
Pediatric Sports Injuries
Pediatric Sports Injuries
You might also like
- Sex God SecretsDocument123 pagesSex God SecretsKhamiss Khouya55% (20)
- 2004 RX8 Parts ManualDocument15 pages2004 RX8 Parts Manualgo0n80% (10)
- Planning and Scheduling of SubstructureDocument81 pagesPlanning and Scheduling of SubstructureHnin Wai Mar Aung100% (3)
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- When To Operate On Spinal Cysts - Dr. WelchDocument57 pagesWhen To Operate On Spinal Cysts - Dr. WelchSaro HerreraNo ratings yet
- Diving Injuries Research Findings and Recommendations For Reducing Catastrophic Injuries PDFDocument273 pagesDiving Injuries Research Findings and Recommendations For Reducing Catastrophic Injuries PDFcarlosNo ratings yet
- Steven Schick Learning Brian Ferneyhough's Bone Alphabet PDFDocument23 pagesSteven Schick Learning Brian Ferneyhough's Bone Alphabet PDFRokitMan_No ratings yet
- Forearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandForearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diabetic FootDocument4 pagesDiabetic FoothegazyscribdNo ratings yet
- DR G Avinash Rao Fellow in Hand and Microsurgery: ArthrogryposisDocument74 pagesDR G Avinash Rao Fellow in Hand and Microsurgery: Arthrogryposisavinashrao39100% (1)
- Lower Extremity DisordersDocument25 pagesLower Extremity DisordersJameson87No ratings yet
- Biomechanics of Volleyball SpikesDocument20 pagesBiomechanics of Volleyball SpikesMujid Benazer100% (2)
- Sports Therapy Dissertation IdeasDocument6 pagesSports Therapy Dissertation IdeasCustomizedPaperSingapore100% (1)
- ACL Injuries in Female Athletes PowerpointDocument8 pagesACL Injuries in Female Athletes Powerpointrupinder24No ratings yet
- MF2 - Spinal Cord InjuryDocument43 pagesMF2 - Spinal Cord InjuryAnnbe BarteNo ratings yet
- Orthopaedic EmergenciesDocument12 pagesOrthopaedic EmergenciesUhuebor DavidNo ratings yet
- Musculoskeletal Disease Associated With Diabetes MellitusDocument290 pagesMusculoskeletal Disease Associated With Diabetes Mellituscharanmann9165No ratings yet
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 pagesPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- Managing Psychiatric Patients in The EDDocument28 pagesManaging Psychiatric Patients in The EDfadiNo ratings yet
- Congenital Dysplasia & DislocatiDocument558 pagesCongenital Dysplasia & DislocatiWilson A. QuinteroNo ratings yet
- Injuries, Risk Factors and Prevention Initiatives in Youth SportDocument27 pagesInjuries, Risk Factors and Prevention Initiatives in Youth SportDonny KurniawanNo ratings yet
- Posterior Tibialis Tendon Dysfunction (PTTD)Document11 pagesPosterior Tibialis Tendon Dysfunction (PTTD)bigpawn13No ratings yet
- AclDocument20 pagesAclDanny OtNo ratings yet
- Chapter 55 - Pelvic Trauma Episode OverviewDocument8 pagesChapter 55 - Pelvic Trauma Episode OverviewKadek Adi WigunaNo ratings yet
- Crush InjuryDocument4 pagesCrush InjuryMuhammad Nur ArifinNo ratings yet
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Document59 pagesTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNo ratings yet
- Peripheral Nerve Injury: J. Navin KumarDocument100 pagesPeripheral Nerve Injury: J. Navin Kumarpuravi91No ratings yet
- Limping Child: Department of Orthopaedics Afmc, PuneDocument101 pagesLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNo ratings yet
- Open Fracture: A Presentation byDocument44 pagesOpen Fracture: A Presentation byNur Liyana Ahmad ZakiNo ratings yet
- Dance Injuries-Foot and AnkleDocument7 pagesDance Injuries-Foot and Ankleapi-198787605100% (1)
- DDH 2Document3 pagesDDH 2monique_munoz_2No ratings yet
- Rehabilitation Management For Rheumatoid Arthritis Patients 2Document19 pagesRehabilitation Management For Rheumatoid Arthritis Patients 2Jothiprasanna KNo ratings yet
- Muscular Dystrophy Fact SheetDocument2 pagesMuscular Dystrophy Fact Sheetmdhaddock87100% (1)
- MPT SyllabusDocument8 pagesMPT Syllabusbluesky_jawedNo ratings yet
- Perthes Disease: Mohamed Hamood MohamedDocument4 pagesPerthes Disease: Mohamed Hamood MohamedMohamed HamoodNo ratings yet
- Fractures in ChildrenDocument5 pagesFractures in ChildrenAbigaille ChuaNo ratings yet
- Congenital Hand AnomaliesDocument59 pagesCongenital Hand AnomaliesnessyuarniNo ratings yet
- 2-Physiotherapy For FracturesDocument17 pages2-Physiotherapy For FracturesJuanitoCabatañaLimIIINo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- What Is Spinal StenosisDocument10 pagesWhat Is Spinal Stenosismariamel31No ratings yet
- Foot Ankle InjuriesDocument55 pagesFoot Ankle InjuriesMark Jan HorstNo ratings yet
- What Is Sport InjuryDocument6 pagesWhat Is Sport Injuryjuanito1979No ratings yet
- Osteoarthritis of The Knee CopieDocument20 pagesOsteoarthritis of The Knee CopieNarcisYonutzNo ratings yet
- Sci Bladder ProtocolDocument45 pagesSci Bladder ProtocolAbbas JafarzadehabbasNo ratings yet
- Anterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationDocument31 pagesAnterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationNurul FajriNo ratings yet
- Spine Rehabilitation in 2022 and BeyondDocument276 pagesSpine Rehabilitation in 2022 and BeyondAhmed Abdel MoneimNo ratings yet
- Orthopaedic SplintingDocument52 pagesOrthopaedic SplintingandhitaNo ratings yet
- Excessive Genu Valgum FINALDocument13 pagesExcessive Genu Valgum FINALMeeraNo ratings yet
- Ankle FAQ's: All Your Questions About Ankle Pain AnsweredDocument31 pagesAnkle FAQ's: All Your Questions About Ankle Pain AnsweredGreg DeaNo ratings yet
- Fracture ManagementDocument21 pagesFracture ManagementPatrickk WandererNo ratings yet
- ScoliosisDocument2 pagesScoliosisZai CruzNo ratings yet
- Pes Cavus - PhysiopediaDocument10 pagesPes Cavus - PhysiopediavaishnaviNo ratings yet
- Medical Rehabilitation in Compression FractureDocument32 pagesMedical Rehabilitation in Compression FracturegloriaNo ratings yet
- Name: ID:: Madiha Sayed Nagy. 51859Document12 pagesName: ID:: Madiha Sayed Nagy. 51859drng48No ratings yet
- 10.physiotherapy After Total Knee Arthroplasty PresentationDocument34 pages10.physiotherapy After Total Knee Arthroplasty PresentationAfaf Al Oufi AfafNo ratings yet
- Guide Ankle Foot Orthosis AfoDocument2 pagesGuide Ankle Foot Orthosis AfoAbdul Razzaq AfridiNo ratings yet
- ShoulderDocument3 pagesShoulderjschiro1No ratings yet
- 香港脊醫 Hong Kong Chiropractors Sep 2016Document6 pages香港脊醫 Hong Kong Chiropractors Sep 2016CDAHKNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- Examination of The Knee Joint - RP's Ortho NotesDocument3 pagesExamination of The Knee Joint - RP's Ortho NotesSabari NathNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Approach To The Limping ChildDocument12 pagesApproach To The Limping ChildinfinityonwardNo ratings yet
- Amc Limb FractureDocument10 pagesAmc Limb Fractureffaa100% (1)
- Why Women CheatDocument8 pagesWhy Women CheatGopi Krishna100% (2)
- The Wing Girl Method Cheat SheetDocument8 pagesThe Wing Girl Method Cheat SheetGopi KrishnaNo ratings yet
- Fuck Yes or No: by Mark MansonDocument5 pagesFuck Yes or No: by Mark MansonGopi KrishnaNo ratings yet
- Cashier ResumeDocument1 pageCashier ResumeGopi KrishnaNo ratings yet
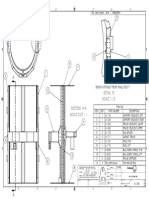
- Detail B Scale 1 / 5: Shown Without Front Ring, Item 7Document1 pageDetail B Scale 1 / 5: Shown Without Front Ring, Item 7Gopi KrishnaNo ratings yet
- Professional 2 Resume LetterDocument2 pagesProfessional 2 Resume LetterGopi KrishnaNo ratings yet
- Odc Letter - Rev 9-4-12 FinalDocument4 pagesOdc Letter - Rev 9-4-12 FinalGopi KrishnaNo ratings yet
- CreativeConfidence PreandintroDocument4 pagesCreativeConfidence PreandintrokophNo ratings yet
- FromDocument1 pageFromGopi KrishnaNo ratings yet
- Professional 2 Resume LetterDocument2 pagesProfessional 2 Resume LetterGopi KrishnaNo ratings yet
- SANIGUARD - 7500 Silane Quat Antimicrobial 99.99 % Protection From Corona Viruses and MicrobesDocument58 pagesSANIGUARD - 7500 Silane Quat Antimicrobial 99.99 % Protection From Corona Viruses and MicrobesKetan GandhiNo ratings yet
- Farmersfz: Agri-Food Supply Chain Start UpDocument2 pagesFarmersfz: Agri-Food Supply Chain Start UpFPOM 2K21No ratings yet
- Part II CH 3Document129 pagesPart II CH 3Davor VeseljkoNo ratings yet
- 18.034 Honors Differential Equations: Mit OpencoursewareDocument4 pages18.034 Honors Differential Equations: Mit Opencoursewarevahid mesicNo ratings yet
- Economic Hubs and Economic Sectors of PakistanDocument2 pagesEconomic Hubs and Economic Sectors of PakistanShahab Naveed RashidNo ratings yet
- Ad360 Port and System RequirementsDocument8 pagesAd360 Port and System RequirementsjrosariocabreraNo ratings yet
- ALKcar BDM100 v1255 Ecu ProgrammerDocument3 pagesALKcar BDM100 v1255 Ecu ProgrammeralkNo ratings yet
- ME2403-Power Plant EngineeringDocument5 pagesME2403-Power Plant EngineeringkrishnabrNo ratings yet
- Getting Started Guide: Model Predictive Control Toolbox™Document174 pagesGetting Started Guide: Model Predictive Control Toolbox™porco gesuNo ratings yet
- Case Study: Banana Plantation Impact On Economy of MindanaoDocument6 pagesCase Study: Banana Plantation Impact On Economy of Mindanaolyramae.dezaNo ratings yet
- JICA's Input For Interim Reporting - 20230120 - Draft - Rev3Document60 pagesJICA's Input For Interim Reporting - 20230120 - Draft - Rev32023kajian sarprasdispardiyNo ratings yet
- V8 (V1.04) Datasheet Rev1.8 - 20230724Document52 pagesV8 (V1.04) Datasheet Rev1.8 - 20230724gaspertrekNo ratings yet
- Karina Nayyar - Senior Tester 8+ Years ExperiencedDocument2 pagesKarina Nayyar - Senior Tester 8+ Years ExperiencedSanam BindraNo ratings yet
- The End of HumanityDocument8 pagesThe End of HumanityDaniel James BarkerNo ratings yet
- Adsorption Kinetic Models: Physical Meanings, Applications, and Solving MethodsDocument18 pagesAdsorption Kinetic Models: Physical Meanings, Applications, and Solving MethodsNórida Pájaro GómezNo ratings yet
- Predictive AnalyticsDocument19 pagesPredictive AnalyticsJosé MundarainNo ratings yet
- Additional Maths Revision NotesDocument87 pagesAdditional Maths Revision NotesSamson YauNo ratings yet
- Stampella 2022Document15 pagesStampella 2022Pablo StampellaNo ratings yet
- 1-Write A Program To Implement The Following Operations On One Dimensional Array A) InsertionDocument19 pages1-Write A Program To Implement The Following Operations On One Dimensional Array A) InsertionAnsh sharmaNo ratings yet
- Non Spore Forming Gram Positive Rods: CorynebacteriumDocument6 pagesNon Spore Forming Gram Positive Rods: CorynebacteriumggzgzhhsNo ratings yet
- BSRM Steels LimitedDocument2 pagesBSRM Steels Limitedashek ishtiak haqNo ratings yet
- CJ4 Avionics 1.01Document36 pagesCJ4 Avionics 1.01Jose Otero De Santiago100% (1)
- Yogesh Aghav 2Document7 pagesYogesh Aghav 2pranjalbaruah8No ratings yet
- Acids and Alkalis WorksheetsDocument42 pagesAcids and Alkalis WorksheetsAFuentesCaballero100% (1)
- BYD P6K-36 335WpDocument1 pageBYD P6K-36 335WpWilson Braga JúniorNo ratings yet
- 8 Engine Terms Every Marine Engineer Should Know - Part 2Document11 pages8 Engine Terms Every Marine Engineer Should Know - Part 2Anonymous fjHSpGNo ratings yet
- Katalog Quot 268 Esk 225 Zbrojovka Uhersk 253 Brod Quot 2021Document61 pagesKatalog Quot 268 Esk 225 Zbrojovka Uhersk 253 Brod Quot 2021Женя АлександровNo ratings yet




































































































Download as ppt, pdf, or txt
You might also like
- Sex God SecretsDocument123 pagesSex God SecretsKhamiss Khouya55% (20)
- 2004 RX8 Parts ManualDocument15 pages2004 RX8 Parts Manualgo0n80% (10)
- Planning and Scheduling of SubstructureDocument81 pagesPlanning and Scheduling of SubstructureHnin Wai Mar Aung100% (3)
- Spine TraumaDocument7 pagesSpine TraumafadlinNo ratings yet
- When To Operate On Spinal Cysts - Dr. WelchDocument57 pagesWhen To Operate On Spinal Cysts - Dr. WelchSaro HerreraNo ratings yet
- Diving Injuries Research Findings and Recommendations For Reducing Catastrophic Injuries PDFDocument273 pagesDiving Injuries Research Findings and Recommendations For Reducing Catastrophic Injuries PDFcarlosNo ratings yet
- Steven Schick Learning Brian Ferneyhough's Bone Alphabet PDFDocument23 pagesSteven Schick Learning Brian Ferneyhough's Bone Alphabet PDFRokitMan_No ratings yet
- Forearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandForearm Fractures, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Turf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandTurf Toe, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diabetic FootDocument4 pagesDiabetic FoothegazyscribdNo ratings yet
- DR G Avinash Rao Fellow in Hand and Microsurgery: ArthrogryposisDocument74 pagesDR G Avinash Rao Fellow in Hand and Microsurgery: Arthrogryposisavinashrao39100% (1)
- Lower Extremity DisordersDocument25 pagesLower Extremity DisordersJameson87No ratings yet
- Biomechanics of Volleyball SpikesDocument20 pagesBiomechanics of Volleyball SpikesMujid Benazer100% (2)
- Sports Therapy Dissertation IdeasDocument6 pagesSports Therapy Dissertation IdeasCustomizedPaperSingapore100% (1)
- ACL Injuries in Female Athletes PowerpointDocument8 pagesACL Injuries in Female Athletes Powerpointrupinder24No ratings yet
- MF2 - Spinal Cord InjuryDocument43 pagesMF2 - Spinal Cord InjuryAnnbe BarteNo ratings yet
- Orthopaedic EmergenciesDocument12 pagesOrthopaedic EmergenciesUhuebor DavidNo ratings yet
- Musculoskeletal Disease Associated With Diabetes MellitusDocument290 pagesMusculoskeletal Disease Associated With Diabetes Mellituscharanmann9165No ratings yet
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Document46 pagesPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- Managing Psychiatric Patients in The EDDocument28 pagesManaging Psychiatric Patients in The EDfadiNo ratings yet
- Congenital Dysplasia & DislocatiDocument558 pagesCongenital Dysplasia & DislocatiWilson A. QuinteroNo ratings yet
- Injuries, Risk Factors and Prevention Initiatives in Youth SportDocument27 pagesInjuries, Risk Factors and Prevention Initiatives in Youth SportDonny KurniawanNo ratings yet
- Posterior Tibialis Tendon Dysfunction (PTTD)Document11 pagesPosterior Tibialis Tendon Dysfunction (PTTD)bigpawn13No ratings yet
- AclDocument20 pagesAclDanny OtNo ratings yet
- Chapter 55 - Pelvic Trauma Episode OverviewDocument8 pagesChapter 55 - Pelvic Trauma Episode OverviewKadek Adi WigunaNo ratings yet
- Crush InjuryDocument4 pagesCrush InjuryMuhammad Nur ArifinNo ratings yet
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Document59 pagesTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNo ratings yet
- Peripheral Nerve Injury: J. Navin KumarDocument100 pagesPeripheral Nerve Injury: J. Navin Kumarpuravi91No ratings yet
- Limping Child: Department of Orthopaedics Afmc, PuneDocument101 pagesLimping Child: Department of Orthopaedics Afmc, Punerithesh ramachandranNo ratings yet
- Open Fracture: A Presentation byDocument44 pagesOpen Fracture: A Presentation byNur Liyana Ahmad ZakiNo ratings yet
- Dance Injuries-Foot and AnkleDocument7 pagesDance Injuries-Foot and Ankleapi-198787605100% (1)
- DDH 2Document3 pagesDDH 2monique_munoz_2No ratings yet
- Rehabilitation Management For Rheumatoid Arthritis Patients 2Document19 pagesRehabilitation Management For Rheumatoid Arthritis Patients 2Jothiprasanna KNo ratings yet
- Muscular Dystrophy Fact SheetDocument2 pagesMuscular Dystrophy Fact Sheetmdhaddock87100% (1)
- MPT SyllabusDocument8 pagesMPT Syllabusbluesky_jawedNo ratings yet
- Perthes Disease: Mohamed Hamood MohamedDocument4 pagesPerthes Disease: Mohamed Hamood MohamedMohamed HamoodNo ratings yet
- Fractures in ChildrenDocument5 pagesFractures in ChildrenAbigaille ChuaNo ratings yet
- Congenital Hand AnomaliesDocument59 pagesCongenital Hand AnomaliesnessyuarniNo ratings yet
- 2-Physiotherapy For FracturesDocument17 pages2-Physiotherapy For FracturesJuanitoCabatañaLimIIINo ratings yet
- 6-Fractures and Joints Dislocations ManagementDocument91 pages6-Fractures and Joints Dislocations ManagementMUGISHA GratienNo ratings yet
- What Is Spinal StenosisDocument10 pagesWhat Is Spinal Stenosismariamel31No ratings yet
- Foot Ankle InjuriesDocument55 pagesFoot Ankle InjuriesMark Jan HorstNo ratings yet
- What Is Sport InjuryDocument6 pagesWhat Is Sport Injuryjuanito1979No ratings yet
- Osteoarthritis of The Knee CopieDocument20 pagesOsteoarthritis of The Knee CopieNarcisYonutzNo ratings yet
- Sci Bladder ProtocolDocument45 pagesSci Bladder ProtocolAbbas JafarzadehabbasNo ratings yet
- Anterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationDocument31 pagesAnterior Cruciate Ligament Reconstruction: Mardani Kivi M. M.D. Presentation Designed For Nurses EducationNurul FajriNo ratings yet
- Spine Rehabilitation in 2022 and BeyondDocument276 pagesSpine Rehabilitation in 2022 and BeyondAhmed Abdel MoneimNo ratings yet
- Orthopaedic SplintingDocument52 pagesOrthopaedic SplintingandhitaNo ratings yet
- Excessive Genu Valgum FINALDocument13 pagesExcessive Genu Valgum FINALMeeraNo ratings yet
- Ankle FAQ's: All Your Questions About Ankle Pain AnsweredDocument31 pagesAnkle FAQ's: All Your Questions About Ankle Pain AnsweredGreg DeaNo ratings yet
- Fracture ManagementDocument21 pagesFracture ManagementPatrickk WandererNo ratings yet
- ScoliosisDocument2 pagesScoliosisZai CruzNo ratings yet
- Pes Cavus - PhysiopediaDocument10 pagesPes Cavus - PhysiopediavaishnaviNo ratings yet
- Medical Rehabilitation in Compression FractureDocument32 pagesMedical Rehabilitation in Compression FracturegloriaNo ratings yet
- Name: ID:: Madiha Sayed Nagy. 51859Document12 pagesName: ID:: Madiha Sayed Nagy. 51859drng48No ratings yet
- 10.physiotherapy After Total Knee Arthroplasty PresentationDocument34 pages10.physiotherapy After Total Knee Arthroplasty PresentationAfaf Al Oufi AfafNo ratings yet
- Guide Ankle Foot Orthosis AfoDocument2 pagesGuide Ankle Foot Orthosis AfoAbdul Razzaq AfridiNo ratings yet
- ShoulderDocument3 pagesShoulderjschiro1No ratings yet
- 香港脊醫 Hong Kong Chiropractors Sep 2016Document6 pages香港脊醫 Hong Kong Chiropractors Sep 2016CDAHKNo ratings yet
- Erbs PalsyDocument9 pagesErbs PalsyVatsalVermaNo ratings yet
- Examination of The Knee Joint - RP's Ortho NotesDocument3 pagesExamination of The Knee Joint - RP's Ortho NotesSabari NathNo ratings yet
- Compartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandCompartment Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Approach To The Limping ChildDocument12 pagesApproach To The Limping ChildinfinityonwardNo ratings yet
- Amc Limb FractureDocument10 pagesAmc Limb Fractureffaa100% (1)
- Why Women CheatDocument8 pagesWhy Women CheatGopi Krishna100% (2)
- The Wing Girl Method Cheat SheetDocument8 pagesThe Wing Girl Method Cheat SheetGopi KrishnaNo ratings yet
- Fuck Yes or No: by Mark MansonDocument5 pagesFuck Yes or No: by Mark MansonGopi KrishnaNo ratings yet
- Cashier ResumeDocument1 pageCashier ResumeGopi KrishnaNo ratings yet
- Detail B Scale 1 / 5: Shown Without Front Ring, Item 7Document1 pageDetail B Scale 1 / 5: Shown Without Front Ring, Item 7Gopi KrishnaNo ratings yet
- Professional 2 Resume LetterDocument2 pagesProfessional 2 Resume LetterGopi KrishnaNo ratings yet
- Odc Letter - Rev 9-4-12 FinalDocument4 pagesOdc Letter - Rev 9-4-12 FinalGopi KrishnaNo ratings yet
- CreativeConfidence PreandintroDocument4 pagesCreativeConfidence PreandintrokophNo ratings yet
- FromDocument1 pageFromGopi KrishnaNo ratings yet
- Professional 2 Resume LetterDocument2 pagesProfessional 2 Resume LetterGopi KrishnaNo ratings yet
- SANIGUARD - 7500 Silane Quat Antimicrobial 99.99 % Protection From Corona Viruses and MicrobesDocument58 pagesSANIGUARD - 7500 Silane Quat Antimicrobial 99.99 % Protection From Corona Viruses and MicrobesKetan GandhiNo ratings yet
- Farmersfz: Agri-Food Supply Chain Start UpDocument2 pagesFarmersfz: Agri-Food Supply Chain Start UpFPOM 2K21No ratings yet
- Part II CH 3Document129 pagesPart II CH 3Davor VeseljkoNo ratings yet
- 18.034 Honors Differential Equations: Mit OpencoursewareDocument4 pages18.034 Honors Differential Equations: Mit Opencoursewarevahid mesicNo ratings yet
- Economic Hubs and Economic Sectors of PakistanDocument2 pagesEconomic Hubs and Economic Sectors of PakistanShahab Naveed RashidNo ratings yet
- Ad360 Port and System RequirementsDocument8 pagesAd360 Port and System RequirementsjrosariocabreraNo ratings yet
- ALKcar BDM100 v1255 Ecu ProgrammerDocument3 pagesALKcar BDM100 v1255 Ecu ProgrammeralkNo ratings yet
- ME2403-Power Plant EngineeringDocument5 pagesME2403-Power Plant EngineeringkrishnabrNo ratings yet
- Getting Started Guide: Model Predictive Control Toolbox™Document174 pagesGetting Started Guide: Model Predictive Control Toolbox™porco gesuNo ratings yet
- Case Study: Banana Plantation Impact On Economy of MindanaoDocument6 pagesCase Study: Banana Plantation Impact On Economy of Mindanaolyramae.dezaNo ratings yet
- JICA's Input For Interim Reporting - 20230120 - Draft - Rev3Document60 pagesJICA's Input For Interim Reporting - 20230120 - Draft - Rev32023kajian sarprasdispardiyNo ratings yet
- V8 (V1.04) Datasheet Rev1.8 - 20230724Document52 pagesV8 (V1.04) Datasheet Rev1.8 - 20230724gaspertrekNo ratings yet
- Karina Nayyar - Senior Tester 8+ Years ExperiencedDocument2 pagesKarina Nayyar - Senior Tester 8+ Years ExperiencedSanam BindraNo ratings yet
- The End of HumanityDocument8 pagesThe End of HumanityDaniel James BarkerNo ratings yet
- Adsorption Kinetic Models: Physical Meanings, Applications, and Solving MethodsDocument18 pagesAdsorption Kinetic Models: Physical Meanings, Applications, and Solving MethodsNórida Pájaro GómezNo ratings yet
- Predictive AnalyticsDocument19 pagesPredictive AnalyticsJosé MundarainNo ratings yet
- Additional Maths Revision NotesDocument87 pagesAdditional Maths Revision NotesSamson YauNo ratings yet
- Stampella 2022Document15 pagesStampella 2022Pablo StampellaNo ratings yet
- 1-Write A Program To Implement The Following Operations On One Dimensional Array A) InsertionDocument19 pages1-Write A Program To Implement The Following Operations On One Dimensional Array A) InsertionAnsh sharmaNo ratings yet
- Non Spore Forming Gram Positive Rods: CorynebacteriumDocument6 pagesNon Spore Forming Gram Positive Rods: CorynebacteriumggzgzhhsNo ratings yet
- BSRM Steels LimitedDocument2 pagesBSRM Steels Limitedashek ishtiak haqNo ratings yet
- CJ4 Avionics 1.01Document36 pagesCJ4 Avionics 1.01Jose Otero De Santiago100% (1)
- Yogesh Aghav 2Document7 pagesYogesh Aghav 2pranjalbaruah8No ratings yet
- Acids and Alkalis WorksheetsDocument42 pagesAcids and Alkalis WorksheetsAFuentesCaballero100% (1)
- BYD P6K-36 335WpDocument1 pageBYD P6K-36 335WpWilson Braga JúniorNo ratings yet
- 8 Engine Terms Every Marine Engineer Should Know - Part 2Document11 pages8 Engine Terms Every Marine Engineer Should Know - Part 2Anonymous fjHSpGNo ratings yet
- Katalog Quot 268 Esk 225 Zbrojovka Uhersk 253 Brod Quot 2021Document61 pagesKatalog Quot 268 Esk 225 Zbrojovka Uhersk 253 Brod Quot 2021Женя АлександровNo ratings yet