Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Case Study of La Posta Mexican RestaurantsDocument1 pageCase Study of La Posta Mexican RestaurantsFatima Atiq80% (5)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Precipitation ProcessesDocument2 pagesPrecipitation ProcessesThembi Matebula100% (1)
- BS 57 (1951)Document23 pagesBS 57 (1951)dapsiduNo ratings yet
- Biomass and Bioenergy: Research PaperDocument18 pagesBiomass and Bioenergy: Research PaperSaleha QuadsiaNo ratings yet
- Effects of Sulphur and Zinc Applications On Growth and Nutrition of Bread Wheat in Calcareous Clay Loam SoilDocument7 pagesEffects of Sulphur and Zinc Applications On Growth and Nutrition of Bread Wheat in Calcareous Clay Loam SoilSaleha QuadsiaNo ratings yet
- Journal of The Energy Institute: Adisak Pattiya, Suntorn SuttibakDocument10 pagesJournal of The Energy Institute: Adisak Pattiya, Suntorn SuttibakSaleha QuadsiaNo ratings yet
- The Impact of Accounting Information Systems AIS oDocument20 pagesThe Impact of Accounting Information Systems AIS oSaleha QuadsiaNo ratings yet
- Supplementary Material: For ManuscriptDocument15 pagesSupplementary Material: For ManuscriptSaleha QuadsiaNo ratings yet
- Basic Challenges of Organizational DesignDocument48 pagesBasic Challenges of Organizational DesignSaleha QuadsiaNo ratings yet
- Au-Sn SLID Bonding EMPC2009 PresentationDocument17 pagesAu-Sn SLID Bonding EMPC2009 PresentationSaleha Quadsia100% (1)
- 3.2.1 Example - WBS, V 1.0.1Document3 pages3.2.1 Example - WBS, V 1.0.1Saleha Quadsia100% (1)
- Diet Plan Week 1: Breakfast Lunch Dinner Snacks ExerciseDocument16 pagesDiet Plan Week 1: Breakfast Lunch Dinner Snacks ExerciseSaleha QuadsiaNo ratings yet
- Eigenfrequencies and Q Factor in The Geometrical Theory of Whispering-Gallery ModesDocument6 pagesEigenfrequencies and Q Factor in The Geometrical Theory of Whispering-Gallery ModesSaleha QuadsiaNo ratings yet
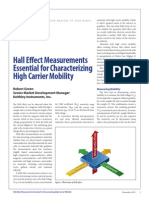
- Hall Effect Measurements Essential For Characterizing High Carrier MobilityDocument4 pagesHall Effect Measurements Essential For Characterizing High Carrier MobilitySaleha QuadsiaNo ratings yet
- Course Schedule2014 PreliminaryDocument1 pageCourse Schedule2014 PreliminarySaleha QuadsiaNo ratings yet
- Conflict Studies Research CentreDocument10 pagesConflict Studies Research CentreSaleha QuadsiaNo ratings yet
- Biostat IntroductionDocument31 pagesBiostat IntroductionteklayNo ratings yet
- WH2009 WaterHorseCatalogDocument132 pagesWH2009 WaterHorseCatalogAiko FeroNo ratings yet
- From Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityDocument14 pagesFrom Rice To Apple-Pear Style - An Ecocritical Approach To China's Korean Ethnic MinorityLing LIUNo ratings yet
- Ibot vs. TaycoDocument2 pagesIbot vs. TaycoMishal Oisin100% (1)
- Persistent System Feedback 2018Document2 pagesPersistent System Feedback 2018sunikesh shuklaNo ratings yet
- SUBHIKSHADocument12 pagesSUBHIKSHAAkshat ChaturvediNo ratings yet
- Ijleo S 23 06033Document26 pagesIjleo S 23 06033Laura DiazNo ratings yet
- American Heart Association PPT - AIHA Webinar - FinalDocument49 pagesAmerican Heart Association PPT - AIHA Webinar - FinalVina WineNo ratings yet
- CPR Test - SummaryDocument2 pagesCPR Test - Summaryas0537 31No ratings yet
- GSM System Fundamental TrainingDocument144 pagesGSM System Fundamental Trainingmansonbazzokka100% (2)
- Defense Support of Civil Authorities (Dsca) : This Briefing IsDocument15 pagesDefense Support of Civil Authorities (Dsca) : This Briefing IsChris WhiteheadNo ratings yet
- De Claro SinglesDocument96 pagesDe Claro Singlesapi-3701495No ratings yet
- CDS13084 M84 EcuDocument3 pagesCDS13084 M84 EcuAbdullah AtfNo ratings yet
- Marcopolo Is A Leading Brazilian Bus Body ManufacturerDocument4 pagesMarcopolo Is A Leading Brazilian Bus Body ManufacturerCH NAIRNo ratings yet
- Advisor Webcast - Customizing The Workflows in Oracle EBS ProcurementDocument53 pagesAdvisor Webcast - Customizing The Workflows in Oracle EBS ProcurementhgopalanNo ratings yet
- Good, Bad and Ugly Process Burner FlamesDocument3 pagesGood, Bad and Ugly Process Burner Flamesratninp9368No ratings yet
- Material ManagementDocument20 pagesMaterial Managementgkataria110100% (1)
- WEDNESDAYDocument11 pagesWEDNESDAYShubham DwivediNo ratings yet
- Database Systems, Eleventh Edition by Coronel Morris, Course Technology 2014Document5 pagesDatabase Systems, Eleventh Edition by Coronel Morris, Course Technology 2014LaluMohan KcNo ratings yet
- The Silt Verses - Chapter 21 TranscriptDocument32 pagesThe Silt Verses - Chapter 21 TranscriptVictória MoraesNo ratings yet
- Common Service Data Model (CSDM) 3.0 White PaperDocument31 pagesCommon Service Data Model (CSDM) 3.0 White PaperЕвгения МазинаNo ratings yet
- Dvp-Es2 Ss2 Sa2 Sx2-Program o en 20110302Document609 pagesDvp-Es2 Ss2 Sa2 Sx2-Program o en 20110302puskyboyNo ratings yet
- Séquence 2: Sciences Et Techniques, Promesses Et Défis: S 2 - T I S SDocument17 pagesSéquence 2: Sciences Et Techniques, Promesses Et Défis: S 2 - T I S SAsmaa AssoumaNo ratings yet
- 3.4 Loader Design Options: 3.4.1 Linkage EditorsDocument25 pages3.4 Loader Design Options: 3.4.1 Linkage EditorsEñg Šǻmèr ǮrắBiųâtNo ratings yet
- Kyle Rowe NC PetitionDocument4 pagesKyle Rowe NC PetitionjustinmcNo ratings yet
- ConcordDocument2 pagesConcordLiwang Ulama UtamaNo ratings yet
- Mage Wars: Variant With No Dice: Basic RulesDocument8 pagesMage Wars: Variant With No Dice: Basic RulesMáté BoaNo ratings yet