Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 06 237046 001 - BDDocument1 page06 237046 001 - BDcarlos yepezNo ratings yet
- Nyeri Kepala IAFKU, DR Betty, SPSDocument43 pagesNyeri Kepala IAFKU, DR Betty, SPSMuhammad AsrizalNo ratings yet
- 4215 10613 1 PB PDFDocument9 pages4215 10613 1 PB PDFMuhammad AsrizalNo ratings yet
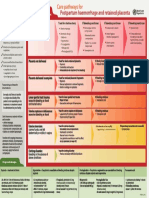
- Hemorragic Post PartumDocument35 pagesHemorragic Post PartumMuhammad AsrizalNo ratings yet
- Professional Med J Q 2014 21 6 1117 1121Document5 pagesProfessional Med J Q 2014 21 6 1117 1121Muhammad AsrizalNo ratings yet
- 1756 0500 6 116Document6 pages1756 0500 6 116Muhammad AsrizalNo ratings yet
- Uterus Soft and Relaxed: Uterine AtonyDocument1 pageUterus Soft and Relaxed: Uterine AtonyMuhammad AsrizalNo ratings yet
- Clinical StudyDocument7 pagesClinical StudyMuhammad AsrizalNo ratings yet
- Up Date ScreeningDocument87 pagesUp Date ScreeningMuhammad AsrizalNo ratings yet
- Iec 61215 61646 en PDFDocument5 pagesIec 61215 61646 en PDFMarysol AyalaNo ratings yet
- 501c3.guidelines Issued by The IRSDocument31 pages501c3.guidelines Issued by The IRSThe Department of Official InformationNo ratings yet
- Common Proper Noun Worksheet Underlining IntermediateDocument1 pageCommon Proper Noun Worksheet Underlining Intermediaterazeen_93No ratings yet
- Yataş Bedding - CatalogDocument87 pagesYataş Bedding - CatalogeftzaeNo ratings yet
- Chemical Method Sterilization Disinfection Powerpoint PresentationDocument33 pagesChemical Method Sterilization Disinfection Powerpoint PresentationVohn Archie EdjanNo ratings yet
- Basic CalculationDocument89 pagesBasic CalculationUsamNo ratings yet
- Fat Loss ProgramDocument2 pagesFat Loss Programrifkarofiah1No ratings yet
- Sikawrap®-900 C: Product Data SheetDocument4 pagesSikawrap®-900 C: Product Data SheetnovitaapriyaniNo ratings yet
- Physical Activity Scale For The Elderly Pase .4Document6 pagesPhysical Activity Scale For The Elderly Pase .4Erna UtamiNo ratings yet
- Implementing A Digital Transformation: November 2018Document5 pagesImplementing A Digital Transformation: November 2018Hasti YektaNo ratings yet
- Chemical Hazard Bulletin: ArgonDocument1 pageChemical Hazard Bulletin: ArgonHaleemUrRashidBangashNo ratings yet
- Induksi Kalus Krisan (Chrysanthemum Morifolium Ramat.) Dengan Penambahan Berbagai Kombinasi Zat Pengatur Tumbuh (ZPT)Document14 pagesInduksi Kalus Krisan (Chrysanthemum Morifolium Ramat.) Dengan Penambahan Berbagai Kombinasi Zat Pengatur Tumbuh (ZPT)JackNo ratings yet
- O Level OrientationDocument4 pagesO Level OrientationKim NisarNo ratings yet
- DSTC 1586861258Document139 pagesDSTC 1586861258Manjeet Thakur100% (2)
- TDS - RHEOSPERSE™ S 300 - en - WWDocument1 pageTDS - RHEOSPERSE™ S 300 - en - WWUlaş ÇuğuNo ratings yet
- Đề số 1Document4 pagesĐề số 1LanChiVũ0% (1)
- Quezon City University 673 Quirino Highway, San Bartolome, Novaliches, Quezon City, PhilippinesDocument6 pagesQuezon City University 673 Quirino Highway, San Bartolome, Novaliches, Quezon City, Philippinesshayn delapenaNo ratings yet
- Quick Hoops™ High Tunnel Bender: Instruction Manual For 9018Document54 pagesQuick Hoops™ High Tunnel Bender: Instruction Manual For 9018glue2No ratings yet
- User Manual Bosch Serie - 4 WTB86238EE (English - 10 Pages)Document2 pagesUser Manual Bosch Serie - 4 WTB86238EE (English - 10 Pages)Erik NagyNo ratings yet
- 2804 June05ms PDFDocument8 pages2804 June05ms PDFTazDhaliwalNo ratings yet
- SujoodDocument7 pagesSujoodapi-19729317No ratings yet
- Osteological ReproductionsDocument88 pagesOsteological ReproductionsAntonioNo ratings yet
- Compressor PresentationDocument24 pagesCompressor PresentationPrashant Kumar mishraNo ratings yet
- De Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NDocument2 pagesDe Ce of Eterm Emen F The Mina NT by e Solu Ation y Pho Ubiliz Nofa Otom Zed P Alum Metric Prod Inum C Titr Uct Min Ratio NRomy Iván Cruz VillarroelNo ratings yet
- ECG LictureDocument25 pagesECG LictureALi NursingNo ratings yet
- EE - exam.PowerSystem - Feb 2 2015-2Document3 pagesEE - exam.PowerSystem - Feb 2 2015-2giophilipNo ratings yet
- Scientific AmericanDocument151 pagesScientific AmericanGutenberg.orgNo ratings yet
- 1 Bengaluru Urban Dist:: Sl. No. Industrial Area Date of Revision (B.M.Date) Prevailing Price/Acre (Rs. in Lakhs) 1 2 3 4Document8 pages1 Bengaluru Urban Dist:: Sl. No. Industrial Area Date of Revision (B.M.Date) Prevailing Price/Acre (Rs. in Lakhs) 1 2 3 4Raju BMNo ratings yet
- Data Sheet: Dulcodes 1 X 80 LP Operating Parameters in Accordance With DVGW Worksheet W 294-1Document2 pagesData Sheet: Dulcodes 1 X 80 LP Operating Parameters in Accordance With DVGW Worksheet W 294-1Willian A. Palacio MurilloNo ratings yet