Download as ppt, pdf, or txt
You might also like
- NCP - Fluid Volume DeficitDocument2 pagesNCP - Fluid Volume DeficitMarielle Osalvo83% (59)
- Anesthaesia and Intensive CareDocument139 pagesAnesthaesia and Intensive CareIvan Kurniadi100% (2)
- Sepsis - 3Document36 pagesSepsis - 3Mohd Ekhwan DarusNo ratings yet
- Anaesthesia & Intensive Care: For Fcai, Frca EdaicDocument139 pagesAnaesthesia & Intensive Care: For Fcai, Frca EdaicMuhammad Farid100% (2)
- CASE Melanoma MalignaDocument29 pagesCASE Melanoma Malignaushagi-chanNo ratings yet
- Painted Heart From Painted Skin Movie Complete Piano SheetDocument5 pagesPainted Heart From Painted Skin Movie Complete Piano Sheetushagi-chanNo ratings yet
- Penatalaksanaan CAPDocument31 pagesPenatalaksanaan CAPridhoNo ratings yet
- Pulmonary InfectionsDocument16 pagesPulmonary InfectionsFawad AhmedNo ratings yet
- Case Studies of Lower Respiratory Tract InfectionsDocument25 pagesCase Studies of Lower Respiratory Tract InfectionsMarianNo ratings yet
- Management of CAP: Recent Guideline in Daily PractisDocument38 pagesManagement of CAP: Recent Guideline in Daily PractisNila hermawatiNo ratings yet
- FeverDocument27 pagesFeverTilaye GebruNo ratings yet
- Surviving SepsisDocument50 pagesSurviving SepsisManish AdhikariNo ratings yet
- Pneumonia: Recent Evidence Based UpdatesDocument30 pagesPneumonia: Recent Evidence Based UpdatesAli AzamNo ratings yet
- PCAP GuidelinesDocument20 pagesPCAP GuidelinesPatricia Anne Collantes90% (20)
- Pneumonia GuidelinesDocument4 pagesPneumonia GuidelinesFatkhul Ali ImronNo ratings yet
- Management of Community Acquired PneumoniaDocument2 pagesManagement of Community Acquired Pneumoniaab_ghaffar_latiffi9337No ratings yet
- Neutropenic SepsisDocument38 pagesNeutropenic SepsisYS NateNo ratings yet
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocument1 pageGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNo ratings yet
- Case Presentation MineDocument30 pagesCase Presentation MineAshman AshNo ratings yet
- Neutropenic Fever Empiric TherapyDocument5 pagesNeutropenic Fever Empiric TherapyRominaPulvermüllerSalvatierraNo ratings yet
- Pcap FDDocument22 pagesPcap FDJeanne Mae Lee AfallaNo ratings yet
- Sumit Bhutani: Neutropenic FeverDocument46 pagesSumit Bhutani: Neutropenic Feversumit240677No ratings yet
- Pneumonia: Abhishek Achar Ly TranDocument34 pagesPneumonia: Abhishek Achar Ly TranRAPURU BHARGAVINo ratings yet
- Cme: Sirs and Modsfinal 3Document26 pagesCme: Sirs and Modsfinal 3asraf amirullahNo ratings yet
- Community Acquired Pneumonia: - Hafsah GhazaliDocument19 pagesCommunity Acquired Pneumonia: - Hafsah GhazaliloribyseaNo ratings yet
- Princy N. Kumar, MDDocument8 pagesPrincy N. Kumar, MDfeedodeedoNo ratings yet
- Farmakoterapi Pada SepsisDocument36 pagesFarmakoterapi Pada SepsisNathaniaNo ratings yet
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- COVID-19 Antiviral TX Guidance 4-22-2020Document23 pagesCOVID-19 Antiviral TX Guidance 4-22-2020Lydia IsaacNo ratings yet
- 07 - 10 - 21 Treatment of Covid 19 InfectionDocument26 pages07 - 10 - 21 Treatment of Covid 19 InfectionStonefalconNo ratings yet
- Management of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Document4 pagesManagement of Adult Febrile Neutropenia: 15011500-10123 99 Street Edmonton, Alberta T5J 3H1Tio Prima SNo ratings yet
- Antibiotic Guidelines Elderly UTI Rationale C Diff & PID Amended 15.09.11 UTI & Flu Amended 04.10 OM Ref 11.11Document29 pagesAntibiotic Guidelines Elderly UTI Rationale C Diff & PID Amended 15.09.11 UTI & Flu Amended 04.10 OM Ref 11.11Syed Yasir HusainNo ratings yet
- Hospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Document32 pagesHospital-Acquired Pneumonia (HAP) & Ventilator-Associated Pneumonia (VAP) Healthcare-Associated Pneumonia (HCAP)Kamel HadyNo ratings yet
- Diagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineDocument57 pagesDiagnosis & Treatment of Healthcare-Associated Pneumonia: Beyond The GuidelineKei MiyazakiNo ratings yet
- Febrile Neutropenia: Dr. Abdelkareem Wedaa EltohamyDocument31 pagesFebrile Neutropenia: Dr. Abdelkareem Wedaa Eltohamyjehemir100% (1)
- COVID 19 MG Protocol FinalDocument13 pagesCOVID 19 MG Protocol FinalajiNo ratings yet
- Evms Critical Care Covid-19 Management Protocol: Paul Marik, MDDocument11 pagesEvms Critical Care Covid-19 Management Protocol: Paul Marik, MDPrashanta Barman Palas100% (1)
- Coursera ABSDocument8 pagesCoursera ABSevanoNo ratings yet
- Community Acquired Pneumonia: - Hafsah GhazaliDocument19 pagesCommunity Acquired Pneumonia: - Hafsah GhazaliCIk ChaNo ratings yet
- Indications of ICU Admission and ICU Management of COVID 19 NEWDocument27 pagesIndications of ICU Admission and ICU Management of COVID 19 NEWMidhat FatmaNo ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument23 pagesEVMS Critical Care COVID-19 ProtocoldarwinNo ratings yet
- Pneumonia 1Document31 pagesPneumonia 1Parushhni NandhagopalNo ratings yet
- CovidDocument31 pagesCovidShaheen SultanNo ratings yet
- สำเนา pneDocument32 pagesสำเนา pneThanawat SimaNo ratings yet
- Lower Respiratory Tract Infection - CAP: Therapy II - LabDocument14 pagesLower Respiratory Tract Infection - CAP: Therapy II - Labsameh EidNo ratings yet
- Principles of Antibiotic TherapyDocument26 pagesPrinciples of Antibiotic TherapyHaroun drissNo ratings yet
- Sepsis and Septic Shock Management Guidelines 2019: Insp. Dr. Sunder Chapagain Nepal APF Hospital KathmanduDocument33 pagesSepsis and Septic Shock Management Guidelines 2019: Insp. Dr. Sunder Chapagain Nepal APF Hospital KathmanduKHAIRUL REDZUANNo ratings yet
- Pneumonia 1 2015Document2 pagesPneumonia 1 2015Min MawNo ratings yet
- Pediatrics MS WordDocument13 pagesPediatrics MS WordSamhitha SharmaNo ratings yet
- Therapy 2 ch4Document74 pagesTherapy 2 ch4Emad MustafaNo ratings yet
- Protocols Sepsis Treatment Stony BrookDocument6 pagesProtocols Sepsis Treatment Stony BrookVicky Chrystine SianiparNo ratings yet
- Habits Are Some of The Strategies RecommendedDocument30 pagesHabits Are Some of The Strategies Recommendedmd.dascalescu2486No ratings yet
- Acute Severe Asthma in AdultsDocument3 pagesAcute Severe Asthma in AdultssobanNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument17 pagesEVMS Critical Care COVID-19 ProtocolInternos YopalNo ratings yet
- GDL Fever OncologyDocument16 pagesGDL Fever OncologyZaini GhazaliNo ratings yet
- Evms Critical Care Covid-19 Management ProtocolDocument30 pagesEvms Critical Care Covid-19 Management ProtocolUsman ShoukatNo ratings yet
- PCAP GuidelinesDocument20 pagesPCAP GuidelinesApril Rae BarairoNo ratings yet
- Pneumonia Management ProtocolDocument2 pagesPneumonia Management Protocolsky nuts100% (1)
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- TREATMENT Bacterial MeningitisDocument32 pagesTREATMENT Bacterial MeningitisironNo ratings yet
- COVID 19 FactsDocument27 pagesCOVID 19 FactsgjpaqueoNo ratings yet
- Labs & Imaging for Primary Eye Care: Optometry In Full ScopeFrom EverandLabs & Imaging for Primary Eye Care: Optometry In Full ScopeNo ratings yet
- Nama: Juniawati Tempat/Tanggal Lahir: BANDUNG, 14/06/1991 Nomor Pokok/NRP: 0910088 Alamat: CIBADAK 309 BANDUNG 40231 Program Studi: MedicineDocument3 pagesNama: Juniawati Tempat/Tanggal Lahir: BANDUNG, 14/06/1991 Nomor Pokok/NRP: 0910088 Alamat: CIBADAK 309 BANDUNG 40231 Program Studi: Medicineushagi-chanNo ratings yet
- Jurnal DR Harry GustianDocument3 pagesJurnal DR Harry Gustianushagi-chanNo ratings yet
- (Ocimum Basilicum Linn.) ON MOSQUITO LARVAE Culex SP.: Larvicidal Test of Basil Leaves OilDocument1 page(Ocimum Basilicum Linn.) ON MOSQUITO LARVAE Culex SP.: Larvicidal Test of Basil Leaves Oilushagi-chanNo ratings yet
- Differential DiagnosisDocument4 pagesDifferential Diagnosisushagi-chanNo ratings yet
- Thyroid Disease During PregnancyDocument15 pagesThyroid Disease During PregnancyAnonymous ysrxggk21cNo ratings yet
- Epilepsy in Children With Cerebral PalsyDocument6 pagesEpilepsy in Children With Cerebral PalsyTiara Renita LestariNo ratings yet
- CelecoxibDocument3 pagesCelecoxibapi-3797941No ratings yet
- What Is ThrombocytosisDocument3 pagesWhat Is ThrombocytosisFred C. MirandaNo ratings yet
- Frozen Shoulder RevisedDocument17 pagesFrozen Shoulder Revisednerissa arvianaNo ratings yet
- Cancer ImmunologyDocument12 pagesCancer ImmunologyFreddy TorresNo ratings yet
- B - Cracked Tooth SyndromeDocument8 pagesB - Cracked Tooth SyndromeDavid TaylorNo ratings yet
- Chest Wall, Lung, Mediastinum, and Pleura: Trachea AnatomyDocument3 pagesChest Wall, Lung, Mediastinum, and Pleura: Trachea AnatomyNur SulistiyaningsihNo ratings yet
- Anti Protozoal AgentsDocument37 pagesAnti Protozoal AgentsGunjan YadavNo ratings yet
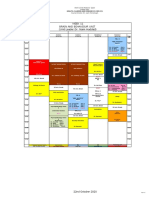
- Week 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)Document1 pageWeek 11 Brain and Behaviour Unit (Unit Leader:Dr. Naim Haddad)f3er3No ratings yet
- 2010 - 2016 With AnswersDocument806 pages2010 - 2016 With AnswersIbrahim Abueltaif83% (6)
- 2020 Bonitas Product BrochureDocument76 pages2020 Bonitas Product BrochuredeenpillayNo ratings yet
- New PPT For HepatitisDocument88 pagesNew PPT For HepatitisPriya100% (2)
- Think Right Now! - I Am Healed NowDocument3 pagesThink Right Now! - I Am Healed NowvaltroduoNo ratings yet
- General Parasitology L2Document27 pagesGeneral Parasitology L2kayse abtidoonNo ratings yet
- KAC Form X Course Registration 17 and Below JUNE2022Document5 pagesKAC Form X Course Registration 17 and Below JUNE2022ALEX SARAOSOSNo ratings yet
- J.P Rizal Ext., West Rembo, Makati City: Personal Safety ProtocolDocument5 pagesJ.P Rizal Ext., West Rembo, Makati City: Personal Safety Protocoljames bonfNo ratings yet
- Monsoon Illnesses-Malaria: Signs and SymptomsDocument1 pageMonsoon Illnesses-Malaria: Signs and SymptomsDisha AgashiwalaNo ratings yet
- Patient Medication Profile and Medication Orders Medical HistoryDocument2 pagesPatient Medication Profile and Medication Orders Medical HistoryLyod BalagasayNo ratings yet
- College of Nursing - NCM 117 1Document36 pagesCollege of Nursing - NCM 117 1joanneNo ratings yet
- Faisal ImranDocument2 pagesFaisal ImranSharjeel AhmedNo ratings yet
- Endoxan: List of ExcipientsDocument4 pagesEndoxan: List of ExcipientsBashyam RamNo ratings yet
- Different Types of DisorderDocument5 pagesDifferent Types of Disordermoonkatana10No ratings yet
- Lesson Plan OBGY PDFDocument12 pagesLesson Plan OBGY PDFKirti kittuNo ratings yet
- HMBDocument41 pagesHMBakmal3501No ratings yet
- ECG Study GuideDocument7 pagesECG Study GuideannaNo ratings yet
- Viral ExanthemDocument18 pagesViral ExanthemRajesh Kumar AsunalaNo ratings yet
- My Research ProposalDocument44 pagesMy Research ProposalMbeng Conrad WamNo ratings yet
- Drug Study On CeftriaxoneDocument7 pagesDrug Study On CeftriaxoneleoNo ratings yet