrthopedicsDocument32 pagesAnticoagulation in Orthopedicsehabede6445No ratings yet
- Medical & Surgical Management in Cerebral PalsyDocument13 pagesMedical & Surgical Management in Cerebral PalsySahil SahniNo ratings yet
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentDocument47 pagesGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJamna MaharajNo ratings yet
- TB MeningeDocument75 pagesTB MeningeAyen FornollesNo ratings yet
- Hospital VS Form PDFDocument2 pagesHospital VS Form PDFsaguliteNo ratings yet
- Spinal Cord Deseases: Na ShaoDocument38 pagesSpinal Cord Deseases: Na ShaoArvindhanNo ratings yet
- LMNL Vs UmnlDocument49 pagesLMNL Vs UmnlLohshini ManickavasagamNo ratings yet
- Crisis Hipertensiva 2019 NEJMDocument10 pagesCrisis Hipertensiva 2019 NEJMRodolfo B. Lopez MiralrioNo ratings yet
- Myopathies: Presented By, Dr. Chandan N Intern, Department of Medicine, MIMS, MandyaDocument42 pagesMyopathies: Presented By, Dr. Chandan N Intern, Department of Medicine, MIMS, MandyaShafira WidiaNo ratings yet
- Where Is The LesionDocument12 pagesWhere Is The LesionHo Yong WaiNo ratings yet
- Fracture 01Document42 pagesFracture 01api-19916399No ratings yet
- 4.cardivascular System ExaminationDocument60 pages4.cardivascular System ExaminationElvisNo ratings yet
- Heart Failure Edit PutihDocument46 pagesHeart Failure Edit PutihJessica Christiana PutriNo ratings yet
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 pagesGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000No ratings yet
- Nerve Injury of Upper LimbDocument41 pagesNerve Injury of Upper LimbbashirjnmcNo ratings yet
- Palak Khanna Sadhana Shukla Madiha Rehamani Ishwin Tandon: By: (Group 2) (Group 2) (Group 2) (Group 1)Document43 pagesPalak Khanna Sadhana Shukla Madiha Rehamani Ishwin Tandon: By: (Group 2) (Group 2) (Group 2) (Group 1)pal0% (1)
- Fractures of The Upper LimbDocument20 pagesFractures of The Upper LimbWendy Francisca Borquez PerezNo ratings yet
- EndocrinologyDocument37 pagesEndocrinologyKochaMsangiNo ratings yet
- Peripheral Neuropathies FOR CLASSIFICATIONDocument9 pagesPeripheral Neuropathies FOR CLASSIFICATIONAnnie JoNo ratings yet
- Cardiomyopathy: M Taufik I, MDDocument28 pagesCardiomyopathy: M Taufik I, MDChi RahmawatiNo ratings yet
- Proposed Constituent Type of Evidence Dose IndicationDocument2 pagesProposed Constituent Type of Evidence Dose IndicationAdrian NasagerNo ratings yet
- USMLE Step 2 (3) - Thyroid DiseaseDocument4 pagesUSMLE Step 2 (3) - Thyroid DiseaseMavra zNo ratings yet
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- As 1038.14.2-2003 Coal and Coke - Analysis and Testing Higher Rank Coal Ash and Coke Ash - Major and Minor ElDocument7 pagesAs 1038.14.2-2003 Coal and Coke - Analysis and Testing Higher Rank Coal Ash and Coke Ash - Major and Minor ElSAI Global - APAC100% (1)
- Soil Kits: Pool and Spa Wastewater Drinking Water Process WaterDocument9 pagesSoil Kits: Pool and Spa Wastewater Drinking Water Process Watermeanangel4No ratings yet
- Apricot Health Benefits and Nutrition FactsDocument7 pagesApricot Health Benefits and Nutrition FactsVijay BhanNo ratings yet
- MineralsDocument87 pagesMineralsHaren Aizhel TenderoNo ratings yet
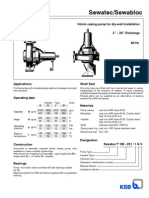
- TSB Sewatec and SewablocDocument28 pagesTSB Sewatec and SewablocZoro4zenaNo ratings yet
- Lecture 6Document38 pagesLecture 6Shaezarah MohamudallyNo ratings yet
- MKS Fluids Compilation: Compliments of Molecular Knowledge SystemsDocument2 pagesMKS Fluids Compilation: Compliments of Molecular Knowledge SystemsZaw Moe KhineNo ratings yet
- Preparation of SaltsDocument8 pagesPreparation of SaltsRose MusariraNo ratings yet
- Practical Organic Chemistry For Advanced StudentsDocument306 pagesPractical Organic Chemistry For Advanced StudentsSamuel DinizNo ratings yet
- Chemical Magic Ford PDFDocument73 pagesChemical Magic Ford PDFPablo HerediaNo ratings yet
- IGCSE Chemistry - Groups 1, 7 and 0Document11 pagesIGCSE Chemistry - Groups 1, 7 and 0ChemistryKlipz100% (4)
- Groundwater Quality and Geothermal Energy. The Case of Cerro PrietoDocument19 pagesGroundwater Quality and Geothermal Energy. The Case of Cerro PrietoLudwi GirabieNo ratings yet
- New Guidelines For Potassium ReplacementDocument33 pagesNew Guidelines For Potassium ReplacementAnggry MambaitNo ratings yet
- Flame Test LabDocument4 pagesFlame Test LabEamon BarkhordarianNo ratings yet
- Waterborn Silicate PaintsDocument98 pagesWaterborn Silicate PaintsJane Ashworth100% (1)
- 2012 Form 5 (Paper 3)Document6 pages2012 Form 5 (Paper 3)Nieda IbrahimNo ratings yet
- Hydrogen Peroxide: Concentration Determination 0.1-5%Document3 pagesHydrogen Peroxide: Concentration Determination 0.1-5%Muzaffar BhatNo ratings yet
- Anayytical Methods Section PDFDocument174 pagesAnayytical Methods Section PDFTatianaNo ratings yet
- Chemistry: Fitzroy's Storm GlassDocument29 pagesChemistry: Fitzroy's Storm GlassIon IonescuNo ratings yet
- Practical SyllabusDocument4 pagesPractical SyllabusOmSilence2651No ratings yet
- Methods of Fertilizer Application: AgriinfoDocument16 pagesMethods of Fertilizer Application: AgriinfojanineNo ratings yet
- Rpms ToolsDocument322 pagesRpms ToolsErnie Caracas LahaylahayNo ratings yet
- Caldo Asparagina PseudomonasDocument2 pagesCaldo Asparagina PseudomonasMSc Penélope MeloNo ratings yet
- Laboratory Chemical Inventory List (Example)Document9 pagesLaboratory Chemical Inventory List (Example)Aris RahmanNo ratings yet
- Explosives-Whistles - Pyrotechnica XIDocument6 pagesExplosives-Whistles - Pyrotechnica XIhwelch5792No ratings yet
- UP - Inorganic Pharmaceutical ChemistryDocument18 pagesUP - Inorganic Pharmaceutical ChemistryKate Evangelista100% (1)
- Pharm Inorg Medicinal Chemistry MidtermDocument247 pagesPharm Inorg Medicinal Chemistry MidtermRohaniah Lumna NoorNo ratings yet
- Chapter-1 Nitrogen Industries & Agro-Chemical IndustriesDocument45 pagesChapter-1 Nitrogen Industries & Agro-Chemical Industriesprashant_cool_4_uNo ratings yet























































































Download as ppt, pdf, or txt
You might also like
- Fertiglobal KatalogDocument65 pagesFertiglobal KatalogDavid Gluhić100% (1)
- Behavioral FinalsDocument28 pagesBehavioral FinalsKofiBNo ratings yet
- G24 Fragility FracturesDocument38 pagesG24 Fragility FracturesDeep Katyan DeepNo ratings yet
- Central Sensitisation Another Label or Useful DiagnosisDocument4 pagesCentral Sensitisation Another Label or Useful DiagnosisMohamed ElMeligieNo ratings yet
- HF Heart Failure: Kat BoardmanDocument8 pagesHF Heart Failure: Kat BoardmankkathrynannaNo ratings yet
- Extra Practice Predicting Products PDFDocument2 pagesExtra Practice Predicting Products PDFCollano M. Noel RogieNo ratings yet
- Localizing The LesionDocument30 pagesLocalizing The LesionTracy NwanneNo ratings yet
- Transfusion For ChildrenDocument5 pagesTransfusion For ChildrenKristine Mae AbrasaldoNo ratings yet
- Wilson S DiseaseDocument28 pagesWilson S DiseasemichaelcylNo ratings yet
- Sameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonDocument179 pagesSameer Smadi MD. Amman-Jordan: Consultant HBP and Liver Transplantation SurgeonNessreen JamalNo ratings yet
- DM CBLDocument18 pagesDM CBLbpt2No ratings yet
- Internal OSCE All Past Years QuestionsDocument17 pagesInternal OSCE All Past Years QuestionsOmar Nayef TaaniNo ratings yet
- Approach To Stroke PatientDocument16 pagesApproach To Stroke PatientNEuRoLoGisT CoFFeeCuP100% (2)
- Weakness B WDocument62 pagesWeakness B WKhan A RehNo ratings yet
- Endocarditis PediatricDocument56 pagesEndocarditis Pediatricfarzzana100% (1)
- Inflammatory Muscle Diseases NEJM 2015 Marinos DalakasDocument14 pagesInflammatory Muscle Diseases NEJM 2015 Marinos DalakasWalther Seven VGNo ratings yet
- Helping Baby To BreathDocument49 pagesHelping Baby To BreathmohdmaghyrehNo ratings yet
- Pathophysiology of Acute PainDocument12 pagesPathophysiology of Acute PainMuhammad Ghilman NurizzanNo ratings yet
- 1a-Introduction To MedicineDocument156 pages1a-Introduction To MedicineEshetu BizunehNo ratings yet
- Cranial Nerve ExaminationDocument45 pagesCranial Nerve ExaminationTanat AsavisanuNo ratings yet
- Bds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsDocument5 pagesBds Third Professional Examination 2007 General Medicine Table of Specifications Chapter Wise Distribution of Mcqs and SeqsJavariya AshrafNo ratings yet
- Seizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityDocument50 pagesSeizures and Epilepsy: Haining Li General Hospital of Ningxia Medical UniversityArvindhanNo ratings yet
- Engine Assembly (3Zz Fe/4Zz Fe) : InspectionDocument4 pagesEngine Assembly (3Zz Fe/4Zz Fe) : Inspectionพลูโตเนียม สองสามเก้าNo ratings yet
- Transfusion RXNDocument17 pagesTransfusion RXNbeautifulbeastNo ratings yet
- TT PLANNING 4th Yr 29th Oct - BDS 4th Yr-1Document48 pagesTT PLANNING 4th Yr 29th Oct - BDS 4th Yr-1Andreea-Georgiana BălanNo ratings yet
- N C C N D: Ursing ARE OF Lients With Eurologic IsordersDocument96 pagesN C C N D: Ursing ARE OF Lients With Eurologic IsordersMatt Lao DionelaNo ratings yet
- A Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Document23 pagesA Framework For Exercise Prescription: DOI: 10.1097/TGR.0000000000000011Lft Ediel PiñaNo ratings yet
- Shortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesDocument49 pagesShortness of Breath: UNC Emergency Medicine Medical Student Lecture SeriesGilbert Solomon Tantono100% (1)
- Chronic Inflammatory Demyelinating PolyneuropathyDocument7 pagesChronic Inflammatory Demyelinating PolyneuropathyApriliaNo ratings yet
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocument80 pagesStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisNo ratings yet
- CBL 101Document446 pagesCBL 101YS NateNo ratings yet
- Learning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationDocument6 pagesLearning and Cognitive Flexibility - Frontostriatal Function and Monoaminergic ModulationFrancisco Ahumada MéndezNo ratings yet
- Hyper para Thyroid Is MDocument27 pagesHyper para Thyroid Is MIbrahimWagesNo ratings yet
- Acid - Base Balance & Abg AnalysisDocument71 pagesAcid - Base Balance & Abg AnalysisMohan KrishnaNo ratings yet
- PPTDocument61 pagesPPTRheal P EsmailNo ratings yet
- PruritusDocument10 pagesPruritusdikka ayuniNo ratings yet
- Osteoarthritis of The KneeDocument8 pagesOsteoarthritis of The Kneeas3syamut649250% (2)
- Anticoagulation in OrthopedicsDocument32 pagesAnticoagulation in Orthopedicsehabede6445No ratings yet
- Medical & Surgical Management in Cerebral PalsyDocument13 pagesMedical & Surgical Management in Cerebral PalsySahil SahniNo ratings yet
- Growth and Development: Infancy Early Childhood Middle Childhood AdolescentDocument47 pagesGrowth and Development: Infancy Early Childhood Middle Childhood AdolescentJamna MaharajNo ratings yet
- TB MeningeDocument75 pagesTB MeningeAyen FornollesNo ratings yet
- Hospital VS Form PDFDocument2 pagesHospital VS Form PDFsaguliteNo ratings yet
- Spinal Cord Deseases: Na ShaoDocument38 pagesSpinal Cord Deseases: Na ShaoArvindhanNo ratings yet
- LMNL Vs UmnlDocument49 pagesLMNL Vs UmnlLohshini ManickavasagamNo ratings yet
- Crisis Hipertensiva 2019 NEJMDocument10 pagesCrisis Hipertensiva 2019 NEJMRodolfo B. Lopez MiralrioNo ratings yet
- Myopathies: Presented By, Dr. Chandan N Intern, Department of Medicine, MIMS, MandyaDocument42 pagesMyopathies: Presented By, Dr. Chandan N Intern, Department of Medicine, MIMS, MandyaShafira WidiaNo ratings yet
- Where Is The LesionDocument12 pagesWhere Is The LesionHo Yong WaiNo ratings yet
- Fracture 01Document42 pagesFracture 01api-19916399No ratings yet
- 4.cardivascular System ExaminationDocument60 pages4.cardivascular System ExaminationElvisNo ratings yet
- Heart Failure Edit PutihDocument46 pagesHeart Failure Edit PutihJessica Christiana PutriNo ratings yet
- Glycogen Storage Disease, Type II (Pompe Disease) : BackgroundDocument7 pagesGlycogen Storage Disease, Type II (Pompe Disease) : Background201111000No ratings yet
- Nerve Injury of Upper LimbDocument41 pagesNerve Injury of Upper LimbbashirjnmcNo ratings yet
- Palak Khanna Sadhana Shukla Madiha Rehamani Ishwin Tandon: By: (Group 2) (Group 2) (Group 2) (Group 1)Document43 pagesPalak Khanna Sadhana Shukla Madiha Rehamani Ishwin Tandon: By: (Group 2) (Group 2) (Group 2) (Group 1)pal0% (1)
- Fractures of The Upper LimbDocument20 pagesFractures of The Upper LimbWendy Francisca Borquez PerezNo ratings yet
- EndocrinologyDocument37 pagesEndocrinologyKochaMsangiNo ratings yet
- Peripheral Neuropathies FOR CLASSIFICATIONDocument9 pagesPeripheral Neuropathies FOR CLASSIFICATIONAnnie JoNo ratings yet
- Cardiomyopathy: M Taufik I, MDDocument28 pagesCardiomyopathy: M Taufik I, MDChi RahmawatiNo ratings yet
- Proposed Constituent Type of Evidence Dose IndicationDocument2 pagesProposed Constituent Type of Evidence Dose IndicationAdrian NasagerNo ratings yet
- USMLE Step 2 (3) - Thyroid DiseaseDocument4 pagesUSMLE Step 2 (3) - Thyroid DiseaseMavra zNo ratings yet
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- As 1038.14.2-2003 Coal and Coke - Analysis and Testing Higher Rank Coal Ash and Coke Ash - Major and Minor ElDocument7 pagesAs 1038.14.2-2003 Coal and Coke - Analysis and Testing Higher Rank Coal Ash and Coke Ash - Major and Minor ElSAI Global - APAC100% (1)
- Soil Kits: Pool and Spa Wastewater Drinking Water Process WaterDocument9 pagesSoil Kits: Pool and Spa Wastewater Drinking Water Process Watermeanangel4No ratings yet
- Apricot Health Benefits and Nutrition FactsDocument7 pagesApricot Health Benefits and Nutrition FactsVijay BhanNo ratings yet
- MineralsDocument87 pagesMineralsHaren Aizhel TenderoNo ratings yet
- TSB Sewatec and SewablocDocument28 pagesTSB Sewatec and SewablocZoro4zenaNo ratings yet
- Lecture 6Document38 pagesLecture 6Shaezarah MohamudallyNo ratings yet
- MKS Fluids Compilation: Compliments of Molecular Knowledge SystemsDocument2 pagesMKS Fluids Compilation: Compliments of Molecular Knowledge SystemsZaw Moe KhineNo ratings yet
- Preparation of SaltsDocument8 pagesPreparation of SaltsRose MusariraNo ratings yet
- Practical Organic Chemistry For Advanced StudentsDocument306 pagesPractical Organic Chemistry For Advanced StudentsSamuel DinizNo ratings yet
- Chemical Magic Ford PDFDocument73 pagesChemical Magic Ford PDFPablo HerediaNo ratings yet
- IGCSE Chemistry - Groups 1, 7 and 0Document11 pagesIGCSE Chemistry - Groups 1, 7 and 0ChemistryKlipz100% (4)
- Groundwater Quality and Geothermal Energy. The Case of Cerro PrietoDocument19 pagesGroundwater Quality and Geothermal Energy. The Case of Cerro PrietoLudwi GirabieNo ratings yet
- New Guidelines For Potassium ReplacementDocument33 pagesNew Guidelines For Potassium ReplacementAnggry MambaitNo ratings yet
- Flame Test LabDocument4 pagesFlame Test LabEamon BarkhordarianNo ratings yet
- Waterborn Silicate PaintsDocument98 pagesWaterborn Silicate PaintsJane Ashworth100% (1)
- 2012 Form 5 (Paper 3)Document6 pages2012 Form 5 (Paper 3)Nieda IbrahimNo ratings yet
- Hydrogen Peroxide: Concentration Determination 0.1-5%Document3 pagesHydrogen Peroxide: Concentration Determination 0.1-5%Muzaffar BhatNo ratings yet
- Anayytical Methods Section PDFDocument174 pagesAnayytical Methods Section PDFTatianaNo ratings yet
- Chemistry: Fitzroy's Storm GlassDocument29 pagesChemistry: Fitzroy's Storm GlassIon IonescuNo ratings yet
- Practical SyllabusDocument4 pagesPractical SyllabusOmSilence2651No ratings yet
- Methods of Fertilizer Application: AgriinfoDocument16 pagesMethods of Fertilizer Application: AgriinfojanineNo ratings yet
- Rpms ToolsDocument322 pagesRpms ToolsErnie Caracas LahaylahayNo ratings yet
- Caldo Asparagina PseudomonasDocument2 pagesCaldo Asparagina PseudomonasMSc Penélope MeloNo ratings yet
- Laboratory Chemical Inventory List (Example)Document9 pagesLaboratory Chemical Inventory List (Example)Aris RahmanNo ratings yet
- Explosives-Whistles - Pyrotechnica XIDocument6 pagesExplosives-Whistles - Pyrotechnica XIhwelch5792No ratings yet
- UP - Inorganic Pharmaceutical ChemistryDocument18 pagesUP - Inorganic Pharmaceutical ChemistryKate Evangelista100% (1)
- Pharm Inorg Medicinal Chemistry MidtermDocument247 pagesPharm Inorg Medicinal Chemistry MidtermRohaniah Lumna NoorNo ratings yet
- Chapter-1 Nitrogen Industries & Agro-Chemical IndustriesDocument45 pagesChapter-1 Nitrogen Industries & Agro-Chemical Industriesprashant_cool_4_uNo ratings yet