Download as ppt, pdf, or txt
You might also like
- Head Trauma: Yoon Seung-Hwan, M.DDocument53 pagesHead Trauma: Yoon Seung-Hwan, M.DAhmed ZahranNo ratings yet
- Ched Memorandum Order (Cmo) 14 2009Document74 pagesChed Memorandum Order (Cmo) 14 2009Matt Lao Dionela100% (1)
- Fookien PDFDocument4 pagesFookien PDFMatt Lao DionelaNo ratings yet
- Neurologicdisorders 100816033614 Phpapp01 PDFDocument96 pagesNeurologicdisorders 100816033614 Phpapp01 PDFenam professorNo ratings yet
- Paget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesFrom EverandPaget Disease of Bone, A Simple Guide to the Condition, Treatment and Related DiseasesNo ratings yet
- Night Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNight Sweats, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Fracture 01Document42 pagesFracture 01api-19916399No ratings yet
- Stroke Rsu Banjar: DR Fuad Hanif Sps M.KesDocument80 pagesStroke Rsu Banjar: DR Fuad Hanif Sps M.KesRobert HarrisNo ratings yet
- FractureDocument302 pagesFractureMaryjoy Gabriellee De La CruzNo ratings yet
- AmputationDocument36 pagesAmputationaldriansilverNo ratings yet
- Head InjuryDocument11 pagesHead InjurypertinenteNo ratings yet
- Supracondylar FractureDocument53 pagesSupracondylar Fracturedesire kbpNo ratings yet
- STROKEDocument9 pagesSTROKEhillary elsaNo ratings yet
- Colles FractureDocument89 pagesColles Fracturenur syafiqah kamaruzaman100% (1)
- Stroke Syndromes (Etiology & Clinical Features)Document40 pagesStroke Syndromes (Etiology & Clinical Features)nisha_m_patel2006No ratings yet
- Leg UlcerDocument28 pagesLeg UlcerRanindya PutriNo ratings yet
- Acute Flaccid ParalysisDocument4 pagesAcute Flaccid ParalysisZharah RuzNo ratings yet
- Introduction To FracturesDocument40 pagesIntroduction To FracturesAnisah Pangandag MapandiNo ratings yet
- PPTDocument61 pagesPPTRheal P EsmailNo ratings yet
- By: Noor Majeed RehaniDocument23 pagesBy: Noor Majeed RehaniMihaela Toma0% (1)
- Wilson S DiseaseDocument28 pagesWilson S DiseasemichaelcylNo ratings yet
- Sequelae of Trumatic Brain InjuryDocument19 pagesSequelae of Trumatic Brain InjuryAnurag SuryawanshiNo ratings yet
- Cerebrovascular AccidentDocument62 pagesCerebrovascular AccidentJaydee DalayNo ratings yet
- Spinal Cord Injury, DisordersDocument54 pagesSpinal Cord Injury, DisordersChananNo ratings yet
- Cerebrovascular AccidentDocument30 pagesCerebrovascular AccidentJaydee Dalay100% (2)
- Rheumatoid Arthritis Module I ADocument22 pagesRheumatoid Arthritis Module I Apanks.79No ratings yet
- Carpel Tunnel SyndromeDocument12 pagesCarpel Tunnel Syndromeyordin deontaNo ratings yet
- Management of Diabetic FootsDocument12 pagesManagement of Diabetic FootsHabib Bakri Mamat At-TaranjaniNo ratings yet
- Bone Marrow and Stem Cell TranspplantDocument28 pagesBone Marrow and Stem Cell TranspplantVILLEJO JHOVIALENNo ratings yet
- Pre Operative Planning For Total Hip ArthroplastyDocument78 pagesPre Operative Planning For Total Hip ArthroplastyJulio EspinozaNo ratings yet
- Acute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramDocument56 pagesAcute Coronary Syndrome: Rich Derby, LT Col, USAF MGMC Family Practice ProgramprincezastaridaNo ratings yet
- Compartment Syndrome: Sebelas Maret UniversityDocument8 pagesCompartment Syndrome: Sebelas Maret Universitykhrisna satyaksaNo ratings yet
- Motor Neuron DiseaseDocument8 pagesMotor Neuron DiseaseyigoNo ratings yet
- Osteoarthritis: T Person's of Developing Osteoarthritis. It IncludesDocument5 pagesOsteoarthritis: T Person's of Developing Osteoarthritis. It IncludesLove Shery SabrosoNo ratings yet
- Spinal Cord SyndromesDocument42 pagesSpinal Cord SyndromesratnacantikNo ratings yet
- Aetiology, Pathogenesis, and Pathology of Cervical NeoplasiaDocument9 pagesAetiology, Pathogenesis, and Pathology of Cervical NeoplasiaKamilah NasarNo ratings yet
- Orthopedic SlidesDocument78 pagesOrthopedic SlidesAzry Mustapa100% (1)
- DesenteryDocument3 pagesDesenteryAby Gift AnnNo ratings yet
- PeritonitisDocument21 pagesPeritonitisVaibhav Karoliya100% (1)
- Osteomyelitis Metabolic Bone DisordersDocument36 pagesOsteomyelitis Metabolic Bone DisordersVishesh JainNo ratings yet
- Sickle Cell Disease: Click To Edit Master Subtitle StyleDocument13 pagesSickle Cell Disease: Click To Edit Master Subtitle StyleAditya Rangga Fandiarta100% (1)
- Slides 2 - Wounds, UlcersDocument80 pagesSlides 2 - Wounds, UlcersCWT2010No ratings yet
- Managing The Diabetic FootDocument45 pagesManaging The Diabetic FootArio Sabrang100% (1)
- Transient Ischemic Attack: - Time Based Definition: (Old Definition) Harrisons Principle of Medicine 19 EditionDocument14 pagesTransient Ischemic Attack: - Time Based Definition: (Old Definition) Harrisons Principle of Medicine 19 EditionHermie Alexander SiaNo ratings yet
- 13 - Surgical InfectionsDocument26 pages13 - Surgical InfectionsEma KhalilNo ratings yet
- Ayurveda ADocument119 pagesAyurveda AAnish JohnNo ratings yet
- LATHYRISM AND PHOTOSENSiTIZATIONDocument33 pagesLATHYRISM AND PHOTOSENSiTIZATIONSunilNo ratings yet
- N24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis AsthmaDocument42 pagesN24: Class #8 Obstructive and Inflammatory Lung Disease: Emphysema Chronic Bronchitis Asthmadentist40No ratings yet
- Head Injury OkeDocument42 pagesHead Injury OkeAnonymous p9msXAEwNo ratings yet
- Pancreatic Cancer: Pathophysiologic EtiologyDocument2 pagesPancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNo ratings yet
- Myotonic Dystrophy: By: Aakash ReddyDocument12 pagesMyotonic Dystrophy: By: Aakash ReddyAakash ReddyNo ratings yet
- InhalDocument33 pagesInhallupeNo ratings yet
- OMCDocument37 pagesOMCyurie_ameliaNo ratings yet
- Muscle Biopsy and Interpretation: Presenter:Dr Suzeena Sayyed Ali Shakoor. Moderator:Dr AmruthaDocument10 pagesMuscle Biopsy and Interpretation: Presenter:Dr Suzeena Sayyed Ali Shakoor. Moderator:Dr AmruthaSuzeena ShabeebNo ratings yet
- Fractures of The Upper LimbDocument20 pagesFractures of The Upper LimbWendy Francisca Borquez PerezNo ratings yet
- Scapulohumeral PeriarthritisDocument29 pagesScapulohumeral PeriarthritisMárcia PatríciaNo ratings yet
- Tumor OtakDocument17 pagesTumor Otakmona030988No ratings yet
- Understanding Low Blood Pressure - The BasicsDocument6 pagesUnderstanding Low Blood Pressure - The BasicsRajeev Nechiyil100% (1)
- Cerebro Vascular AccidentDocument82 pagesCerebro Vascular AccidentJayvee Novenario Casaljay100% (1)
- Degenerative Disease of CNSDocument50 pagesDegenerative Disease of CNSRadhikaNo ratings yet
- Anal FistulaDocument26 pagesAnal FistulaBeverly PagcaliwaganNo ratings yet
- Synovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandSynovial Chondromatosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Policies, Standards Requirements For Licensing Birthing ClinicDocument46 pagesPolicies, Standards Requirements For Licensing Birthing ClinicMatt Lao Dionela83% (24)
- What To Do List After Passing The NleDocument2 pagesWhat To Do List After Passing The NleMatt Lao Dionela50% (2)
- Relativism, Healthcare and Moral-Cultural IssuesDocument55 pagesRelativism, Healthcare and Moral-Cultural IssuesMatt Lao Dionela83% (6)
- Fundamentals of IV Therapy.22613459Document15 pagesFundamentals of IV Therapy.22613459Matt Lao DionelaNo ratings yet
- Intravenous TherapyDocument22 pagesIntravenous TherapyMatt Lao Dionela100% (1)
- Geriatric Nursing Week2Document45 pagesGeriatric Nursing Week2Matt Lao DionelaNo ratings yet
- Neurocardio NursingDocument101 pagesNeurocardio NursingMatt Lao DionelaNo ratings yet
- Care of Clients With Cardiovascular DisordersDocument67 pagesCare of Clients With Cardiovascular DisordersMatt Lao DionelaNo ratings yet
- Maternal/Ob NotesDocument45 pagesMaternal/Ob NotesJoanne Christina Buenafe100% (1)
- NURSING PRACTICE IV Care of Clients With Physiologic and Psychosocial AlterationsDocument31 pagesNURSING PRACTICE IV Care of Clients With Physiologic and Psychosocial AlterationsMatt Lao Dionela100% (1)
- My Hope Is JesusDocument2 pagesMy Hope Is JesusMatt Lao DionelaNo ratings yet
- Medical Surgical ComprehensiveDocument15 pagesMedical Surgical ComprehensiveMatt Lao DionelaNo ratings yet
- Why Does God Allow People To Suffer?Document6 pagesWhy Does God Allow People To Suffer?Matt Lao DionelaNo ratings yet
- Eas 749 2010 Brown Sugar SpecificationDocument10 pagesEas 749 2010 Brown Sugar SpecificationFelix MwandukaNo ratings yet
- Viewpoint Shaping Resilient SDocument11 pagesViewpoint Shaping Resilient SLM 165No ratings yet
- Blockchain and COVID-19 Pandemic: Applications and ChallengesDocument20 pagesBlockchain and COVID-19 Pandemic: Applications and ChallengesSameerNo ratings yet
- Sambutan Ketupel SeminterDocument1 pageSambutan Ketupel SeminterIt's NovNo ratings yet
- Shampoo BarDocument1 pageShampoo BarrezaNo ratings yet
- ACTIVITY # 2 Pharmacology SubjectDocument3 pagesACTIVITY # 2 Pharmacology SubjectSamantha Grace SuicoNo ratings yet
- Goals and Subgoals of The SurveyDocument18 pagesGoals and Subgoals of The SurveyUrja DhabardeNo ratings yet
- Biological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyDocument34 pagesBiological Approach Dement and Kleitman (Sleep and Dreams) : Ms - Mariam El GabalawyNeda ElewaNo ratings yet
- Luma - Health Insurance Quotation - May Kabyar Oo (3 Options)Document3 pagesLuma - Health Insurance Quotation - May Kabyar Oo (3 Options)Kabyar MayNo ratings yet
- ANSI b301 99pdfDocument20 pagesANSI b301 99pdfstrip1No ratings yet
- TBT-14 Personal Protective Equipments Week-12Document3 pagesTBT-14 Personal Protective Equipments Week-12saad aliNo ratings yet
- Safety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingDocument8 pagesSafety Data Sheet: Section 1: Identification of The Substance/Mixture and of The Company/UndertakingElizabeth Trejo MoralesNo ratings yet
- Mid-Term Test - Writing CreativeDocument3 pagesMid-Term Test - Writing CreativeTazqianisa RohadiNo ratings yet
- Research Paper - Negative Effects of Video Games On ChildrenDocument2 pagesResearch Paper - Negative Effects of Video Games On ChildrenNicole JimelgaNo ratings yet
- 2021 BLS Study GuideDocument2 pages2021 BLS Study GuideShane Brown100% (3)
- Quarterly Test - Q4 English 5Document4 pagesQuarterly Test - Q4 English 5Bem JazzelNo ratings yet
- A Study of Plithogenic Graphs: Applications in Spreading Coronavirus Disease (COVID-19) GloballyDocument21 pagesA Study of Plithogenic Graphs: Applications in Spreading Coronavirus Disease (COVID-19) GloballyScience DirectNo ratings yet
- Vision: WWW - Visionias.inDocument18 pagesVision: WWW - Visionias.inamitNo ratings yet
- MSDS - Mobil DTE 26 UltraDocument10 pagesMSDS - Mobil DTE 26 UltraYosua SimanjuntakNo ratings yet
- Daycare Case ReportDocument45 pagesDaycare Case ReportApril ToweryNo ratings yet
- Medicaid Adult Dental Benefits Overview Appendix - 091519Document6 pagesMedicaid Adult Dental Benefits Overview Appendix - 091519carzhallNo ratings yet
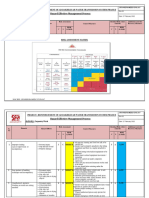
- RISK ASSESSMENT - Carpentry WorkDocument6 pagesRISK ASSESSMENT - Carpentry WorkbalajiNo ratings yet
- Lab Manual - LEVEL 1 - AIR PARTICLES - During MCODocument3 pagesLab Manual - LEVEL 1 - AIR PARTICLES - During MCOAthirah DinataNo ratings yet
- MSDS-Hand Sanitizer - CHIKDocument15 pagesMSDS-Hand Sanitizer - CHIKVarun AggarwalNo ratings yet
- A Definition of CoachingDocument32 pagesA Definition of CoachingSandy KumarNo ratings yet
- Material Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationDocument4 pagesMaterial Safety Data Sheet Hyperplast ES901: 1: Product and Company IdentificationStewart CredoNo ratings yet
- Laboratory Errors in The Fabrication of Complete Dentures. A Clinical SurveyDocument5 pagesLaboratory Errors in The Fabrication of Complete Dentures. A Clinical Surveykhaled allaNo ratings yet
- Respectful Maternity CareDocument33 pagesRespectful Maternity CareJenelle Melinda TullochNo ratings yet
- Philippine Normal University - Center For Teaching and LearningDocument41 pagesPhilippine Normal University - Center For Teaching and LearningFritz Ren KeifferNo ratings yet
- Erythrocyte Sedimentation Rate: Westergren MethodDocument20 pagesErythrocyte Sedimentation Rate: Westergren MethodDenise April June CadizNo ratings yet