Download as pptx, pdf, or txt
You might also like
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Pin Retained RestorationDocument31 pagesPin Retained RestorationVinisha Vipin SharmaNo ratings yet
- Preliminary ConsiderationsDocument22 pagesPreliminary ConsiderationsDayen LimNo ratings yet
- Rotary EndodonticsDocument61 pagesRotary EndodonticsVijayendra kamathNo ratings yet
- Single Visit Endodontic TherapyDocument95 pagesSingle Visit Endodontic TherapyAshish Bhadane100% (2)
- Composites in Pediatric Dentistry: ROLL NO. - 21277010001 Dr. Lopamoodra Das Batch-2018-2021Document20 pagesComposites in Pediatric Dentistry: ROLL NO. - 21277010001 Dr. Lopamoodra Das Batch-2018-2021Khushboorana A Scientist100% (1)
- Cervical AbrasionDocument14 pagesCervical AbrasionAdjei Joshua100% (1)
- Dental CariesDocument74 pagesDental CariesParidhi Garg67% (3)
- Psychological Considerations For Complete Denture Patients.Document7 pagesPsychological Considerations For Complete Denture Patients.Prateek MishraNo ratings yet
- Textbook of Pediatric Dentistry-3rd EditionDocument18 pagesTextbook of Pediatric Dentistry-3rd EditionAnna NgNo ratings yet
- Intra-Oral Radio Graphs For The Pediatric Dental Patient PedoDocument44 pagesIntra-Oral Radio Graphs For The Pediatric Dental Patient PedoFourthMolar.comNo ratings yet
- Lecture 4 Diagnosis of Dental CariesDocument12 pagesLecture 4 Diagnosis of Dental CariesDt omarNo ratings yet
- Geriatric EndodonticsDocument88 pagesGeriatric EndodonticsNajla MohammedNo ratings yet
- Adhesion Steps Total Etch Emax EmpressDocument1 pageAdhesion Steps Total Etch Emax EmpressErick Lachner100% (1)
- 4-Fluid Control &tissue DilationDocument57 pages4-Fluid Control &tissue Dilationyahia salahNo ratings yet
- Australian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryDocument7 pagesAustralian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryVishakha SabooNo ratings yet
- Soffit and PCD PDFDocument4 pagesSoffit and PCD PDFKalpanaNo ratings yet
- Clinical ConsiderationsDocument108 pagesClinical ConsiderationsPankaj JainNo ratings yet
- Odontogenic Cysts and TumorsDocument273 pagesOdontogenic Cysts and TumorsAliImadAlKhasaki82% (11)
- Management of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearDocument44 pagesManagement of Discoloured Teeth: Presented By: Amisha Jain M.D.S II YearANUBHANo ratings yet
- Use of Polyethylene Ribbon To Create A Provisional Fixed Partial DentureDocument4 pagesUse of Polyethylene Ribbon To Create A Provisional Fixed Partial DentureAhmed AbdulazeezNo ratings yet
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Document27 pagesPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. ZoghborNo ratings yet
- Decision Trees For Management of An Avulsed Permanent ToothDocument2 pagesDecision Trees For Management of An Avulsed Permanent ToothAbhi ThakkarNo ratings yet
- Rationale of Endodontic TreatmentDocument45 pagesRationale of Endodontic TreatmentAmy Rita0% (1)
- Surgical Extrusion: A Dental TechniqueDocument6 pagesSurgical Extrusion: A Dental TechniqueDragos CiongaruNo ratings yet
- Complex RestorationDocument59 pagesComplex Restorationsamar yousif mohamed100% (1)
- Devices and Methods For Preheating Prewarming Dental Resin CompositesDocument4 pagesDevices and Methods For Preheating Prewarming Dental Resin CompositesMADA100% (1)
- Classification of Endodontic FlapsDocument23 pagesClassification of Endodontic FlapsDilu DavisNo ratings yet
- Mechanism of Action of Fluoride in Dental Caries PedoDocument21 pagesMechanism of Action of Fluoride in Dental Caries PedoFourthMolar.com100% (1)
- Basic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014Document54 pagesBasic TxPlanning-Prognosis and Treatment Planning-Revised 9 September 2014DraspiNo ratings yet
- Estrogenicity of CompositesDocument8 pagesEstrogenicity of CompositesSubhashini RajshekarNo ratings yet
- Periodontic - EndodonticDocument86 pagesPeriodontic - EndodonticPiyusha SharmaNo ratings yet
- Single Visit Vs Multiple Visit EndodonticsDocument47 pagesSingle Visit Vs Multiple Visit Endodonticspiece_of_mindzz1969No ratings yet
- Gypsum Products Gypsum Products Gypsum Products Gypsum Products Gypsum ProductsDocument16 pagesGypsum Products Gypsum Products Gypsum Products Gypsum Products Gypsum ProductsZHAREIGHNEILE C. MAMOLO100% (1)
- Endodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarDocument6 pagesEndodontic Failures-A Review: Dr. Sadashiv Daokar, DR - Anita.KalekarGunjan GargNo ratings yet
- Endodontic MicrobiologyDocument219 pagesEndodontic Microbiologyrasagna reddy100% (1)
- Lec7-Selection of Artificial TeethDocument12 pagesLec7-Selection of Artificial TeethHassan BotaniNo ratings yet
- Aiims MDS Entrance Exam Past Questions Nov 2001Document190 pagesAiims MDS Entrance Exam Past Questions Nov 2001Raman Dhungel100% (2)
- Fibro OsseousDocument25 pagesFibro OsseoussadiaNo ratings yet
- Dentinal Hypersensitivity: Dr. Nitin MaitinDocument133 pagesDentinal Hypersensitivity: Dr. Nitin MaitinShipra MaitinNo ratings yet
- DIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsDocument51 pagesDIAGNOSTIC METHODS (Emphasis On Recent Advances) IN EndodonticsKalpesh DeyNo ratings yet
- Complex Amalgam Restoration (Final)Document26 pagesComplex Amalgam Restoration (Final)Neil HerreraNo ratings yet
- Cleaning & ShapingDocument47 pagesCleaning & ShapingdrmahmoudbadrNo ratings yet
- Aberrant Frenum and Its TreatmentDocument90 pagesAberrant Frenum and Its TreatmentheycoolalexNo ratings yet
- 12 Pin Retained RestorationDocument59 pages12 Pin Retained RestorationMohsin HabibNo ratings yet
- Case HistoryDocument135 pagesCase HistoryDr. Victor Samuel100% (6)
- Tanvi Shah - Maaz ShaikhDocument29 pagesTanvi Shah - Maaz ShaikhTanvi ShahNo ratings yet
- Diagnosis and Diagnostic Adis in Endodontics - Copy (100668749)Document39 pagesDiagnosis and Diagnostic Adis in Endodontics - Copy (100668749)kapilphysio100% (1)
- 1-2-3 Steps in Endodontic Irrigation PDFDocument4 pages1-2-3 Steps in Endodontic Irrigation PDFAnn M.No ratings yet
- Cervical Margin Relocation and Indirect Restorations: Case Report and Literature ReviewDocument5 pagesCervical Margin Relocation and Indirect Restorations: Case Report and Literature ReviewDevin KwanNo ratings yet
- Removable Partial DentureDocument72 pagesRemovable Partial DentureAyodele Oludare AyodejiNo ratings yet
- ErythroplakiaDocument20 pagesErythroplakiaEshan VermaNo ratings yet
- Lecture 6 - Reconstructive Periodontal Surgery Part I PPT EsamDocument24 pagesLecture 6 - Reconstructive Periodontal Surgery Part I PPT EsamHaneen Al-HajjNo ratings yet
- Recent Advances in Pulp Vitality TestingDocument6 pagesRecent Advances in Pulp Vitality Testingatul_singh2001No ratings yet
- Complex Amalgam Restoration LectureDocument30 pagesComplex Amalgam Restoration LectureaakritiNo ratings yet
- Oral Manifestations of Denture AbuseDocument53 pagesOral Manifestations of Denture AbuseBharanija100% (2)
- Basic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionFrom EverandBasic Level of Dental Resins - Material Science & Technology: 4th Edition, 2nd VersionNo ratings yet
- DENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideFrom EverandDENTAL AUXILIARY EDUCATION EXAMINATION IN DENTAL MATERIALS: Passbooks Study GuideNo ratings yet
- Diff Betwn Inlay and Amalgam CavityDocument7 pagesDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDocument6 pagesNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaNo ratings yet
- Acupuncture in Dentistry PDFDocument73 pagesAcupuncture in Dentistry PDFVinisha Vipin SharmaNo ratings yet
- Content ServerDocument5 pagesContent ServerVinisha Vipin SharmaNo ratings yet
- Mechanical Preparation Updated May2017 Prof Marco VersianiDocument159 pagesMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaNo ratings yet
- Challenges in Working Length DeterminationDocument101 pagesChallenges in Working Length DeterminationVinisha Vipin SharmaNo ratings yet
- Criteria of SelectionDocument12 pagesCriteria of SelectionVinisha Vipin SharmaNo ratings yet
- Glide Path PreparationDocument5 pagesGlide Path PreparationVinisha Vipin SharmaNo ratings yet
- Some Basics of LasersDocument102 pagesSome Basics of LasersVinisha Vipin SharmaNo ratings yet
- Laser in Conservative Dentistry & EndodonticsDocument75 pagesLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaNo ratings yet
- Show TextDocument1 pageShow TextVinisha Vipin SharmaNo ratings yet
- Eaat 14 I 1 P 217Document6 pagesEaat 14 I 1 P 217Vinisha Vipin SharmaNo ratings yet
- EchsDocument20 pagesEchsVinisha Vipin SharmaNo ratings yet
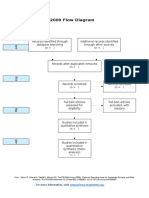
- PRISMA 2009 Flow Diagram: For More Information, VisitDocument1 pagePRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaNo ratings yet
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDocument5 pagesCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaNo ratings yet
- Content ServerDocument6 pagesContent ServerVinisha Vipin SharmaNo ratings yet
- Dentin HypersensitivityDocument62 pagesDentin HypersensitivityVinisha Vipin Sharma100% (1)
- Nanodentistry: New Buzz in Dentistry: Review ArticleDocument5 pagesNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaNo ratings yet
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDocument5 pagesPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaNo ratings yet
- PRISMA-P Statement - Moher Sys Rev Jan 2015Document9 pagesPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaNo ratings yet
- Clarks Cavity PreparationDocument10 pagesClarks Cavity PreparationVinisha Vipin SharmaNo ratings yet
- Esthetic Alternatives To AmalgamDocument15 pagesEsthetic Alternatives To AmalgamVinisha Vipin SharmaNo ratings yet
- Introduction To PharmacologyDocument50 pagesIntroduction To PharmacologyAbdishakour Hassa.100% (1)
- A Thesis On Homoeopathic Management of GoutDocument3 pagesA Thesis On Homoeopathic Management of GouthirenNo ratings yet
- ChemotherapyDocument102 pagesChemotherapyJoseph John K Pothanikat100% (1)
- Nevada Dentist Adam Lousig-Nont Had Complaints From 5 PatientsDocument38 pagesNevada Dentist Adam Lousig-Nont Had Complaints From 5 PatientsLas Vegas Review-JournalNo ratings yet
- Lyme Disease and The GutDocument14 pagesLyme Disease and The GutClaudeVanDammNo ratings yet
- Hypnosis or HypnotherapyDocument5 pagesHypnosis or HypnotherapyNadeem IqbalNo ratings yet
- NarcolepsyDocument25 pagesNarcolepsysnackwellsNo ratings yet
- Chemotherapy RadiationDocument2 pagesChemotherapy RadiationPeter Lucky TurianoNo ratings yet
- The Test Urine CultureDocument13 pagesThe Test Urine CultureAnonymous 5aoV2RWWAwNo ratings yet
- Long-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyDocument5 pagesLong-Term Efficacy of Percutaneous Steroid Injection For Treating Benign Vocal Fold Lesions: A Prospective StudyWahyu JuliandaNo ratings yet
- Pokhrel PresentationDocument13 pagesPokhrel Presentationapi-374957857No ratings yet
- Parental Routes of AdministrationDocument2 pagesParental Routes of AdministrationdrugdrugNo ratings yet
- Antibiotic Therapy: The Pneumonia PanaceaDocument3 pagesAntibiotic Therapy: The Pneumonia PanaceabobbyramakantNo ratings yet
- Full Crown ModuleDocument16 pagesFull Crown ModuleDragos 1No ratings yet
- Clinical Research DocumentationDocument2 pagesClinical Research Documentationamey_dpdNo ratings yet
- Methadone Hydro ChlorideDocument4 pagesMethadone Hydro Chlorideapi-3797941100% (1)
- Resume 101: Write A Resume That Gets You NoticedDocument16 pagesResume 101: Write A Resume That Gets You Noticedgqu3No ratings yet
- RAdiology Related Infratemporal Fossa, Pterygo Palatine Fossa, Parapharyngeal SpaceDocument11 pagesRAdiology Related Infratemporal Fossa, Pterygo Palatine Fossa, Parapharyngeal SpacehaneefmdfNo ratings yet
- Pityrosporum FolliculitisDocument3 pagesPityrosporum Folliculitisshivam18No ratings yet
- 7 Consent Form 09Document1 page7 Consent Form 09DentalBoardNo ratings yet
- 1.2 An-Introduction-to-Quality-Improvement-Society-of-Hospital-Medicine-revROBDocument67 pages1.2 An-Introduction-to-Quality-Improvement-Society-of-Hospital-Medicine-revROBMICHAEL DOGBENo ratings yet
- 2017 SF Surrogacy Conference, Jan 14-15Document28 pages2017 SF Surrogacy Conference, Jan 14-15Men Having Babies, Inc.No ratings yet
- Otitis Media: Joseph E. Kerschner and Diego PreciadoDocument16 pagesOtitis Media: Joseph E. Kerschner and Diego PreciadoTridiaPutraGunantaNo ratings yet
- Fistula ManagementDocument34 pagesFistula ManagementNoer AfhizanNo ratings yet
- Non-Pharmacologic Pain Management in OrthodonticsDocument21 pagesNon-Pharmacologic Pain Management in OrthodonticsDr. Kanak100% (1)
- Review Article in ProsthodonticsDocument8 pagesReview Article in ProsthodonticsChandrika VeerareddyNo ratings yet
- Referral System in IndiaDocument25 pagesReferral System in IndiaKailash NagarNo ratings yet
- BLS Book (New)Document7 pagesBLS Book (New)Saman FirdousNo ratings yet
- Thyroid Disorder Research PaperDocument5 pagesThyroid Disorder Research Paperapi-254922343No ratings yet