Download as ppt, pdf, or txt
You might also like
- INTERACT Nursing Home To Hospital Transfer FormDocument2 pagesINTERACT Nursing Home To Hospital Transfer FormAgnieszka WaligóraNo ratings yet
- Ascariasis & GiardiasisDocument34 pagesAscariasis & GiardiasisMuhammad ShahzadNo ratings yet
- Growth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsDocument49 pagesGrowth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsfateeeNo ratings yet
- Tropical Medicine-1Document355 pagesTropical Medicine-1Fabb NelsonNo ratings yet
- AscarisDocument21 pagesAscarisdipanb625No ratings yet
- Growth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsDocument50 pagesGrowth and Development Failure (Failure To Thrive) Due To Parasitic InfectionsArianti Miranti Lestari FajrinNo ratings yet
- HOOKWORMDocument30 pagesHOOKWORMALBINUS AmbroseNo ratings yet
- Report On AmoebiasisDocument36 pagesReport On Amoebiasisrhimineecat71No ratings yet
- Liver FluksDocument28 pagesLiver Flukszaid nabeelNo ratings yet
- Clinical Manifestation of AscariasisDocument28 pagesClinical Manifestation of AscariasisAishah Shalimar PutriNo ratings yet
- Viral Gastroenteritis: Submitted byDocument20 pagesViral Gastroenteritis: Submitted byRavi PrakashNo ratings yet
- DudeDocument38 pagesDudeGustavo VasquezNo ratings yet
- AphasmidsDocument60 pagesAphasmidsRitz CelsoNo ratings yet
- Nematodes 10-11Document128 pagesNematodes 10-11microperadeniya83% (6)
- 2 NematodesDocument163 pages2 NematodesSammy MirandaNo ratings yet
- Acute If 4 Weeks in DurationDocument9 pagesAcute If 4 Weeks in DurationSalsabila Rahma FadlillahNo ratings yet
- Gastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsDocument77 pagesGastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsSindhu BabuNo ratings yet
- E VermicularisDocument18 pagesE VermicularisYashoda AmarasekeraNo ratings yet
- Junior Intern Review - Oral Revalida 2016Document170 pagesJunior Intern Review - Oral Revalida 2016Cyrus ZalameaNo ratings yet
- 12 - NematodaDocument44 pages12 - NematodaAnnisya MaharaniNo ratings yet
- Nematodes: Prepared By: Charriz A. AmoyanDocument81 pagesNematodes: Prepared By: Charriz A. AmoyanAudrie Allyson GabalesNo ratings yet
- AscariasisDocument50 pagesAscariasisAnaleah MalayaoNo ratings yet
- AscarisDocument18 pagesAscarisHabib UllahNo ratings yet
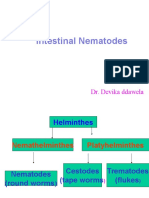
- Intestinal Nematodes: Dr. Devika DdawelaDocument127 pagesIntestinal Nematodes: Dr. Devika DdawelaPraveenKumarNo ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesRosi Gustina100% (8)
- Amebiasis, Giradiasis, Helminths: DR Asim ShresthaDocument49 pagesAmebiasis, Giradiasis, Helminths: DR Asim ShresthaAsim ShresthaNo ratings yet
- Fascioliasis, TrematodesDocument31 pagesFascioliasis, Trematodesحسین جاسم ستارNo ratings yet
- Ascari As IsDocument4 pagesAscari As IsHassan osmanNo ratings yet
- 01 - Parasitic Infections 2020Document85 pages01 - Parasitic Infections 2020gilbert agudoNo ratings yet
- Lung FlukesDocument23 pagesLung FlukesGelli LebinNo ratings yet
- Oral Cavity and GIT Parasitology NoteDocument15 pagesOral Cavity and GIT Parasitology NoteNAOGE GEDEFANo ratings yet
- Worm Infestation: Ms Alisha TalwarDocument82 pagesWorm Infestation: Ms Alisha TalwarSumon Kumar biswasNo ratings yet
- Acute Gastroenteritis: Defnition and Etiology/Clinical ManifestationsDocument13 pagesAcute Gastroenteritis: Defnition and Etiology/Clinical ManifestationsMia EstadillaNo ratings yet
- Ascaris LumbricoidesDocument24 pagesAscaris LumbricoidesQonik Nuzulul FalakhiNo ratings yet
- AscariasisDocument6 pagesAscariasisPika PearlasNo ratings yet
- AscariasisDocument7 pagesAscariasisMia Angela Del MundoNo ratings yet
- Ascaris LumbricoidesDocument33 pagesAscaris LumbricoidesBio SciencesNo ratings yet
- ANTOLIN, Shelila Hope D. ZETA, Jamaica Mae BSN3-ADocument23 pagesANTOLIN, Shelila Hope D. ZETA, Jamaica Mae BSN3-Arhimineecat71No ratings yet
- Case 2B (Group 8) Blok GITDocument74 pagesCase 2B (Group 8) Blok GITkheluwisNo ratings yet
- CHN Food and WaterDocument4 pagesCHN Food and WatertimmybunsenNo ratings yet
- Nematode Infections 2019 Student PDFDocument272 pagesNematode Infections 2019 Student PDFCharlene SuliganNo ratings yet
- Amphistomiasis, SchistosomiasisDocument15 pagesAmphistomiasis, Schistosomiasisdharmachakra ComNo ratings yet
- 24 FasciolaDocument27 pages24 FasciolaJohnree A. EvangelistaNo ratings yet
- 3 Fasciola and FasciolopsisDocument49 pages3 Fasciola and FasciolopsisSohaib KhanNo ratings yet
- Infcetions Intestinal Protozoal InfectionsDocument40 pagesInfcetions Intestinal Protozoal InfectionsDr.P.NatarajanNo ratings yet
- Diarrhea (Pedia)Document8 pagesDiarrhea (Pedia)Eliza Paula BacudNo ratings yet
- Typhoid Fever: ProfessorDocument48 pagesTyphoid Fever: ProfessormanibharathiNo ratings yet
- Pemicu 3 GITDocument143 pagesPemicu 3 GITMudita DewiNo ratings yet
- Chapter - 2 - C - V-B Infectious - Diarrhea PPT AmnaDocument47 pagesChapter - 2 - C - V-B Infectious - Diarrhea PPT AmnaEmmaNo ratings yet
- ParasitologyDocument43 pagesParasitologyBatool SherbiniNo ratings yet
- Disentri Amoeba TUTORDocument26 pagesDisentri Amoeba TUTORShameer Mohamed AljabarNo ratings yet
- Lecture 15 Infertility in Sheep and GoatsDocument38 pagesLecture 15 Infertility in Sheep and GoatsgnpobsNo ratings yet
- Infertility in Sheep and GoatsDocument38 pagesInfertility in Sheep and GoatsgnpobsNo ratings yet
- Pemicu 3 GIT GraceDocument67 pagesPemicu 3 GIT GraceGrace KahonoNo ratings yet
- Fasciola Hepatica: Adithya Ashok Roll No: 1Document19 pagesFasciola Hepatica: Adithya Ashok Roll No: 1Anjana AshokNo ratings yet
- Communicable and Vector Bone Diseases1) - 1Document175 pagesCommunicable and Vector Bone Diseases1) - 1staceyatienoomaNo ratings yet
- AMOEBIASISDocument31 pagesAMOEBIASISpriyagerard100% (1)
- AmoebiasisDocument29 pagesAmoebiasisFatima murtadaNo ratings yet
- Food Poisoning N AMOEBIASIS - LECTUREDocument60 pagesFood Poisoning N AMOEBIASIS - LECTUREpriyanka100% (1)
- Pemicu 3 GIT BudiDocument67 pagesPemicu 3 GIT BudiGrace KahonoNo ratings yet
- Roundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandRoundworm Infections, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Dengue Prescription and Monitoring CardDocument2 pagesDengue Prescription and Monitoring CardKristin Villaseñor-MercadoNo ratings yet
- M3 Health HomeworkDocument1 pageM3 Health HomeworkKarlyNo ratings yet
- Restorative Management of Dental Implants: 5.1 Basic Implant TerminologyDocument19 pagesRestorative Management of Dental Implants: 5.1 Basic Implant TerminologyleeminhoangrybirdNo ratings yet
- Anatomy McqsDocument3 pagesAnatomy McqsMunazzaNo ratings yet
- Do School Bags Cause Back Pain?Document6 pagesDo School Bags Cause Back Pain?TNo ratings yet
- Gastric LavageDocument15 pagesGastric LavageEm BelandoNo ratings yet
- Afias-1 and Afias-6 BrochuresDocument4 pagesAfias-1 and Afias-6 BrochuresShadreck MabvoroNo ratings yet
- 05 Palmieri-VadalaDocument7 pages05 Palmieri-VadalaSantosNo ratings yet
- Gastroparesis InfoDocument9 pagesGastroparesis Infoडा. सत्यदेव त्यागी आर्य100% (1)
- Cutaneous Leishmania: Dr. Vijayakumar Unki Asst Professor VCGDocument16 pagesCutaneous Leishmania: Dr. Vijayakumar Unki Asst Professor VCGLohith MCNo ratings yet
- HbA1c (Glycosylated HB)Document3 pagesHbA1c (Glycosylated HB)يوسف الشرقاويNo ratings yet
- Practical Approach To GIB, Hemorragia Gastrointestinal, Hemorragia GastricaDocument86 pagesPractical Approach To GIB, Hemorragia Gastrointestinal, Hemorragia GastricaRamiro AlanisNo ratings yet
- CSF AnalysisDocument20 pagesCSF AnalysisEBNo ratings yet
- Endemic and Sporadic GoiterDocument13 pagesEndemic and Sporadic GoiterBtwo SoelNo ratings yet
- Curriculum Dia Rad Gi - Gu RotationDocument2 pagesCurriculum Dia Rad Gi - Gu Rotationmafsd jlNo ratings yet
- NCPDocument2 pagesNCPNikai PabayoNo ratings yet
- Anti-Dystrophin Antibody, Prediluted Ab15278: Product DatasheetDocument3 pagesAnti-Dystrophin Antibody, Prediluted Ab15278: Product DatasheetĐạt Hoàng TrầnNo ratings yet
- Obesity Diagnosis ManagementDocument26 pagesObesity Diagnosis ManagementAdán 'Olveera100% (1)
- Pre-Implant - Prosthodontics 2Document56 pagesPre-Implant - Prosthodontics 2Ameera RabayahNo ratings yet
- Health Assessment in Female GenetaliaDocument175 pagesHealth Assessment in Female GenetaliaChristine LeeNo ratings yet
- Unit 4 VocabularyDocument3 pagesUnit 4 VocabularyAndris RosinNo ratings yet
- Clinical EnzymologyDocument28 pagesClinical EnzymologySparrowNo ratings yet
- Siadh and Di NclexDocument13 pagesSiadh and Di NclexDianne NuñalNo ratings yet
- Fetal CirculationDocument5 pagesFetal CirculationJaime PorscheNo ratings yet
- Vital Dyes For Chromovitrectomy: Colours For The Vitreoretinal Surgeon!!!Document6 pagesVital Dyes For Chromovitrectomy: Colours For The Vitreoretinal Surgeon!!!Dr. liji menonNo ratings yet
- Acid Base: by Adam HollingworthDocument8 pagesAcid Base: by Adam HollingworthIdrissa ContehNo ratings yet
- Lab Assignment: Community Nutrition BS-III (6 Semester)Document23 pagesLab Assignment: Community Nutrition BS-III (6 Semester)huzairaNo ratings yet
- Causes of ObesityDocument3 pagesCauses of ObesityKaren Chambre100% (1)