Download as pptx, pdf, or txt
You might also like
- NATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFDocument700 pagesNATIONAL GUIDELINES ON QUALITY OBSTETRICS AND PERINATAL CARE Final Feb 2022 PDFvincent obunga50% (2)
- Public Health Nursing: Scope and Standards of PracticeFrom EverandPublic Health Nursing: Scope and Standards of PracticeRating: 5 out of 5 stars5/5 (1)
- Kids Ramadan Journal Blue DotDocument35 pagesKids Ramadan Journal Blue Doth_khatimah100% (1)
- MOP Micronutrient SupplementationDocument250 pagesMOP Micronutrient SupplementationRaphael Panotes100% (1)
- State of Content Marketing 2023Document126 pagesState of Content Marketing 2023pavan teja100% (1)
- Doh Programs PDFDocument68 pagesDoh Programs PDFMikaela Lozano100% (2)
- Project Proposal On Child Nutrition For Sustainable Health and Prenatal ClinicDocument6 pagesProject Proposal On Child Nutrition For Sustainable Health and Prenatal Clinicczeremar chan100% (2)
- Starbucks Communications StrategyDocument23 pagesStarbucks Communications Strategyapi-284048334100% (1)
- DOH ProgramsDocument114 pagesDOH ProgramsAlyssandra Luceno100% (6)
- National Guidelines For Quality Obstetrics and Perinatal Care PDFDocument410 pagesNational Guidelines For Quality Obstetrics and Perinatal Care PDFduncan100% (1)
- Maternal Care Package - Full.1-76Document76 pagesMaternal Care Package - Full.1-76goobee93% (14)
- SCHOOL NURSE RESOURCE MANUAL Tenth Edition: Tenth Edition: A Guide to PracticeFrom EverandSCHOOL NURSE RESOURCE MANUAL Tenth Edition: Tenth Edition: A Guide to PracticeNo ratings yet
- Unit 2 - Creative Media IndustryDocument12 pagesUnit 2 - Creative Media Industryapi-425190825100% (1)
- RCH - Reproductive and Child Health Part 1Document21 pagesRCH - Reproductive and Child Health Part 1Dr. Rakshit SolankiNo ratings yet
- Doh ProgramsDocument51 pagesDoh ProgramsDhaneanne Marie ChanNo ratings yet
- Department F Health Plans, Programs, Projects NotesDocument26 pagesDepartment F Health Plans, Programs, Projects NotesEdgar DumagpiNo ratings yet
- Capaian Target Kesehatan Ibu Dan Bayi Di Indonesia (Maret 2015)Document71 pagesCapaian Target Kesehatan Ibu Dan Bayi Di Indonesia (Maret 2015)Gerakan Kesehatan Ibu dan Anak100% (1)
- RCH - Reproductive and Child Health Part 2Document32 pagesRCH - Reproductive and Child Health Part 2Dr. Rakshit SolankiNo ratings yet
- Module 1 NCM 107 NewDocument44 pagesModule 1 NCM 107 NewAmethystNo ratings yet
- CHN & NCDDocument92 pagesCHN & NCDlorelie asisNo ratings yet
- Ehealth in Indonesia Development StrategiesDocument24 pagesEhealth in Indonesia Development StrategiesMansurNo ratings yet
- Department of Health (Doh) ProgramsDocument51 pagesDepartment of Health (Doh) ProgramsDhaneanne Marie ChanNo ratings yet
- MNH Davao Region Toolbox UpdatedDocument57 pagesMNH Davao Region Toolbox UpdatedddesabilleNo ratings yet
- Politicas de Educacion 2013Document30 pagesPoliticas de Educacion 2013Roberto GarciaNo ratings yet
- AMoran - AlignMNH Plenary EPMM ENAP PPT FINALDocument14 pagesAMoran - AlignMNH Plenary EPMM ENAP PPT FINALjedava4724No ratings yet
- Primary Health Care BSNDocument67 pagesPrimary Health Care BSNAmiel Francisco ReyesNo ratings yet
- Doh ProgramsDocument7 pagesDoh ProgramsFatima Grace EchemNo ratings yet
- Nutrition Information SystemDocument7 pagesNutrition Information SystemAbel AgoroNo ratings yet
- ECON4410 Slide 7Document55 pagesECON4410 Slide 7Farjad ImtiazNo ratings yet
- W6 - Nutrition Program, Oral Health Program, Essential Health Packages For The Adolescent, and Older PersonsDocument4 pagesW6 - Nutrition Program, Oral Health Program, Essential Health Packages For The Adolescent, and Older PersonsApostol DyNo ratings yet
- Kesehatan Reproduksi: Department Obstetri & Ginekologi Fakultas Kedokteran USUDocument43 pagesKesehatan Reproduksi: Department Obstetri & Ginekologi Fakultas Kedokteran USUdewi0% (1)
- Strategy: Roadmap For Nutrition in South Africa 2013-2017Document50 pagesStrategy: Roadmap For Nutrition in South Africa 2013-2017Laura Lopez GonzalezNo ratings yet
- Community Health NursingDocument23 pagesCommunity Health Nursingcoy008No ratings yet
- National Health Programmes For Children in IndiaDocument79 pagesNational Health Programmes For Children in IndiashahnazNo ratings yet
- 1.2B Safe Motherhood Program & Women's Health PDFDocument11 pages1.2B Safe Motherhood Program & Women's Health PDFStephen Pilar PortilloNo ratings yet
- Doh Programs Presentation IV FDocument53 pagesDoh Programs Presentation IV FJanine GuevarraNo ratings yet
- National Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024Document78 pagesNational Social and Behaviour Change Communication Strategy For Integrated Ecd Nutrition and Wash 2018-2024rukwavuNo ratings yet
- Mhealth Guide For Newborn Health OnlineDocument34 pagesMhealth Guide For Newborn Health OnlinekithchetrashchNo ratings yet
- National Programmes: DR Nishant Verma Assistant Professor Department of Pediatrics King George's Medical UniversityDocument51 pagesNational Programmes: DR Nishant Verma Assistant Professor Department of Pediatrics King George's Medical UniversityVaishali AmbilkarNo ratings yet
- PCM Primary Health Care Development Goals and DohDocument37 pagesPCM Primary Health Care Development Goals and DohSydrex SarmientoNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentKhenyuza Angel ClementeNo ratings yet
- CHN HandoutsDocument41 pagesCHN Handoutssendang JNo ratings yet
- CBR Assignment SUBMITTED BY:Shawn Jimmy Group:2: Village Rehabilitation Worker AnswerDocument5 pagesCBR Assignment SUBMITTED BY:Shawn Jimmy Group:2: Village Rehabilitation Worker AnswerShawn JimmyNo ratings yet
- Community Health NursingDocument34 pagesCommunity Health NursingJohn Michael ClimacoNo ratings yet
- Health PowerpointDocument40 pagesHealth PowerpointJayden Lorie DecoynaNo ratings yet
- SDG Group1 Beced12aDocument7 pagesSDG Group1 Beced12abeaodiamarNo ratings yet
- Final Presentation - PPTX JATINDocument22 pagesFinal Presentation - PPTX JATINJatin ChaudharyNo ratings yet
- MDG Progress Towards MDG 4 and 5Document25 pagesMDG Progress Towards MDG 4 and 5John Thiong'oNo ratings yet
- Iccm Me PlanDocument64 pagesIccm Me PlanFanciecom TechnologiesNo ratings yet
- Safe MotherhoodDocument27 pagesSafe MotherhoodEsory BasnetNo ratings yet
- Pakistan and SDG3Document20 pagesPakistan and SDG3Minhaj QidwaiNo ratings yet
- Physical PharmaceuticsDocument34 pagesPhysical PharmaceuticsGyanaranjan MallickNo ratings yet
- Arellano UniversityDocument14 pagesArellano UniversityRizalyn VictaNo ratings yet
- Ashish Paliwal Rmncha PDFDocument83 pagesAshish Paliwal Rmncha PDFAshish PaliwalNo ratings yet
- NNC Strategies For Infant and Young Child Nutrition: Consultation Workshop For The 63 WHADocument28 pagesNNC Strategies For Infant and Young Child Nutrition: Consultation Workshop For The 63 WHAKhair SoomroNo ratings yet
- HEALTH PROGRAMS CompleteDocument194 pagesHEALTH PROGRAMS CompleteAbigail AnziaNo ratings yet
- Primary Health CareDocument28 pagesPrimary Health CareJHONESSA LAYOSNo ratings yet
- DOHDocument6 pagesDOHEvan Lloyd Cedeno MirafloresNo ratings yet
- Welcome To The Seminar On: Primary Health Care and Modes of PreventionDocument38 pagesWelcome To The Seminar On: Primary Health Care and Modes of PreventionTom ThomasNo ratings yet
- Nutrition Behavior and CounselingDocument133 pagesNutrition Behavior and CounselingAijeleth AvilaNo ratings yet
- EWEC Globalstrategyreport 200915 FINAL WEB PDFDocument108 pagesEWEC Globalstrategyreport 200915 FINAL WEB PDFRahmad AjisNo ratings yet
- Ational Ealth Rogramme Elated O Hild Elfare: Presented byDocument98 pagesAtional Ealth Rogramme Elated O Hild Elfare: Presented byshubham vermaNo ratings yet
- 3 NationalhealthprogrammesDocument92 pages3 NationalhealthprogrammesABISHAK RAVIKUMARNo ratings yet
- Family Nutrition GuideFrom EverandFamily Nutrition GuideNo ratings yet
- Lampiran Permen 14 TH 2016Document23 pagesLampiran Permen 14 TH 2016h_khatimahNo ratings yet
- Translation KPKDocument37 pagesTranslation KPKh_khatimahNo ratings yet
- Ozzy HoppingDocument16 pagesOzzy Hoppingh_khatimahNo ratings yet
- Seoul Nanjido KoreaDocument25 pagesSeoul Nanjido Koreah_khatimahNo ratings yet
- Envi School: Explaining Complexity of Nature in Fun Way: Logo Eplc, Yuhan Kimberly, KotakuDocument6 pagesEnvi School: Explaining Complexity of Nature in Fun Way: Logo Eplc, Yuhan Kimberly, Kotakuh_khatimahNo ratings yet
- HXM ECP L2 Partner Deep Dive Sales Presentation June 2021Document103 pagesHXM ECP L2 Partner Deep Dive Sales Presentation June 2021tegara2487No ratings yet
- Chelsea Vs Newcastle - Google SearchDocument1 pageChelsea Vs Newcastle - Google SearchfortniteplayerzerobuildNo ratings yet
- UK v. Albania (Corfu Channel Case) Use of ForceDocument2 pagesUK v. Albania (Corfu Channel Case) Use of ForceJacob FerrerNo ratings yet
- (02.08.07) Coletânea de Provas de Inglês Fundação Getúlio VargasDocument115 pages(02.08.07) Coletânea de Provas de Inglês Fundação Getúlio VargasJosé Maurício FreireNo ratings yet
- Intensive-Level Survey of The Washington Heights Area of Washington DC.Document128 pagesIntensive-Level Survey of The Washington Heights Area of Washington DC.Envision Adams MorganNo ratings yet
- Supply Chain Management NotesDocument35 pagesSupply Chain Management NotesRazin GajiwalaNo ratings yet
- Animation Thesis FilmDocument4 pagesAnimation Thesis Filmjuliemedinaphoenix100% (2)
- Sri-Lanka From SamudraNewsAlerts SouthAsiaNewsAlertsDocument342 pagesSri-Lanka From SamudraNewsAlerts SouthAsiaNewsAlertsInvestor BritishNo ratings yet
- Start-Up Success Story PresentationDocument15 pagesStart-Up Success Story PresentationSamarth MittalNo ratings yet
- Buddy HollyDocument3 pagesBuddy Hollyapi-276376703No ratings yet
- LLB102 2023 2 DeferredDocument8 pagesLLB102 2023 2 Deferredlo seNo ratings yet
- Freeman v. Grain Processing Corp., No. 13-0723 (Iowa June 13, 2014)Document63 pagesFreeman v. Grain Processing Corp., No. 13-0723 (Iowa June 13, 2014)RHTNo ratings yet
- India Today 09.11.2020Document66 pagesIndia Today 09.11.2020sures108No ratings yet
- Grapes of WrathDocument3 pagesGrapes of Wrathdoom_lord22No ratings yet
- Bpme1013 Group B Introduction To Entrepreneurship (Full)Document27 pagesBpme1013 Group B Introduction To Entrepreneurship (Full)Randa RamadhanNo ratings yet
- Bts - Butter (CD) Target 2Document1 pageBts - Butter (CD) Target 2ife ogundeleNo ratings yet
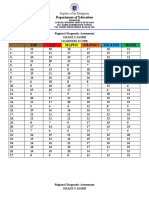
- Raw ScoreDocument2 pagesRaw ScoreDemi Nodado-JamirNo ratings yet
- Tata Acquired Luxury Auto Brands Jaguar and Land Rover - From Ford MotorsDocument15 pagesTata Acquired Luxury Auto Brands Jaguar and Land Rover - From Ford MotorsJoel SaldanhaNo ratings yet
- ANC 103rd Birthday Transport PlanDocument6 pagesANC 103rd Birthday Transport PlanCityPressNo ratings yet
- Regional Development Plan CAR 2017-2022 Chapter 1Document6 pagesRegional Development Plan CAR 2017-2022 Chapter 1Andrew EvangelistaNo ratings yet
- Construction Waste Management ManualDocument31 pagesConstruction Waste Management ManualChethana DeviNo ratings yet
- Gillette India LTD MAK - II Project: Group 6 Section BDocument92 pagesGillette India LTD MAK - II Project: Group 6 Section BPrakhar RatheeNo ratings yet
- Agreements BBG enDocument26 pagesAgreements BBG enRajasheker ReddyNo ratings yet
- Sibal Demo TeachingDocument69 pagesSibal Demo TeachingNizeth Jane Macion CuajotorNo ratings yet
- UntitledDocument18 pagesUntitledjeralyn juditNo ratings yet
- Definition:: Handover NotesDocument3 pagesDefinition:: Handover NotesRalkan KantonNo ratings yet
- Carrick-On-Suir, A Glimpse Into Ireland's HistoryDocument13 pagesCarrick-On-Suir, A Glimpse Into Ireland's HistoryPaul JennepinNo ratings yet