
M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research Scholar
M.Prasad Naidu MSC Medical Biochemistry, Ph.D.Research Scholar
You might also like
- Principles of Econometrics 4th Edition Hill Solutions ManualDocument34 pagesPrinciples of Econometrics 4th Edition Hill Solutions Manualcourtneyriceacnmbxqiky100% (13)
- F5ae9484 9454 AgricolaDocument150 pagesF5ae9484 9454 Agricolajvega_534120No ratings yet
- Investigatory ProjectDocument13 pagesInvestigatory Projecte_geanga84% (31)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- For Information Only, Will Not Be Exchanged When Altered!: Spare Parts ListDocument13 pagesFor Information Only, Will Not Be Exchanged When Altered!: Spare Parts Listhorica7167% (3)
- The Gastrointestinal Tract: صقن اهيب ةرضاحملا Cron disease Ulcerative colitis Lipase enzyme Calprotectin ليصافتDocument31 pagesThe Gastrointestinal Tract: صقن اهيب ةرضاحملا Cron disease Ulcerative colitis Lipase enzyme Calprotectin ليصافتامجد حسين جواد كاظمNo ratings yet
- Karaganda Medical University Pathphysiology Submitted By: Uppal Prachi GROUP: 3001 Task 1Document4 pagesKaraganda Medical University Pathphysiology Submitted By: Uppal Prachi GROUP: 3001 Task 1Prachi UppalNo ratings yet
- Malabsorption SyndromeDocument12 pagesMalabsorption Syndromekint manlangitNo ratings yet
- Intestinal Failure and Short Bowel SyndromeDocument5 pagesIntestinal Failure and Short Bowel SyndromesivaNo ratings yet
- Disorders of Intestinal AbsorptionDocument83 pagesDisorders of Intestinal AbsorptionMalika SadridinovaNo ratings yet
- Lactose Intolerance: C2 - Group 3Document29 pagesLactose Intolerance: C2 - Group 3Mark PadulloNo ratings yet
- 14.malabsorption SyndromesDocument5 pages14.malabsorption SyndromesPriyaNo ratings yet
- Evaluation Chronic DiarrheaDocument34 pagesEvaluation Chronic DiarrheaarthoclaseNo ratings yet
- FesesDocument27 pagesFesesNurul Aeni FitriyahNo ratings yet
- Chronic Diarrhoea TreatmentDocument4 pagesChronic Diarrhoea TreatmentRanjith KumarNo ratings yet
- Report DISORDERS OF MALABSORPTIONDocument8 pagesReport DISORDERS OF MALABSORPTIONKathleen Anzhelika B. NemenzoNo ratings yet
- Protocol SBSDocument33 pagesProtocol SBSSteven GodelmanNo ratings yet
- Diarrea Crónica Mar95Document5 pagesDiarrea Crónica Mar95apadronNo ratings yet
- Pud Case StudyDocument6 pagesPud Case Studyapi-302326926100% (1)
- Fecal Fat Test-2020Document4 pagesFecal Fat Test-2020Djdjjd SiisusNo ratings yet
- 1Document55 pages1abcd efgh0% (1)
- Liver Cirrhosis Marking KeyDocument5 pagesLiver Cirrhosis Marking KeyChristone “Zuluzulu” ZuluNo ratings yet
- CC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CDocument45 pagesCC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CMukhtar JamacNo ratings yet
- GI (PBL3) - Mohamad Arbian Karim - FMUI20Document7 pagesGI (PBL3) - Mohamad Arbian Karim - FMUI20Mohamad Arbian KarimNo ratings yet
- Diagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical ExaminationDocument58 pagesDiagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical Examinationsanjay kumarNo ratings yet
- Gastrointestinal FunctionDocument36 pagesGastrointestinal Functionsarkiaeesha20No ratings yet
- Celiac DiseaseDocument15 pagesCeliac DiseaseMarty AsisNo ratings yet
- SX Intestino Corto 2Document6 pagesSX Intestino Corto 2Avof's SamashNo ratings yet
- Malabsorption SyndromeDocument31 pagesMalabsorption SyndromeSahilSharma100% (1)
- Hyperemesis GravidarumDocument4 pagesHyperemesis GravidarumAaliyaan KhanNo ratings yet
- Case 034: ConstipationDocument7 pagesCase 034: ConstipationZauza100% (1)
- Drugs Used in Liver DiseaseDocument17 pagesDrugs Used in Liver Diseaseblast2111No ratings yet
- Lactose Intolerance A2 GRP 3Document60 pagesLactose Intolerance A2 GRP 3Kristian CadaNo ratings yet
- Chronic DiarrheaDocument53 pagesChronic Diarrheahusenbrz4No ratings yet
- Surgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DDocument33 pagesSurgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DLilibeth Tenorio De Leon100% (1)
- en Paralytic Ileus in Vegetarian With PneumDocument6 pagesen Paralytic Ileus in Vegetarian With PneumDanuNo ratings yet
- Nutrition For Patients With Gastrointestinal Disorders Lec 7Document20 pagesNutrition For Patients With Gastrointestinal Disorders Lec 7Youssif Menam100% (1)
- Exercise and Spirulina Control Non-Alcoholic Hepatic Steatosis and Lipid Profile in Diabetic Wistar RatsDocument7 pagesExercise and Spirulina Control Non-Alcoholic Hepatic Steatosis and Lipid Profile in Diabetic Wistar RatslilumomoNo ratings yet
- CC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingDocument36 pagesCC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingSaad KhanNo ratings yet
- Manchester Anaemia GuideDocument13 pagesManchester Anaemia Guidemubzy14No ratings yet
- Anti DiarrhoealsDocument37 pagesAnti DiarrhoealsCrome operatorNo ratings yet
- Major Case StudyDocument26 pagesMajor Case StudyVin Mamuric Meneses100% (1)
- Mep 2 Assesemnt CC NewDocument12 pagesMep 2 Assesemnt CC NewPrecious Bardon-MempinNo ratings yet
- Malabsorption SyndromeDocument1 pageMalabsorption SyndromesamanthaNo ratings yet
- Ikp 4-MavzuDocument13 pagesIkp 4-Mavzubegzodrahmonberdiyev03No ratings yet
- Malabsorption SyndromeDocument24 pagesMalabsorption SyndromeanojanNo ratings yet
- 17 1 DR ElhadariDocument11 pages17 1 DR ElhadariatgyjppsjxbdvtwdvjNo ratings yet
- Ospe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryDocument29 pagesOspe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryManashi JalanNo ratings yet
- Liver CirrhosisDocument8 pagesLiver CirrhosisgoyaNo ratings yet
- Liver Function TestDocument5 pagesLiver Function Testkriss WongNo ratings yet
- Diare 1Document9 pagesDiare 1Altus GoldenNo ratings yet
- HidalgoElishaGay CaseStudyDocument20 pagesHidalgoElishaGay CaseStudyinkpen56789No ratings yet
- Neonatal Cholestasis: Priyanka VishwakarmaDocument38 pagesNeonatal Cholestasis: Priyanka VishwakarmaAlex100% (1)
- Osmotic Diarrhoea: Difficile)Document4 pagesOsmotic Diarrhoea: Difficile)Marwan M.No ratings yet
- Lactose Intolerance Final PresentationDocument63 pagesLactose Intolerance Final PresentationCarl Angelo SuaybaguioNo ratings yet
- Age-J AnDocument5 pagesAge-J AnEnna NiromaNo ratings yet
- Sas 4Document2 pagesSas 4Charlene LagradillaNo ratings yet
- Chronic Diarrhoea and MalabsorptionDocument25 pagesChronic Diarrhoea and MalabsorptionadelekeyusufNo ratings yet
- Bence JonesDocument5 pagesBence JonesChristian Eduard de Dios100% (1)
- Total Parenteral NutritionDocument9 pagesTotal Parenteral NutritionLilian YmbongNo ratings yet
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Dietary Dialysis With Acacia Gum: Intestinal Dialysis TechnologyDocument8 pagesDietary Dialysis With Acacia Gum: Intestinal Dialysis TechnologyAamir Jalal Al-MosawiNo ratings yet
- Neonatal JaundiceDocument77 pagesNeonatal Jaundiceodhiambovictor2424No ratings yet
- Endocrine: (Type 2 Diabetes Mellitus) : A1C TestDocument8 pagesEndocrine: (Type 2 Diabetes Mellitus) : A1C TestAce FabrigasNo ratings yet
- Translation: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument33 pagesTranslation: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Non-Parametric Tests: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument15 pagesNon-Parametric Tests: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Vitamin-A: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument42 pagesVitamin-A: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Thyroid HormonesDocument63 pagesThyroid HormonesDr. M. Prasad NaiduNo ratings yet
- Water Soluble VitaminsDocument55 pagesWater Soluble VitaminsDr. M. Prasad Naidu100% (1)
- Urea CycleDocument8 pagesUrea CycleDr. M. Prasad Naidu100% (1)
- STUDENT T-TestDocument20 pagesSTUDENT T-TestDr. M. Prasad NaiduNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument23 pagesM.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Signal TransductionDocument77 pagesSignal TransductionM.PRASAD NAIDUNo ratings yet
- Transcription: M.Prasad Naidu MSC Medical Biochemisty, Ph.D.Research ScholarDocument33 pagesTranscription: M.Prasad Naidu MSC Medical Biochemisty, Ph.D.Research ScholarDr. M. Prasad NaiduNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument17 pagesM.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Thin Layer ChromatographyDocument16 pagesThin Layer ChromatographyDr. M. Prasad Naidu100% (1)
- Serum Protein Electrophoresis & Their Clinical ImportanceDocument44 pagesSerum Protein Electrophoresis & Their Clinical ImportanceDr. M. Prasad NaiduNo ratings yet
- Sequence DatabaseDocument36 pagesSequence DatabaseDr. M. Prasad NaiduNo ratings yet
- TGF-β Signalling From CellDocument14 pagesTGF-β Signalling From CellDr. M. Prasad NaiduNo ratings yet
- Serum Ferritin and Diabetes Mellitus Type LLDocument21 pagesSerum Ferritin and Diabetes Mellitus Type LLM.PRASAD NAIDUNo ratings yet
- Sex HormonesDocument10 pagesSex HormonesM.PRASAD NAIDUNo ratings yet
- Rna Processing: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument33 pagesRna Processing: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Peptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument30 pagesPeptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Recombinant DNA TechnologyDocument34 pagesRecombinant DNA TechnologyDr. M. Prasad NaiduNo ratings yet
- Renal CalculiDocument49 pagesRenal CalculiDr. M. Prasad NaiduNo ratings yet
- Protein Synthesis: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument12 pagesProtein Synthesis: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Shell RLA Step 4Document2 pagesShell RLA Step 4jonbilbaoNo ratings yet
- Demo LPDocument16 pagesDemo LPAbi RocesNo ratings yet
- Central Board of School EducationDocument11 pagesCentral Board of School EducationADITYA SHARMANo ratings yet
- Spentwash ProcessDocument251 pagesSpentwash ProcessSouvik Pal100% (2)
- Technical Issues Related To New Transmission Lines in Denmark PDFDocument132 pagesTechnical Issues Related To New Transmission Lines in Denmark PDFAndré Luiz0% (1)
- Yaskawa Academy 2016 EDocument56 pagesYaskawa Academy 2016 Ejmorenoh103100% (1)
- MSL Clutch & P P 1-2-13Document3 pagesMSL Clutch & P P 1-2-13Abhishek SinghNo ratings yet
- Flame Tests and Atomic SpectraDocument3 pagesFlame Tests and Atomic SpectraImmanuel LashleyNo ratings yet
- HVAC FundamentalDocument192 pagesHVAC FundamentalMyo Kyaw Kyaw100% (1)
- III Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationDocument18 pagesIII Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationJoathan LessaNo ratings yet
- Pathways To E-Mobility Transition in UgandaDocument10 pagesPathways To E-Mobility Transition in UgandaWamboga OkothNo ratings yet
- Lapping Length of Reinforcement Steel BarsDocument1 pageLapping Length of Reinforcement Steel BarsRambabuNo ratings yet
- m07500838 XXXXXXXX 0enDocument244 pagesm07500838 XXXXXXXX 0enHiệp Phan VănNo ratings yet
- Manual Proportional Directional Control Valve (With Pressure Compensation, Multiple Valve Series)Document6 pagesManual Proportional Directional Control Valve (With Pressure Compensation, Multiple Valve Series)Fawzi AlzubairyNo ratings yet
- Manuale Tecnico-Iconadeco EngDocument28 pagesManuale Tecnico-Iconadeco EngjoaoNo ratings yet
- Work Tool Attachments: Product LineDocument24 pagesWork Tool Attachments: Product LineSzilárd SNo ratings yet
- WS01 Slopes Samantha SarahDocument7 pagesWS01 Slopes Samantha SarahSAMANTHA SARAH PURBANo ratings yet
- The Three Types of Rocks!: Learning ObjectivesDocument2 pagesThe Three Types of Rocks!: Learning ObjectivesJekim Novo LumbaNo ratings yet
- 17 C ENGG NR-1 FATEHGARH-III EQP 400kV ISO STRDocument1 page17 C ENGG NR-1 FATEHGARH-III EQP 400kV ISO STRsarat mishraNo ratings yet
- RidleyWorks15 02Document112 pagesRidleyWorks15 02Sergio Omar OrlandoNo ratings yet
- Perfect Polymers - Product-Introduction - SUNPAL Multiwall Cell) Polycarbonate Standing-Seam Architectural SystemDocument28 pagesPerfect Polymers - Product-Introduction - SUNPAL Multiwall Cell) Polycarbonate Standing-Seam Architectural SystemGirish DhawanNo ratings yet
- Alp 11Document14 pagesAlp 11Alexandra CarhuanchoNo ratings yet
- Optyma™ Slim Pack Just Mount, Connect Piping and Plug: CatalogueDocument36 pagesOptyma™ Slim Pack Just Mount, Connect Piping and Plug: CatalogueCarlos MarroNo ratings yet
- ASAL Economics Workbook AnswersDocument111 pagesASAL Economics Workbook AnswersMatej Milosavljevic100% (1)
- Dec Hanu Tht2 Writing Week 4 - Effect ParagraphDocument11 pagesDec Hanu Tht2 Writing Week 4 - Effect ParagraphHồng BắcNo ratings yet
- Chapter 4Document10 pagesChapter 4Htet_Aung_HlaingNo ratings yet













































































































M.
Prasad Naidu
MSc Medical Biochemistry,
Ph.D.Research Scholar
DEFINITION
The term malabsorption denotes disorders in which
there is a disruption of digestion and nutrients
absorption.
Impairment can be of single or multiple depending on
the abnormality.
This may lead to malnutrition and a variety of
anaemias.
PATHOPHYSIOLOGY :
Digestion is by enzymatic hydrolysis which is initiated by
intraluminal processes requiring gastric,pancreatic, and
biliary secretions.
The final products of digestion are absorbed through the
intestinal epithelial cells.
Malabsorption constitutes the pathological interference with
the normal physiological sequence of digestion (intraluminal
process), absorption (mucosal process) and transport
(postmucosal events) of nutrients.
CLASSIFICATION
CLINICAL FEATURES
Diarrheoa, often steatorrhoea is the most common feature.
Watery,diurnal and nocturnal,bulky,frequent stools are the
clinical hallmark of overt malabsorption.
It is due to impaired water, electrolyte absorption or
irritation from unabsorbed fatty acid.
Bloating, flatulence and abdominal discomfort also seen.
Cramping pain suggests obstructive intestinal segment
especially if it persist after defecation. Eg; Crohns disease.
Weight loss can be significant despite increased oral intake
of nutrients.
Growth retardation,failure to thrive,delayed puberty are seen
in children.
Swelling or oedema are seen due to loss of protein.
Anaemias, commonly from vitamin B
12
, folic acid and iron
deficiency presenting as fatigue and weakness.
Muscle cramp from decreased vitamin D, calcium absorption
and they lead to osteomalacia and osteoporosis.
Bleeding tendencies are seen from vitamin K and other
coagulation factor deficiencies.
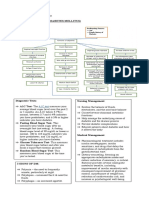
DIAGNOSIS:
As a baseline,the estimation of full blood
count,ESR,haematinics in the form of folate,B
12
and
iron status and serum albumin with serum
calcium,phosphate and magnesium have to be done.
TESTS FOR FAT MALABSORPTION:
The following methods are available .
1.TOTAL FECAL FAT ESTIMATION:
Before the test, the patient is put on a high fat diet,
consuming between 50-150 g/day of fat for three days.
The patient must collect their feces over the next 72
hours using a 1-gallon paint that can be well sealed.
The fecal sample must be refrigerated to prevent any
bacterial action.
Fecal fat analysis is performed by first weighing the sample
and then extracting the lipids with an organic solvent.
The extraction solvent is evaporated and the dry weight of
the fat that remains is measured.
Normal absorption of fat is indicated by a fecal fat level of
less than or equal to 7 grams per day.
2.FAT SCREENING:
A more simple but less accurate way to measure fat
absorption is to count the fat droplets in a well mixed
sample of the stool specimen using a microscope and a
neutral fat stain.
Another simplified screening test is the fat tolerance
test called the butterfat or the fatty meal test.
In this test,the patient is asked to fast overnight and is
given 1 gram of fat per kg of body weight.
Blood is drawn before the dose and again three and six
hours afterwards.
The fasting, three-hour and six-hour plasma samples
are analyzed for triglyceride concentration.
Normal absorption is indicated by at least a 50%
increase in triglycerides over the fasting level.
The 14C-triolein breath test can be useful to
make a diagnosis of steatorrhoea in patients
with difficult diarrhoea.
It has also been used to monitor pancreatic fat
malabsorption
TESTS FOR PANCREATIC MALABSORPTION
Non-invasive pancreatic function tests include
1.The pancreolauryl tests:
It requires the avoidance of Vitamin B and some drugs, and
two consecutive day 10 hour urine collections.
2.The PABA test:
It should be reported as a urinary PABA excretion index by
coadministration of p-aminosalicyclic acid or 14C-PABA.
Both these tests were acceptable as screening tests for
pancreatic exocrine insufficiency.
The invasive tests like secretin-cholecystokinin test and the
Lundh test are in research.
DISACCHARIDASE MALABSORPTION
The measurement of disaccharidases, usually lactase,
maltase and sucrase, is of limited use because of high
coefficients of Variation.
They have a role in diagnosing lactase deficiency and
limited use for monitoring disaccharidase deficiencies
in coeliac disease.
HYDROGEN BREATH TEST
The hydrogen breath test is used to measure two things,
carbohydrate malabsorption such as lactose intolerance
and bacterial overgrowth.
Hydrogen is produced by bacterial fermentation of
unabsorbed carbohydrates in the intestines.
The hydrogen produced goes into the blood stream and is
excreted through the lungs.
The test is done using a gas chromatograph, an apparatus
that can separate compounds from one another based on
their chemical composition.
The patient is asked to fast overnight, and his or her
breath is collected in a plastic syringe at the start of the
test.
The patient is then given something to eat depending
on what is being evaluated.
The patient's breath will be collected in a plastic
syringe every thirty minutes for the next two to five
hours, depending on the test.
The syringe will be capped and sent to the laboratory
for analysis.
The test is simple, non-invasive and not diagnostic, it
gives the doctor an idea of what may be wrong.
PROTEIN LOOSING ENTEROPATHY
Chromium radiolabelled albumin or alpha-1 antitrypsin
excretion are the definitive tests.
BILE ACID MALABSORPTION:
The SeHCAT test with a seven day retention is useful but, if
unavailable, a simple assessment of the clinical response of
diarrhoea to cholestyramine 4-8gms t.d.s. can be used.
TESTS FOR CELIAC DISEASE
Tests for this disease involve drawing the patient's blood and
testing for the presence of three antibodies, antigliadin,
antiendomysium, and antireticulin antibodies.
D-XYLOSE ABSORPTION TEST
D-xylose is a pentose sugar that is not normally found in the
blood.
It can be easily absorbed by healthy intestinal cells without
the aid of pancreatic enzymes, and is poorly metabolized so
that at least 50% of the dose is excreted in the urine within 24
hours.
This test is a good general screen for malfunction of
absorption, and helps to differentiate intestinal
malabsorption syndromes (reduced Dxylose absorption)
from pancreatitis (normal D-xylose absorption).
Adults are given an oral dose usually 25 grams of D-
xylose.
A five-hour timed urine sample is collected, and a
blood sample is collected two hours after the dose is
given.
Children are given a 5 gram dose of Dxylose, and a
blood sample is collected one hour after the dose is
given.
Adults should excrete at least 25% of the dose in the
five-hour urine sample, and have a two-hour blood
level of at least 25 mg/dL.
Children should have a one-hour blood level of at least
20 mg/dL.
The D-xylose test will be normal if the patient has
normal absorptive capacity in the intestine, or if the
patient has malabsorption that is caused by a
pancreatic problem.
It will be low if the patient has celiac disease, tropical
sprue, Crohn's disease, advanced AIDs, or pellegra
(niacin deficiency).
TESTS FOR VITAMIN B12 DEFICIENCY
It is measured by Schilling test.it has 4 stages.
Stage 1: oral vitamin B
12
plus intramuscular
vitamin B
12
In the first part of the test, the patient is
given radiolabeled vitamin B
12
to drink or eat.
An intramuscular injection of unlabeled vitamin B
12
is
given at or around the same time.
.
The purpose of the single injection is to temporarily saturate
B
12
receptors in the liver with enough normal vitamin B
12
to
prevent radioactive vitamin B
12
binding in body tissues
(especially in the liver), so that if absorbed from the G.I.
tract, it will pass into the urine.
The patient's urine is then collected over the next 24 hours to
assess the absorption.
In patients with pernicious anemia or with deficiency due to
impaired absorption, less than 5% of the radiolabeled
vitamin B
12
is detected.
Stage 2: vitamin B
12
and intrinsic factor
If an abnormality is found, the test is repeated, this
time with additional oral intrinsic factor.
If this second urine collection is normal, this shows a
lack of intrinsic factor production, or pernicious
anemia.
Stage 3: vitamin B
12
and antibiotics
This stage is useful for identifying patients with
bacterial overgrowth syndrome.
Stage 4: vitamin B
12
and pancreatic enzymes
This stage, in which pancreatic enzymes are
administered, can be useful in identifying patients
with pancreatitis.
BIOPSY OF SMALL INTESTINAL MUCOSA:
It is useful to confirm the diagnosis.
MALABSORPTION TREATMENT
Management includes
(1) the correction of nutritional deficiencies, and
(2) when possible, the treatment of causative diseases.
Nutritional support
Supplementing various minerals, such as calcium, magnesium, iron,
and vitamins, which may be deficient in malabsorption, is important.
Caloric and protein replacement also is essential.
Medium-chain triglycerides can be used as fat substitutes because
they do not require micelle formation for absorption and their route
of transport is portal rather than lymphatic.
In severe intestinal disease, such as massive resection and extensive
regional enteritis, parenteral nutrition may become necessary.
Treatment of causative diseases
A gluten-free diet helps treat celiac disease.
Similarly, a lactose-free diet helps correct lactose intolerance;
supplementing the first bite of milk-containing food products
with Lactaid also helps.
Protease and lipase supplements are the therapy for pancreatic
insufficiency.
Antibiotics are the therapy for bacterial overgrowth.
Corticosteroids, anti-inflammatory agents, such as
mesalamine, and other therapies are used to treat regional
enteritis.
You might also like
- Principles of Econometrics 4th Edition Hill Solutions ManualDocument34 pagesPrinciples of Econometrics 4th Edition Hill Solutions Manualcourtneyriceacnmbxqiky100% (13)
- F5ae9484 9454 AgricolaDocument150 pagesF5ae9484 9454 Agricolajvega_534120No ratings yet
- Investigatory ProjectDocument13 pagesInvestigatory Projecte_geanga84% (31)
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (3)
- For Information Only, Will Not Be Exchanged When Altered!: Spare Parts ListDocument13 pagesFor Information Only, Will Not Be Exchanged When Altered!: Spare Parts Listhorica7167% (3)
- The Gastrointestinal Tract: صقن اهيب ةرضاحملا Cron disease Ulcerative colitis Lipase enzyme Calprotectin ليصافتDocument31 pagesThe Gastrointestinal Tract: صقن اهيب ةرضاحملا Cron disease Ulcerative colitis Lipase enzyme Calprotectin ليصافتامجد حسين جواد كاظمNo ratings yet
- Karaganda Medical University Pathphysiology Submitted By: Uppal Prachi GROUP: 3001 Task 1Document4 pagesKaraganda Medical University Pathphysiology Submitted By: Uppal Prachi GROUP: 3001 Task 1Prachi UppalNo ratings yet
- Malabsorption SyndromeDocument12 pagesMalabsorption Syndromekint manlangitNo ratings yet
- Intestinal Failure and Short Bowel SyndromeDocument5 pagesIntestinal Failure and Short Bowel SyndromesivaNo ratings yet
- Disorders of Intestinal AbsorptionDocument83 pagesDisorders of Intestinal AbsorptionMalika SadridinovaNo ratings yet
- Lactose Intolerance: C2 - Group 3Document29 pagesLactose Intolerance: C2 - Group 3Mark PadulloNo ratings yet
- 14.malabsorption SyndromesDocument5 pages14.malabsorption SyndromesPriyaNo ratings yet
- Evaluation Chronic DiarrheaDocument34 pagesEvaluation Chronic DiarrheaarthoclaseNo ratings yet
- FesesDocument27 pagesFesesNurul Aeni FitriyahNo ratings yet
- Chronic Diarrhoea TreatmentDocument4 pagesChronic Diarrhoea TreatmentRanjith KumarNo ratings yet
- Report DISORDERS OF MALABSORPTIONDocument8 pagesReport DISORDERS OF MALABSORPTIONKathleen Anzhelika B. NemenzoNo ratings yet
- Protocol SBSDocument33 pagesProtocol SBSSteven GodelmanNo ratings yet
- Diarrea Crónica Mar95Document5 pagesDiarrea Crónica Mar95apadronNo ratings yet
- Pud Case StudyDocument6 pagesPud Case Studyapi-302326926100% (1)
- Fecal Fat Test-2020Document4 pagesFecal Fat Test-2020Djdjjd SiisusNo ratings yet
- 1Document55 pages1abcd efgh0% (1)
- Liver Cirrhosis Marking KeyDocument5 pagesLiver Cirrhosis Marking KeyChristone “Zuluzulu” ZuluNo ratings yet
- CC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CDocument45 pagesCC CC C C C!"#C $!$%: C$!$C c!"7 ":"!CMukhtar JamacNo ratings yet
- GI (PBL3) - Mohamad Arbian Karim - FMUI20Document7 pagesGI (PBL3) - Mohamad Arbian Karim - FMUI20Mohamad Arbian KarimNo ratings yet
- Diagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical ExaminationDocument58 pagesDiagnostic Approach To Malabsorbtion: Suspecting Presence of Malabsorption-History, Physical Examinationsanjay kumarNo ratings yet
- Gastrointestinal FunctionDocument36 pagesGastrointestinal Functionsarkiaeesha20No ratings yet
- Celiac DiseaseDocument15 pagesCeliac DiseaseMarty AsisNo ratings yet
- SX Intestino Corto 2Document6 pagesSX Intestino Corto 2Avof's SamashNo ratings yet
- Malabsorption SyndromeDocument31 pagesMalabsorption SyndromeSahilSharma100% (1)
- Hyperemesis GravidarumDocument4 pagesHyperemesis GravidarumAaliyaan KhanNo ratings yet
- Case 034: ConstipationDocument7 pagesCase 034: ConstipationZauza100% (1)
- Drugs Used in Liver DiseaseDocument17 pagesDrugs Used in Liver Diseaseblast2111No ratings yet
- Lactose Intolerance A2 GRP 3Document60 pagesLactose Intolerance A2 GRP 3Kristian CadaNo ratings yet
- Chronic DiarrheaDocument53 pagesChronic Diarrheahusenbrz4No ratings yet
- Surgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DDocument33 pagesSurgical Nutritions: Prepared By: Lilibeth C.Tenorio, M.DLilibeth Tenorio De Leon100% (1)
- en Paralytic Ileus in Vegetarian With PneumDocument6 pagesen Paralytic Ileus in Vegetarian With PneumDanuNo ratings yet
- Nutrition For Patients With Gastrointestinal Disorders Lec 7Document20 pagesNutrition For Patients With Gastrointestinal Disorders Lec 7Youssif Menam100% (1)
- Exercise and Spirulina Control Non-Alcoholic Hepatic Steatosis and Lipid Profile in Diabetic Wistar RatsDocument7 pagesExercise and Spirulina Control Non-Alcoholic Hepatic Steatosis and Lipid Profile in Diabetic Wistar RatslilumomoNo ratings yet
- CC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingDocument36 pagesCC2E D Ananasovski - Pre-Analytical Factors in Glucose TestingSaad KhanNo ratings yet
- Manchester Anaemia GuideDocument13 pagesManchester Anaemia Guidemubzy14No ratings yet
- Anti DiarrhoealsDocument37 pagesAnti DiarrhoealsCrome operatorNo ratings yet
- Major Case StudyDocument26 pagesMajor Case StudyVin Mamuric Meneses100% (1)
- Mep 2 Assesemnt CC NewDocument12 pagesMep 2 Assesemnt CC NewPrecious Bardon-MempinNo ratings yet
- Malabsorption SyndromeDocument1 pageMalabsorption SyndromesamanthaNo ratings yet
- Ikp 4-MavzuDocument13 pagesIkp 4-Mavzubegzodrahmonberdiyev03No ratings yet
- Malabsorption SyndromeDocument24 pagesMalabsorption SyndromeanojanNo ratings yet
- 17 1 DR ElhadariDocument11 pages17 1 DR ElhadariatgyjppsjxbdvtwdvjNo ratings yet
- Ospe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryDocument29 pagesOspe Case Discussion: Presenter - Dr. Salma Ahmed Dept. of BiochemistryManashi JalanNo ratings yet
- Liver CirrhosisDocument8 pagesLiver CirrhosisgoyaNo ratings yet
- Liver Function TestDocument5 pagesLiver Function Testkriss WongNo ratings yet
- Diare 1Document9 pagesDiare 1Altus GoldenNo ratings yet
- HidalgoElishaGay CaseStudyDocument20 pagesHidalgoElishaGay CaseStudyinkpen56789No ratings yet
- Neonatal Cholestasis: Priyanka VishwakarmaDocument38 pagesNeonatal Cholestasis: Priyanka VishwakarmaAlex100% (1)
- Osmotic Diarrhoea: Difficile)Document4 pagesOsmotic Diarrhoea: Difficile)Marwan M.No ratings yet
- Lactose Intolerance Final PresentationDocument63 pagesLactose Intolerance Final PresentationCarl Angelo SuaybaguioNo ratings yet
- Age-J AnDocument5 pagesAge-J AnEnna NiromaNo ratings yet
- Sas 4Document2 pagesSas 4Charlene LagradillaNo ratings yet
- Chronic Diarrhoea and MalabsorptionDocument25 pagesChronic Diarrhoea and MalabsorptionadelekeyusufNo ratings yet
- Bence JonesDocument5 pagesBence JonesChristian Eduard de Dios100% (1)
- Total Parenteral NutritionDocument9 pagesTotal Parenteral NutritionLilian YmbongNo ratings yet
- Keto LogDocument7 pagesKeto LogKim Justin InfantadoNo ratings yet
- Dietary Dialysis With Acacia Gum: Intestinal Dialysis TechnologyDocument8 pagesDietary Dialysis With Acacia Gum: Intestinal Dialysis TechnologyAamir Jalal Al-MosawiNo ratings yet
- Neonatal JaundiceDocument77 pagesNeonatal Jaundiceodhiambovictor2424No ratings yet
- Endocrine: (Type 2 Diabetes Mellitus) : A1C TestDocument8 pagesEndocrine: (Type 2 Diabetes Mellitus) : A1C TestAce FabrigasNo ratings yet
- Translation: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument33 pagesTranslation: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Non-Parametric Tests: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument15 pagesNon-Parametric Tests: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Vitamin-A: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument42 pagesVitamin-A: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Thyroid HormonesDocument63 pagesThyroid HormonesDr. M. Prasad NaiduNo ratings yet
- Water Soluble VitaminsDocument55 pagesWater Soluble VitaminsDr. M. Prasad Naidu100% (1)
- Urea CycleDocument8 pagesUrea CycleDr. M. Prasad Naidu100% (1)
- STUDENT T-TestDocument20 pagesSTUDENT T-TestDr. M. Prasad NaiduNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument23 pagesM.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Signal TransductionDocument77 pagesSignal TransductionM.PRASAD NAIDUNo ratings yet
- Transcription: M.Prasad Naidu MSC Medical Biochemisty, Ph.D.Research ScholarDocument33 pagesTranscription: M.Prasad Naidu MSC Medical Biochemisty, Ph.D.Research ScholarDr. M. Prasad NaiduNo ratings yet
- M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument17 pagesM.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Thin Layer ChromatographyDocument16 pagesThin Layer ChromatographyDr. M. Prasad Naidu100% (1)
- Serum Protein Electrophoresis & Their Clinical ImportanceDocument44 pagesSerum Protein Electrophoresis & Their Clinical ImportanceDr. M. Prasad NaiduNo ratings yet
- Sequence DatabaseDocument36 pagesSequence DatabaseDr. M. Prasad NaiduNo ratings yet
- TGF-β Signalling From CellDocument14 pagesTGF-β Signalling From CellDr. M. Prasad NaiduNo ratings yet
- Serum Ferritin and Diabetes Mellitus Type LLDocument21 pagesSerum Ferritin and Diabetes Mellitus Type LLM.PRASAD NAIDUNo ratings yet
- Sex HormonesDocument10 pagesSex HormonesM.PRASAD NAIDUNo ratings yet
- Rna Processing: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument33 pagesRna Processing: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Peptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument30 pagesPeptides and Proteins: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Recombinant DNA TechnologyDocument34 pagesRecombinant DNA TechnologyDr. M. Prasad NaiduNo ratings yet
- Renal CalculiDocument49 pagesRenal CalculiDr. M. Prasad NaiduNo ratings yet
- Protein Synthesis: M.Prasad Naidu MSC Medical Biochemistry, PH.DDocument12 pagesProtein Synthesis: M.Prasad Naidu MSC Medical Biochemistry, PH.DDr. M. Prasad NaiduNo ratings yet
- Shell RLA Step 4Document2 pagesShell RLA Step 4jonbilbaoNo ratings yet
- Demo LPDocument16 pagesDemo LPAbi RocesNo ratings yet
- Central Board of School EducationDocument11 pagesCentral Board of School EducationADITYA SHARMANo ratings yet
- Spentwash ProcessDocument251 pagesSpentwash ProcessSouvik Pal100% (2)
- Technical Issues Related To New Transmission Lines in Denmark PDFDocument132 pagesTechnical Issues Related To New Transmission Lines in Denmark PDFAndré Luiz0% (1)
- Yaskawa Academy 2016 EDocument56 pagesYaskawa Academy 2016 Ejmorenoh103100% (1)
- MSL Clutch & P P 1-2-13Document3 pagesMSL Clutch & P P 1-2-13Abhishek SinghNo ratings yet
- Flame Tests and Atomic SpectraDocument3 pagesFlame Tests and Atomic SpectraImmanuel LashleyNo ratings yet
- HVAC FundamentalDocument192 pagesHVAC FundamentalMyo Kyaw Kyaw100% (1)
- III Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationDocument18 pagesIII Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationJoathan LessaNo ratings yet
- Pathways To E-Mobility Transition in UgandaDocument10 pagesPathways To E-Mobility Transition in UgandaWamboga OkothNo ratings yet
- Lapping Length of Reinforcement Steel BarsDocument1 pageLapping Length of Reinforcement Steel BarsRambabuNo ratings yet
- m07500838 XXXXXXXX 0enDocument244 pagesm07500838 XXXXXXXX 0enHiệp Phan VănNo ratings yet
- Manual Proportional Directional Control Valve (With Pressure Compensation, Multiple Valve Series)Document6 pagesManual Proportional Directional Control Valve (With Pressure Compensation, Multiple Valve Series)Fawzi AlzubairyNo ratings yet
- Manuale Tecnico-Iconadeco EngDocument28 pagesManuale Tecnico-Iconadeco EngjoaoNo ratings yet
- Work Tool Attachments: Product LineDocument24 pagesWork Tool Attachments: Product LineSzilárd SNo ratings yet
- WS01 Slopes Samantha SarahDocument7 pagesWS01 Slopes Samantha SarahSAMANTHA SARAH PURBANo ratings yet
- The Three Types of Rocks!: Learning ObjectivesDocument2 pagesThe Three Types of Rocks!: Learning ObjectivesJekim Novo LumbaNo ratings yet
- 17 C ENGG NR-1 FATEHGARH-III EQP 400kV ISO STRDocument1 page17 C ENGG NR-1 FATEHGARH-III EQP 400kV ISO STRsarat mishraNo ratings yet
- RidleyWorks15 02Document112 pagesRidleyWorks15 02Sergio Omar OrlandoNo ratings yet
- Perfect Polymers - Product-Introduction - SUNPAL Multiwall Cell) Polycarbonate Standing-Seam Architectural SystemDocument28 pagesPerfect Polymers - Product-Introduction - SUNPAL Multiwall Cell) Polycarbonate Standing-Seam Architectural SystemGirish DhawanNo ratings yet
- Alp 11Document14 pagesAlp 11Alexandra CarhuanchoNo ratings yet
- Optyma™ Slim Pack Just Mount, Connect Piping and Plug: CatalogueDocument36 pagesOptyma™ Slim Pack Just Mount, Connect Piping and Plug: CatalogueCarlos MarroNo ratings yet
- ASAL Economics Workbook AnswersDocument111 pagesASAL Economics Workbook AnswersMatej Milosavljevic100% (1)
- Dec Hanu Tht2 Writing Week 4 - Effect ParagraphDocument11 pagesDec Hanu Tht2 Writing Week 4 - Effect ParagraphHồng BắcNo ratings yet
- Chapter 4Document10 pagesChapter 4Htet_Aung_HlaingNo ratings yet