
Kuliah Antiepilepsi
Kuliah Antiepilepsi
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Assessment Qs 20160501Document10 pagesMedical Assessment Qs 20160501jaish8904No ratings yet
- GI BleedDocument96 pagesGI Bleedjaish8904100% (2)
- Population Dynamics and Control of ContraceptionDocument16 pagesPopulation Dynamics and Control of Contraceptionjaish8904No ratings yet
- HORMONAL CONTRACEPTION PresentationDocument25 pagesHORMONAL CONTRACEPTION Presentationjaish8904100% (1)
- Histology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana UniversityDocument39 pagesHistology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana Universityjaish8904No ratings yet
- Blood Grouping (BCS) LDocument10 pagesBlood Grouping (BCS) Ljaish8904No ratings yet
- Name: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal InfluenzaDocument13 pagesName: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal Influenzajaish8904No ratings yet
- Cohort 1Document25 pagesCohort 1jaish8904No ratings yet
- PitcDocument12 pagesPitcjaish8904No ratings yet
- Lecture Wirawan Ing Desk Cross Sectional 2009Document22 pagesLecture Wirawan Ing Desk Cross Sectional 2009jaish8904No ratings yet
- 4) Crude, Specific and Adjusted RateDocument19 pages4) Crude, Specific and Adjusted Ratejaish8904100% (1)
- Care Support TreatmentDocument10 pagesCare Support Treatmentjaish8904No ratings yet
- Management of InfluenzaDocument14 pagesManagement of Influenzajaish8904No ratings yet
- Kuliah Blok Growth and DevelopmentDocument44 pagesKuliah Blok Growth and Developmentjaish8904No ratings yet
- 3) Measurement of Mortality and MorbidityDocument21 pages3) Measurement of Mortality and Morbidityjaish8904100% (1)
- "Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"Document11 pages"Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"jaish8904No ratings yet
- Conse LingDocument39 pagesConse Lingjaish8904No ratings yet
- Neonatal Nutrition: Mohammad KhassawnehDocument34 pagesNeonatal Nutrition: Mohammad Khassawnehjaish8904No ratings yet
- Management Report 2012Document41 pagesManagement Report 2012Daniela AlimanNo ratings yet
- Emergency Preparedness For Severe WeatherDocument2 pagesEmergency Preparedness For Severe WeatherRandy PedrozaNo ratings yet
- BARTECDocument252 pagesBARTECHoangNo ratings yet
- Pelaporan IKP Puskesmas Arjaty Daud 2022Document16 pagesPelaporan IKP Puskesmas Arjaty Daud 2022Fajar Slalu CeriaNo ratings yet
- Craftsman Garden Tractor 917287451Document68 pagesCraftsman Garden Tractor 917287451mabe002No ratings yet
- This Set of Building Construction Multiple Choice QuestionsDocument5 pagesThis Set of Building Construction Multiple Choice QuestionspransuNo ratings yet
- Glycemic Targets 2022Document14 pagesGlycemic Targets 2022Tom BiusoNo ratings yet
- 2007 06 08 OA FEA Kalaeloa Asphalt TerminalDocument255 pages2007 06 08 OA FEA Kalaeloa Asphalt TerminalEsteban Lopez ArboledaNo ratings yet
- ĐỀ 51Document9 pagesĐỀ 51bichngocvonagiNo ratings yet
- THE INDEPENDENT Issue 558Document44 pagesTHE INDEPENDENT Issue 558The Independent MagazineNo ratings yet
- FamiliesDocument26 pagesFamiliesChaoukiNo ratings yet
- Parole: Ca 2 - Non-Institutional CorrectionsDocument8 pagesParole: Ca 2 - Non-Institutional CorrectionsWena Mae Cristobal100% (5)
- Abridged Translation of Wombat-Zine Vol. 1Document6 pagesAbridged Translation of Wombat-Zine Vol. 1Yuto TsunodaNo ratings yet
- Technical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000Document88 pagesTechnical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000mohammad khoraminiaNo ratings yet
- Ebook Encyclopedia of Cardiovascular Research and Medicine PDF Full Chapter PDFDocument47 pagesEbook Encyclopedia of Cardiovascular Research and Medicine PDF Full Chapter PDFkimberly.dixon591100% (30)
- DNA DR In-Class ActivitiesDocument15 pagesDNA DR In-Class ActivitiesCéline Engels100% (1)
- UntitledDocument55 pagesUntitledJerko AndreićNo ratings yet
- Biotechnology Study GuideDocument24 pagesBiotechnology Study GuideÖzlem ErdemNo ratings yet
- Product Manual 3055Document5 pagesProduct Manual 3055North EastNo ratings yet
- 57-Online Rejection Note, Material ReturnDocument3 pages57-Online Rejection Note, Material Returnananth100% (1)
- Programme Title:: (Dd/mm/yyyy) (XXX)Document4 pagesProgramme Title:: (Dd/mm/yyyy) (XXX)ghanNo ratings yet
- Nauli-The Key To ConfidenceDocument4 pagesNauli-The Key To ConfidencekailashchsabatNo ratings yet
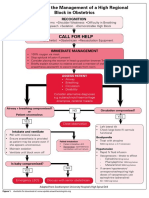
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- Alternatives To Shifting Cultivation-248Document9 pagesAlternatives To Shifting Cultivation-248Chandrashekhar KhobragadeNo ratings yet
- The Domestication and Use of Poultry PDFDocument87 pagesThe Domestication and Use of Poultry PDFKamila JotNo ratings yet
- MSDS AltDocument6 pagesMSDS AltPuskesmas Tambakboyo TubanNo ratings yet
- Invisible InkDocument6 pagesInvisible InkMary Rose BaluranNo ratings yet
- FlicDocument18 pagesFlicLima Limón LimoneroNo ratings yet
- Kiln Inlet Analyzer.: CalibrationDocument3 pagesKiln Inlet Analyzer.: CalibrationZakariya ChoudharyNo ratings yet
- Work at Heights Risk Assessment and PermitDocument4 pagesWork at Heights Risk Assessment and PermitNikola StojanovNo ratings yet






















































































Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Medical Assessment Qs 20160501Document10 pagesMedical Assessment Qs 20160501jaish8904No ratings yet
- GI BleedDocument96 pagesGI Bleedjaish8904100% (2)
- Population Dynamics and Control of ContraceptionDocument16 pagesPopulation Dynamics and Control of Contraceptionjaish8904No ratings yet
- HORMONAL CONTRACEPTION PresentationDocument25 pagesHORMONAL CONTRACEPTION Presentationjaish8904100% (1)
- Histology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana UniversityDocument39 pagesHistology of Nervous System: Dr. I Wayan Sugiritama, M.Kes Histology Department Medical Faculty of Udayana Universityjaish8904No ratings yet
- Blood Grouping (BCS) LDocument10 pagesBlood Grouping (BCS) Ljaish8904No ratings yet
- Name: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal InfluenzaDocument13 pagesName: Sujala Manakandan Nim Num: 0902005188 Sememster: 3/ Klas B Topic: Seasonal Influenzajaish8904No ratings yet
- Cohort 1Document25 pagesCohort 1jaish8904No ratings yet
- PitcDocument12 pagesPitcjaish8904No ratings yet
- Lecture Wirawan Ing Desk Cross Sectional 2009Document22 pagesLecture Wirawan Ing Desk Cross Sectional 2009jaish8904No ratings yet
- 4) Crude, Specific and Adjusted RateDocument19 pages4) Crude, Specific and Adjusted Ratejaish8904100% (1)
- Care Support TreatmentDocument10 pagesCare Support Treatmentjaish8904No ratings yet
- Management of InfluenzaDocument14 pagesManagement of Influenzajaish8904No ratings yet
- Kuliah Blok Growth and DevelopmentDocument44 pagesKuliah Blok Growth and Developmentjaish8904No ratings yet
- 3) Measurement of Mortality and MorbidityDocument21 pages3) Measurement of Mortality and Morbidityjaish8904100% (1)
- "Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"Document11 pages"Diagnostic Testing": "Sensitivity" "Specificity" "Predictive Value"jaish8904No ratings yet
- Conse LingDocument39 pagesConse Lingjaish8904No ratings yet
- Neonatal Nutrition: Mohammad KhassawnehDocument34 pagesNeonatal Nutrition: Mohammad Khassawnehjaish8904No ratings yet
- Management Report 2012Document41 pagesManagement Report 2012Daniela AlimanNo ratings yet
- Emergency Preparedness For Severe WeatherDocument2 pagesEmergency Preparedness For Severe WeatherRandy PedrozaNo ratings yet
- BARTECDocument252 pagesBARTECHoangNo ratings yet
- Pelaporan IKP Puskesmas Arjaty Daud 2022Document16 pagesPelaporan IKP Puskesmas Arjaty Daud 2022Fajar Slalu CeriaNo ratings yet
- Craftsman Garden Tractor 917287451Document68 pagesCraftsman Garden Tractor 917287451mabe002No ratings yet
- This Set of Building Construction Multiple Choice QuestionsDocument5 pagesThis Set of Building Construction Multiple Choice QuestionspransuNo ratings yet
- Glycemic Targets 2022Document14 pagesGlycemic Targets 2022Tom BiusoNo ratings yet
- 2007 06 08 OA FEA Kalaeloa Asphalt TerminalDocument255 pages2007 06 08 OA FEA Kalaeloa Asphalt TerminalEsteban Lopez ArboledaNo ratings yet
- ĐỀ 51Document9 pagesĐỀ 51bichngocvonagiNo ratings yet
- THE INDEPENDENT Issue 558Document44 pagesTHE INDEPENDENT Issue 558The Independent MagazineNo ratings yet
- FamiliesDocument26 pagesFamiliesChaoukiNo ratings yet
- Parole: Ca 2 - Non-Institutional CorrectionsDocument8 pagesParole: Ca 2 - Non-Institutional CorrectionsWena Mae Cristobal100% (5)
- Abridged Translation of Wombat-Zine Vol. 1Document6 pagesAbridged Translation of Wombat-Zine Vol. 1Yuto TsunodaNo ratings yet
- Technical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000Document88 pagesTechnical Data Demag Hoist Units Volume 2: Double-Rail Crab EZDH 600 - EZDH 1000 Double-Rail Crab EZLDH 600 - EZLDH 2000mohammad khoraminiaNo ratings yet
- Ebook Encyclopedia of Cardiovascular Research and Medicine PDF Full Chapter PDFDocument47 pagesEbook Encyclopedia of Cardiovascular Research and Medicine PDF Full Chapter PDFkimberly.dixon591100% (30)
- DNA DR In-Class ActivitiesDocument15 pagesDNA DR In-Class ActivitiesCéline Engels100% (1)
- UntitledDocument55 pagesUntitledJerko AndreićNo ratings yet
- Biotechnology Study GuideDocument24 pagesBiotechnology Study GuideÖzlem ErdemNo ratings yet
- Product Manual 3055Document5 pagesProduct Manual 3055North EastNo ratings yet
- 57-Online Rejection Note, Material ReturnDocument3 pages57-Online Rejection Note, Material Returnananth100% (1)
- Programme Title:: (Dd/mm/yyyy) (XXX)Document4 pagesProgramme Title:: (Dd/mm/yyyy) (XXX)ghanNo ratings yet
- Nauli-The Key To ConfidenceDocument4 pagesNauli-The Key To ConfidencekailashchsabatNo ratings yet
- Algorithm For The Management of A High Regional Block in ObstetricsDocument5 pagesAlgorithm For The Management of A High Regional Block in ObstetricsRaditya DidotNo ratings yet
- Alternatives To Shifting Cultivation-248Document9 pagesAlternatives To Shifting Cultivation-248Chandrashekhar KhobragadeNo ratings yet
- The Domestication and Use of Poultry PDFDocument87 pagesThe Domestication and Use of Poultry PDFKamila JotNo ratings yet
- MSDS AltDocument6 pagesMSDS AltPuskesmas Tambakboyo TubanNo ratings yet
- Invisible InkDocument6 pagesInvisible InkMary Rose BaluranNo ratings yet
- FlicDocument18 pagesFlicLima Limón LimoneroNo ratings yet
- Kiln Inlet Analyzer.: CalibrationDocument3 pagesKiln Inlet Analyzer.: CalibrationZakariya ChoudharyNo ratings yet
- Work at Heights Risk Assessment and PermitDocument4 pagesWork at Heights Risk Assessment and PermitNikola StojanovNo ratings yet