Download as ppt, pdf, or txt
You might also like
- Inborn Metabolic Disease - Saudubray PDFDocument655 pagesInborn Metabolic Disease - Saudubray PDFCarlos Mendoza100% (5)
- BiochemistryDocument113 pagesBiochemistryMohammed Faizuddin siddiqui100% (1)
- Introduction To Endocrinology & Endocrine Function Tests.Document14 pagesIntroduction To Endocrinology & Endocrine Function Tests.Junayed Safar MahmudNo ratings yet
- Mathews - Biochemistry (Mathews 3rd Ed) PDFDocument2,464 pagesMathews - Biochemistry (Mathews 3rd Ed) PDFMiguel González96% (24)
- Metabolic OR Endocrine Disorders: Amanda Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistDocument124 pagesMetabolic OR Endocrine Disorders: Amanda Du, MD, DPPS, DPSNBM Pediatrician-NeonatologistLyn LynNo ratings yet
- Inborn Errors of Metabolism IEM 1Document36 pagesInborn Errors of Metabolism IEM 1bhaskar chinnanandhi100% (1)
- Genetics of Metabolic Disorders IDocument17 pagesGenetics of Metabolic Disorders IGagan DhaliwalNo ratings yet
- Inborn Errors or MetabolismDocument25 pagesInborn Errors or MetabolismAnonymous 7dsX2F8nNo ratings yet
- Inborn Errors or MetabolismDocument21 pagesInborn Errors or Metabolismsaleema11No ratings yet
- Inborn Error of MetabolismDocument16 pagesInborn Error of MetabolismIvy NNo ratings yet
- Inborn Errors of MetabolismDocument27 pagesInborn Errors of MetabolismShelyAzradNo ratings yet
- Amino Acid: Prepared By: Anthonette Ann Alemania-STEM 12Document28 pagesAmino Acid: Prepared By: Anthonette Ann Alemania-STEM 12Anthonette Alemania100% (1)
- Urine Screening For Metabolic Disorders: Learning ObjectivesDocument12 pagesUrine Screening For Metabolic Disorders: Learning ObjectivesJonalyn LumantasNo ratings yet
- G6PD, GalactosemiaDocument32 pagesG6PD, GalactosemiaEricka B. BanaszczukNo ratings yet
- Inborn Errors of MetabolismDocument4 pagesInborn Errors of Metabolismcurly perkyNo ratings yet
- Inborn Errors of MetabolismDocument60 pagesInborn Errors of MetabolismPyneandy KimberlyNo ratings yet
- ProteinDocument13 pagesProteinapi-272775120No ratings yet
- Ni Nyoman Ayu Dewi Dept. of Biochemistry, Faculty of Medicine Udayana University Ayu - Dewi@unud - Ac.idDocument37 pagesNi Nyoman Ayu Dewi Dept. of Biochemistry, Faculty of Medicine Udayana University Ayu - Dewi@unud - Ac.idWida Utami100% (1)
- Gastrointestinal Infections Shigellosis InfectionsDocument6 pagesGastrointestinal Infections Shigellosis InfectionsNishita ChandNo ratings yet
- Recombinant Protein Production in E.coliDocument23 pagesRecombinant Protein Production in E.coliSanjay KumarNo ratings yet
- Vitamins ReviewDocument105 pagesVitamins Reviewjltrek123No ratings yet
- Endocrinology NotesDocument12 pagesEndocrinology Notesrandiey john abelleraNo ratings yet
- Protein QuantificationDocument60 pagesProtein Quantificationkiedd_0491% (11)
- Genetics of Cystic FibrosisDocument3 pagesGenetics of Cystic Fibrosislutfiah_liaNo ratings yet
- Hemoglobin MetabolismDocument80 pagesHemoglobin MetabolismSurya BudikusumaNo ratings yet
- 6 - Clinical Biochemistry - 1001411Document14 pages6 - Clinical Biochemistry - 1001411bsmallahNo ratings yet
- Name Pi R Group: Characteristic Three LetterDocument1 pageName Pi R Group: Characteristic Three LetterAloysius QuitaligNo ratings yet
- Inborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Document4 pagesInborn Errors of Metabolism - Basics For Students (Iver Andreas Norbergs Kopi Som Er I Konflikt 2016-01-24)Wen Jie LauNo ratings yet
- Plasma EnzymesDocument4 pagesPlasma EnzymesIbrahim ZorobNo ratings yet
- Clinical Biochemistry Practical IDocument73 pagesClinical Biochemistry Practical Isama_omery100% (1)
- Diagnositc Testing: By: Jervy P. Beranrdino, RN, MSNDocument34 pagesDiagnositc Testing: By: Jervy P. Beranrdino, RN, MSNadni_wgNo ratings yet
- Chromosomal Abnormalities in Humans and AnimalsDocument15 pagesChromosomal Abnormalities in Humans and AnimalsGautam ChandwaniNo ratings yet
- Apoptosis Tutorial NotesDocument8 pagesApoptosis Tutorial NotesismealNo ratings yet
- Cell Biology LabManual Version 8.0 May 2012 1 TRUNCATEDDocument57 pagesCell Biology LabManual Version 8.0 May 2012 1 TRUNCATEDதுர்காஸ்ரீ கங்கா ராதிகாNo ratings yet
- Glycogen Storage DeseasesDocument26 pagesGlycogen Storage DeseasesirsaNo ratings yet
- Some Biochem MnemonicsDocument8 pagesSome Biochem MnemonicsMikey PalominoNo ratings yet
- Overview of Cystic Fibrosis & Its ManagementDocument54 pagesOverview of Cystic Fibrosis & Its Managementvani reddyNo ratings yet
- Carbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistryDocument93 pagesCarbohydrate Metabolism: By:-Dr - Priyanka Sharma 1 Year MDS Dept. of Public Health DentistrySimham Venu0% (1)
- Biochemistry of Digestive SystemDocument55 pagesBiochemistry of Digestive SystemSyam UnhasNo ratings yet
- Hormon GDSDocument23 pagesHormon GDSBRI KUNo ratings yet
- 2 - Lipid Metabolism Lecture For StudentsDocument68 pages2 - Lipid Metabolism Lecture For StudentshwhsgxNo ratings yet
- Shelly HyperlipidemiaDocument22 pagesShelly Hyperlipidemiaale marilNo ratings yet
- CoenzymesDocument60 pagesCoenzymesraddagNo ratings yet
- Mineral MetabolismDocument49 pagesMineral MetabolismArvind MishraNo ratings yet
- Multiple Choice Questions-Cancers: AdvertisementDocument5 pagesMultiple Choice Questions-Cancers: AdvertisementSp PpvNo ratings yet
- Reducing and Non-Reducing SugarDocument4 pagesReducing and Non-Reducing SugarAyunee ZulhasNo ratings yet
- What Are CarbohydratesDocument36 pagesWhat Are CarbohydratesPINNACLE CAFENo ratings yet
- Gluconeogenesis, Glycogen MetabolismDocument35 pagesGluconeogenesis, Glycogen MetabolismdanielachynaNo ratings yet
- Classification of Anemia OkDocument60 pagesClassification of Anemia OkAnonymous 7CnBF0cjNo ratings yet
- Enzyme Catalysis-Chapter 7 (Part 1)Document22 pagesEnzyme Catalysis-Chapter 7 (Part 1)OmSilence2651No ratings yet
- Modulator: Dr. P.B.Desai HOD, Dept of Biochemistry. Presenter: DR Vijayetha S. KagwadDocument68 pagesModulator: Dr. P.B.Desai HOD, Dept of Biochemistry. Presenter: DR Vijayetha S. KagwadvijayethaNo ratings yet
- Electron Transport ChainDocument9 pagesElectron Transport Chainalokesh1982100% (1)
- Biochemistry VivaDocument8 pagesBiochemistry VivaNazia WasimNo ratings yet
- Fatty Acid MetabolismDocument40 pagesFatty Acid MetabolismMichelle Arredondo100% (1)
- S13.CHO .MetabolismDocument18 pagesS13.CHO .MetabolismGhea Jovita SinagaNo ratings yet
- Inborn Error of MetabolismDocument33 pagesInborn Error of MetabolismAlmiraNo ratings yet
- Precision Medicine NOTESDocument50 pagesPrecision Medicine NOTESNishtha KhannaNo ratings yet
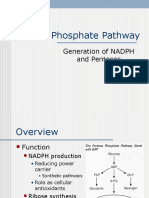
- Pentose Phosphate Pathway: Generation of NADPH and PentosesDocument23 pagesPentose Phosphate Pathway: Generation of NADPH and PentosesV sNo ratings yet
- Glucose, Part1Document33 pagesGlucose, Part1SarahNo ratings yet
- Nucleic Acid DisordersDocument29 pagesNucleic Acid Disorderskritimahajan1989No ratings yet
- Lesson 7.1 Inborn Errors of MetabolismDocument119 pagesLesson 7.1 Inborn Errors of Metabolismmisaki06100% (2)
- Nucleotide Metabolism: Introduction and de Novo Purine MetabolismDocument4 pagesNucleotide Metabolism: Introduction and de Novo Purine Metabolismkang seulgi can set me on fire with her gaze aloneNo ratings yet
- 41 & 42 - Nucleic Acid MetabolismDocument56 pages41 & 42 - Nucleic Acid MetabolismMădă Claws100% (1)
- Uworld JournalDocument3 pagesUworld JournalJayNo ratings yet
- Nucleotide Metabolism PPDocument65 pagesNucleotide Metabolism PPCLEMENTNo ratings yet
- Nucleotides McqsDocument8 pagesNucleotides McqsSp Ppv0% (1)
- Purine Metabolism de Novo Synthesis and Salvage Pathway, 2015Document28 pagesPurine Metabolism de Novo Synthesis and Salvage Pathway, 2015Tehreem NadeemNo ratings yet