Download as pptx, pdf, or txt
You might also like
- The Essentials of Psychodynamic PsychotherapyDocument6 pagesThe Essentials of Psychodynamic PsychotherapyMarthaRamirez100% (3)
- Subjective Data:: Assessme NT Diagnos IS Planning Intervention Rationale EvaluationDocument1 pageSubjective Data:: Assessme NT Diagnos IS Planning Intervention Rationale EvaluationCuttie Anne GalangNo ratings yet
- MedSurg Notes - Cancer of The LiverDocument2 pagesMedSurg Notes - Cancer of The LiverMae CeaesarNo ratings yet
- Bullying, Stalking and ExtortionDocument17 pagesBullying, Stalking and ExtortionJLafge83% (6)
- Acute PyelonephritisDocument9 pagesAcute Pyelonephritistaekado-1No ratings yet
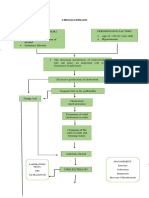
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Acute TonsillopharyngitisDocument17 pagesAcute TonsillopharyngitisRachel Haide NaravalNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Acute Cholecystolithiasis - G4 SB2Document125 pagesAcute Cholecystolithiasis - G4 SB2Jeofy PamaNo ratings yet
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDocument4 pagesNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebNo ratings yet
- Suppositories: Abenol (CAN)Document2 pagesSuppositories: Abenol (CAN)Mikko McDonie VeloriaNo ratings yet
- NSTEMIDocument33 pagesNSTEMIwaazalimahwahidNo ratings yet
- 4th Yr. Med Cardio Module Question - Copy-1Document11 pages4th Yr. Med Cardio Module Question - Copy-1Sheda BondNo ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- Drug Study ColestipolDocument3 pagesDrug Study ColestipolAbby AngNo ratings yet
- Case Study Liver CirrhosisDocument55 pagesCase Study Liver CirrhosisJoseph Emmanuel CandaNo ratings yet
- CHN FinalsDocument15 pagesCHN FinalsLyndon SayongNo ratings yet
- Amoebiasis Case StudyDocument13 pagesAmoebiasis Case StudymelvinpasionaNo ratings yet
- PYOMYOSITISDocument6 pagesPYOMYOSITISChristine CoridoNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument76 pagesChronic Obstructive Pulmonary DiseasedidinNo ratings yet
- Ongoing AppraisalDocument2 pagesOngoing AppraisalLouisa Marie MirandaNo ratings yet
- Cholelithiasis PathophysiologyDocument2 pagesCholelithiasis PathophysiologyShinrin SukehiroNo ratings yet
- Pathophysiology of Urinary Tract ObstructionDocument50 pagesPathophysiology of Urinary Tract ObstructionPryo UtamaNo ratings yet
- Bowel IncontinenceDocument4 pagesBowel IncontinenceprashanthNo ratings yet
- Copd - NCPDocument6 pagesCopd - NCPMonique Sacherow BacherNo ratings yet
- 1 Febrile Seizures DDocument30 pages1 Febrile Seizures DDorjee SengeNo ratings yet
- Case Study - Dengue Fever V - S UtiDocument12 pagesCase Study - Dengue Fever V - S UtiHarlene Joyce ReyNo ratings yet
- MSN CASE STUDY FORMATnew-1Document26 pagesMSN CASE STUDY FORMATnew-1Dinesh BanerjeeNo ratings yet
- Ngo 2bsn1 Ncm109 Prelim NCPDocument7 pagesNgo 2bsn1 Ncm109 Prelim NCPAMIEL SIMON NGONo ratings yet
- Nursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionDocument2 pagesNursing Care Plan: Acute Pain Related To Inflammatory Response Secondary To InfectionTammy De GuzmanNo ratings yet
- PEDIA CASE 3 FinalDocument9 pagesPEDIA CASE 3 FinalXandra BnnNo ratings yet
- Intrapartum Assessment: Jonelle Baloloy, MD MCMC Ob GyneDocument39 pagesIntrapartum Assessment: Jonelle Baloloy, MD MCMC Ob GyneJonelle baloloyNo ratings yet
- Model Nursing Care PlanDocument35 pagesModel Nursing Care PlanAnuchithra RadhakrishnanNo ratings yet
- GE BasavaDocument21 pagesGE BasavaAmalin PrãdhãñNo ratings yet
- Hyperthermia and Risk For AspirationDocument3 pagesHyperthermia and Risk For AspirationAlmyr RimandoNo ratings yet
- Anemia-Careplan For AdultDocument29 pagesAnemia-Careplan For AdultdjbhetaNo ratings yet
- NCP CvaDocument4 pagesNCP CvaMariquita BuenafeNo ratings yet
- Insulin GlargineDocument2 pagesInsulin GlarginePatricia MaglasangNo ratings yet
- Regañon - Rle Case # 1Document22 pagesRegañon - Rle Case # 1Darla Janyll RegañonNo ratings yet
- OtosclerosisDocument36 pagesOtosclerosisShamsheer ShaikNo ratings yet
- Sample Case StudyDocument23 pagesSample Case StudyDELFIN, Kristalyn JaneNo ratings yet
- Nursing Care in MR.X With Urinary Retention: Disusun OlehDocument4 pagesNursing Care in MR.X With Urinary Retention: Disusun OlehHafin WardanaNo ratings yet
- Chronic GastritisDocument7 pagesChronic GastritisDivina AquinoNo ratings yet
- Nursing Care Plan On Platelet DisordersDocument8 pagesNursing Care Plan On Platelet DisordersbhavanaNo ratings yet
- IM AdconDocument28 pagesIM AdconCla SantosNo ratings yet
- Case Scenario 1: Benign Prostatic Hyperplasia: Aldrin M. Paulino BSN 3ADocument4 pagesCase Scenario 1: Benign Prostatic Hyperplasia: Aldrin M. Paulino BSN 3A24 PAULINO ALDRIN MUJARNo ratings yet
- Cu 3 Week 3Document3 pagesCu 3 Week 3Maica LectanaNo ratings yet
- Diabetic Ketoacidosis: Albano, Bautista, Cimatu, Purificacion, SieteralesDocument84 pagesDiabetic Ketoacidosis: Albano, Bautista, Cimatu, Purificacion, SieteralesSyd BautistaNo ratings yet
- Nursing Skills Output (Nso)Document4 pagesNursing Skills Output (Nso)Julius ElciarioNo ratings yet
- Action Plan - Inadequate IncomeDocument2 pagesAction Plan - Inadequate IncomeBenedict James BermasNo ratings yet
- Intussusception: PathophysiologyDocument8 pagesIntussusception: PathophysiologyNaufal AndaluNo ratings yet
- Nursing Physical AssessmentDocument5 pagesNursing Physical AssessmentApril Louise PaluganNo ratings yet
- Case Presentation: Presented byDocument34 pagesCase Presentation: Presented byZahid AnwarNo ratings yet
- CASE PRESentationDocument30 pagesCASE PRESentationllanelli.graciaNo ratings yet
- Family Nursing Care Plan: Group A3 - ObDocument4 pagesFamily Nursing Care Plan: Group A3 - ObErika CadawanNo ratings yet
- BPHDocument81 pagesBPHFlo Neri BerondoNo ratings yet
- Orientation On Community Health - Doh Programs & ServicesDocument11 pagesOrientation On Community Health - Doh Programs & ServicesAudrey Beatrice ReyesNo ratings yet
- Ariane NCP 1Document2 pagesAriane NCP 1Kristian Ray EraulaNo ratings yet
- Acute PyelonephritisDocument105 pagesAcute Pyelonephritisyasira50% (2)
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Heirs of John Sycip vs. CA G.R. No. 76487 November 9 1990Document3 pagesHeirs of John Sycip vs. CA G.R. No. 76487 November 9 1990Mariel D. Portillo100% (1)
- Plyometric Training - Part I by Juan Carlos SantanaDocument2 pagesPlyometric Training - Part I by Juan Carlos SantanaPedro SilvaNo ratings yet
- Mge 4Document17 pagesMge 4RUPAV TIWARINo ratings yet
- Major Landforms of The Earth NotesDocument3 pagesMajor Landforms of The Earth NotesSIMMA SAI PRASANNANo ratings yet
- GWI Hydrothermal 2018 US-final-updated 1125191Document196 pagesGWI Hydrothermal 2018 US-final-updated 1125191Garima BohraNo ratings yet
- Ferdinando Carulli - Op 121, 24 Pieces - 4. Anglaise in A MajorDocument2 pagesFerdinando Carulli - Op 121, 24 Pieces - 4. Anglaise in A MajorOniscoidNo ratings yet
- Assignment in Research 1Document7 pagesAssignment in Research 1cpmac123No ratings yet
- If ملخص قواعدDocument2 pagesIf ملخص قواعدAhmed GaninyNo ratings yet
- Rat ModelDocument1 pageRat Modelapi-483276188No ratings yet
- Artificial Intelligence and Patent LawDocument4 pagesArtificial Intelligence and Patent LawSaksham TyagiNo ratings yet
- The Role of Green InfrastractureDocument18 pagesThe Role of Green InfrastractureYonaminos Taye WassieNo ratings yet
- Dedication Certificate John Clyde D. Cristobal: This Certifies ThatDocument1 pageDedication Certificate John Clyde D. Cristobal: This Certifies ThatAGSAOAY JASON F.No ratings yet
- Present Continuous - Present Simple Vs Present ContinuousDocument2 pagesPresent Continuous - Present Simple Vs Present ContinuouseewuanNo ratings yet
- SocratesDocument10 pagesSocratesarvin paruliNo ratings yet
- Case Study of A Condemned Boiler & Methods To Re-Establish ItDocument43 pagesCase Study of A Condemned Boiler & Methods To Re-Establish Its sivaNo ratings yet
- Imesa Minifluor Copertina - en WebDocument52 pagesImesa Minifluor Copertina - en WebAlaa ZoraNo ratings yet
- Desmand Whitson Resume 1PDFDocument2 pagesDesmand Whitson Resume 1PDFRed RaptureNo ratings yet
- State of The Handloom Industry of BangladeshDocument8 pagesState of The Handloom Industry of BangladeshNoshin NawarNo ratings yet
- Analysis of Old Trends in Indian Wine-Making and Need of Expert System in Wine-MakingDocument10 pagesAnalysis of Old Trends in Indian Wine-Making and Need of Expert System in Wine-MakingIJRASETPublicationsNo ratings yet
- Staffordshire Surge Vs Manchester TitansDocument28 pagesStaffordshire Surge Vs Manchester TitansShaun RogersNo ratings yet
- Accounting For Managers: S. No. Questions 1Document5 pagesAccounting For Managers: S. No. Questions 1shilpa mishraNo ratings yet
- Module 3 Segmentation Targeting Positioning FINAL PDFDocument13 pagesModule 3 Segmentation Targeting Positioning FINAL PDFLusiana Lie100% (1)
- User Manual of CUBOIDDocument50 pagesUser Manual of CUBOIDshahinur rahmanNo ratings yet
- Product Data Sheet Ingenuity Core LRDocument16 pagesProduct Data Sheet Ingenuity Core LRCeoĐứcTrườngNo ratings yet
- Test Method For DDF ProjectDocument13 pagesTest Method For DDF ProjectrantosbNo ratings yet
- 07 - Chapter 3 PDFDocument56 pages07 - Chapter 3 PDFSrikanth GandhamNo ratings yet
- Stones Unit 2bDocument11 pagesStones Unit 2bJamal Al-deenNo ratings yet
- Deed of DonationDocument2 pagesDeed of DonationMary RockwellNo ratings yet