Download as pptx, pdf, or txt
You might also like
- 1.microbiology - Bacteriology MCQs FormattedDocument73 pages1.microbiology - Bacteriology MCQs FormattedDr P N N Reddy94% (17)
- NCP - Poststreptococcal GlomerulonephritisDocument12 pagesNCP - Poststreptococcal GlomerulonephritisAya BolinasNo ratings yet
- Acute Glomerulonephritis: Mohd Zamir Ghouse 060100848Document40 pagesAcute Glomerulonephritis: Mohd Zamir Ghouse 060100848zamirsg100% (1)
- Pathophysiology of NephrosclerosisDocument2 pagesPathophysiology of NephrosclerosisJessica Damasen Caballero0% (1)
- Glomerulonephritis-1 (Dr. Soffa)Document58 pagesGlomerulonephritis-1 (Dr. Soffa)Rahmailla Khanza Diana FebriliantriNo ratings yet
- DM NCPDocument2 pagesDM NCPVirgilio Reyes ManuelNo ratings yet
- Anemia Unspecified FinalDocument47 pagesAnemia Unspecified FinalMaria Paula BungayNo ratings yet
- Pahtophysiology of EsrdDocument5 pagesPahtophysiology of EsrdCarl JardelezaNo ratings yet
- Pathophys of JaundiceDocument1 pagePathophys of JaundiceNathan Vince CruzNo ratings yet
- How To Make Your Own Colloidal SilverDocument21 pagesHow To Make Your Own Colloidal Silverrawzero92% (12)
- Paper 4 Publication 333Document14 pagesPaper 4 Publication 333leBariNo ratings yet
- Acute Glomerulonephritis 42-mDocument27 pagesAcute Glomerulonephritis 42-mcbanguisNo ratings yet
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case StudyPrincess Tindugan100% (1)
- Acute Glomerulonephritis - CSDocument31 pagesAcute Glomerulonephritis - CSMASIINo ratings yet
- Acute GlomerularnephritisDocument17 pagesAcute GlomerularnephritiszamirsgNo ratings yet
- Case Study - Acute Glomerulonephritis Sample Case Study Report For PCL Level by Amrit BanstolaDocument15 pagesCase Study - Acute Glomerulonephritis Sample Case Study Report For PCL Level by Amrit BanstolaAmrit Banstola100% (5)
- Acute Glomerulonephritis: Gordon Sara Sonnya Ayutthaya Novita Sari DewiDocument12 pagesAcute Glomerulonephritis: Gordon Sara Sonnya Ayutthaya Novita Sari DewiSara Sonnya Ayutthaya NapitupuluNo ratings yet
- Cs AGNDocument177 pagesCs AGNMa Rafaela Rosales PalomponNo ratings yet
- Acute Glomerulonephritis (AGN)Document5 pagesAcute Glomerulonephritis (AGN)smashayielNo ratings yet
- Case StudyDocument41 pagesCase StudyAubrey Ann FolloscoNo ratings yet
- Acute GlumerulonephritisDocument77 pagesAcute GlumerulonephritisNicoleNo ratings yet
- Acute GlomerulonephritisDocument57 pagesAcute Glomerulonephritisynadelcastillo100% (7)
- Acute Glomerulonephritis Case StudyDocument12 pagesAcute Glomerulonephritis Case Study19lyon92100% (6)
- Case Study: Acute GlomerulonephritisDocument28 pagesCase Study: Acute GlomerulonephritisMa Rafaela Rosales Palompon91% (11)
- HyponatremiaDocument6 pagesHyponatremiaJaymart Saclolo CostillasNo ratings yet
- Hyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)Document8 pagesHyperosmolar Hyperglycemic Nonketotic Syndrome (HHNS)amiraNo ratings yet
- Agn NCPDocument11 pagesAgn NCPRaidis PangilinanNo ratings yet
- Case StudyDocument26 pagesCase Studyamazing grace mejia carlos100% (2)
- Case AGNDocument66 pagesCase AGNMohaima PanditaNo ratings yet
- Nursing Care Plan (NCP) : Patient & Family Centered (In Priority Order)Document1 pageNursing Care Plan (NCP) : Patient & Family Centered (In Priority Order)WorodNo ratings yet
- Acute GlomerulonephritisDocument17 pagesAcute GlomerulonephritisBayanSecond WardNo ratings yet
- Post-Partum Hemorrhage Pathophysiology PaperDocument5 pagesPost-Partum Hemorrhage Pathophysiology Paperapi-399619969No ratings yet
- NCP CSDocument7 pagesNCP CSTwobee Kriz LeghidNo ratings yet
- Schistosomiasis (From Anatomy To Pathophysiology)Document10 pagesSchistosomiasis (From Anatomy To Pathophysiology)Tiger Knee100% (1)
- ABRUPTIO PLACENTAE PathophysiologyDocument3 pagesABRUPTIO PLACENTAE PathophysiologyBarda GulanNo ratings yet
- Case Study 102Document6 pagesCase Study 102Cheska Lopez100% (1)
- Acute GlomerulonephritisDocument12 pagesAcute Glomerulonephritiskuchaibaru90No ratings yet
- Acute BronchitisDocument38 pagesAcute BronchitisNikko MelencionNo ratings yet
- SiadhDocument10 pagesSiadhehjing75% (4)
- St. Anne College Lucena Inc. Diversion Road G-Gulang Lucena CityDocument22 pagesSt. Anne College Lucena Inc. Diversion Road G-Gulang Lucena CitymcensoredNo ratings yet
- Case 1 (Pneumonia) ArioDocument26 pagesCase 1 (Pneumonia) ArioJoegie ArioNo ratings yet
- NCP AgnDocument2 pagesNCP Agnj3nann3No ratings yet
- Benign Prostatic Hyperplasia (NCP)Document4 pagesBenign Prostatic Hyperplasia (NCP)24 PAULINO ALDRIN MUJARNo ratings yet
- Acute Glomerulonephritis (AGN)Document35 pagesAcute Glomerulonephritis (AGN)jennalyn_dejelo100% (1)
- Drug Studies and Health Teaching PlanDocument28 pagesDrug Studies and Health Teaching PlansfkjalkhsafgNo ratings yet
- Acute Glomerulonephritis PathophysiologyDocument4 pagesAcute Glomerulonephritis PathophysiologyChester NicoleNo ratings yet
- Lupus Case ReportDocument1 pageLupus Case ReportMendy HararyNo ratings yet
- Unit 3 Assessment Sitaca Tan Viedor Yap BSN 2cDocument9 pagesUnit 3 Assessment Sitaca Tan Viedor Yap BSN 2capi-532152575No ratings yet
- HyperphosphatemiaDocument2 pagesHyperphosphatemiatephNo ratings yet
- Novilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Hemophilia: St. Paul College of Ilocos SurCharina AubreyNo ratings yet
- Case On ColitisDocument34 pagesCase On ColitisAamer SyedNo ratings yet
- Assessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationDocument6 pagesAssessment Nsg. Diagnosis Sci. Explanation Planning Intervention Rationale EvaluationRoMarie AbainzaNo ratings yet
- Pathophy - Nephrotic SyndromeedDocument1 pagePathophy - Nephrotic Syndromeedianecunar100% (1)
- NCP MiDocument4 pagesNCP MiPitaca Madiam Annabehl PaulNo ratings yet
- Final Case StudyDocument13 pagesFinal Case StudyJen Gacula OsinNo ratings yet
- Individual Case Study Acute GlomerulonephritisDocument26 pagesIndividual Case Study Acute GlomerulonephritisMonique ReyesNo ratings yet
- Case Report Jai 3Document8 pagesCase Report Jai 3EACMed Nursing Station 5th FloorNo ratings yet
- Acute Glomerulonephritis Is A Disease Characterized by The Sudden Appearance of EdemaDocument9 pagesAcute Glomerulonephritis Is A Disease Characterized by The Sudden Appearance of Edemamelissa guillermoNo ratings yet
- Case Study yDocument23 pagesCase Study yRaidis PangilinanNo ratings yet
- 95873u77 PrintDocument21 pages95873u77 PrintAdelina PopaNo ratings yet
- Acute Poststreptococcal GlomerulonephritisDocument58 pagesAcute Poststreptococcal GlomerulonephritisALI MUMTAZNo ratings yet
- Nephrotic Syndrome in ChildrenDocument12 pagesNephrotic Syndrome in ChildrenLaras Ciingu SyahrezaNo ratings yet
- Case 2-1-1Document11 pagesCase 2-1-1Shakshi RainaNo ratings yet
- 5 Major Diseases and TreatmentsDocument11 pages5 Major Diseases and Treatmentsiangould12No ratings yet
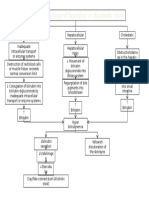
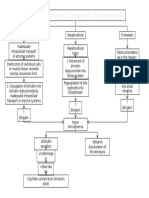
- Pathophysiology CKD Secondary To CGNDocument1 pagePathophysiology CKD Secondary To CGNNathan Vince CruzNo ratings yet
- Pathophysiology of JaundiceDocument1 pagePathophysiology of JaundiceNathan Vince CruzNo ratings yet
- Modifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsDocument1 pageModifiable Risk Factors Non-Modifiable Risk Factors: Physical Assessment Findings Lab Result FindingsNathan Vince CruzNo ratings yet
- Pathophy CKD Secondary To CGNDocument1 pagePathophy CKD Secondary To CGNNathan Vince CruzNo ratings yet
- Infective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableDocument1 pageInfective Endocarditis: Non-Modifiable Age Congenital Heart Disease Gender Preexisting Heart Conditions ModifiableNathan Vince CruzNo ratings yet
- Diabetic Ketoacidosis Case PresentationDocument37 pagesDiabetic Ketoacidosis Case PresentationNathan Vince Cruz100% (2)
- Sputum AnalysisDocument12 pagesSputum AnalysisAdriana GarciaNo ratings yet
- Dental NotesDocument12 pagesDental NotesFaye Nervanna Alecha AlferezNo ratings yet
- Yersinia Pestis V Protein Epitopes Recognized by CD4 T CellsDocument8 pagesYersinia Pestis V Protein Epitopes Recognized by CD4 T CellsHerdi ArdianaNo ratings yet
- 27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiDocument14 pages27 Purpureal Venous Thrombosis and Pulmonary Embolism by Shambuling HebballiSamhitha Ayurvedic ChennaiNo ratings yet
- Case Study DengueDocument11 pagesCase Study DengueCarl Julienne MasangcayNo ratings yet
- African Healthcare Setting VHF PDFDocument209 pagesAfrican Healthcare Setting VHF PDFWill TellNo ratings yet
- Bios Life Slim UAEDocument4 pagesBios Life Slim UAEJey BautistaNo ratings yet
- Item 2 Models of Health and Health CareDocument7 pagesItem 2 Models of Health and Health CareSarah LambleyNo ratings yet
- The Mortality of Cholera in EnglandDocument506 pagesThe Mortality of Cholera in England杨振宇No ratings yet
- Grade 11 Eng and MyanDocument20 pagesGrade 11 Eng and Myanrobben11175% (4)
- It 25 - JHP RLDDocument52 pagesIt 25 - JHP RLDkalajengkingkalakalaNo ratings yet
- 12 FilovirusesDocument15 pages12 FilovirusesJames WilliamNo ratings yet
- Journal PNTD 0006822Document22 pagesJournal PNTD 0006822Ade margusNo ratings yet
- Sterilization and Disinfection in OrthodonticsDocument16 pagesSterilization and Disinfection in OrthodonticswaterbayNo ratings yet
- Reflection Paper Outbreak Movie QuestionsDocument3 pagesReflection Paper Outbreak Movie QuestionsNicoleFrias100% (1)
- College of Medicine & Health SciencesDocument56 pagesCollege of Medicine & Health SciencesMebratu DemessNo ratings yet
- CAE Use of EnglishDocument7 pagesCAE Use of Englishali_nusNo ratings yet
- Respiratory AcidosisDocument16 pagesRespiratory AcidosisIssa GutierrezNo ratings yet
- Mikosis ParuDocument33 pagesMikosis ParuselviaNo ratings yet
- Consideration of Disease Through Prashna Kundali: Planets Related To DiseasesDocument3 pagesConsideration of Disease Through Prashna Kundali: Planets Related To Diseasesrahul106100% (1)
- Ent Question PaperDocument23 pagesEnt Question PaperGirish SubashNo ratings yet
- Notice: Federal Management Regulation: Real Property Policies UpdateDocument2 pagesNotice: Federal Management Regulation: Real Property Policies UpdateJustia.comNo ratings yet
- Arbo VirusesDocument67 pagesArbo Virusesneelam badruddin100% (1)
- CPH - Health and Development of My CommunityDocument1 pageCPH - Health and Development of My Communityangela roperezNo ratings yet
- Course Outline - Him73030 101 - Epidemiology Population Health and Public HealthDocument3 pagesCourse Outline - Him73030 101 - Epidemiology Population Health and Public Healthapi-382689726No ratings yet
- Latihan Soal Asking For Attention and Checking UnderstandingDocument4 pagesLatihan Soal Asking For Attention and Checking UnderstandingKevin ChandraNo ratings yet
- Open Veins of Latin America Essay (Autoguardado)Document6 pagesOpen Veins of Latin America Essay (Autoguardado)Scarleth Caroline Bula Paez50% (2)