Download as ppt, pdf, or txt
You might also like
- ACLSDocument61 pagesACLSmgthida935100% (1)
- GrissDocument9 pagesGrissEduardo Ignacio Méndez GaldamesNo ratings yet
- Basic Life Support (BLS) Provider HandbookFrom EverandBasic Life Support (BLS) Provider HandbookRating: 5 out of 5 stars5/5 (2)
- Adult Advanced Life Support: Resuscitation Council (UK)Document23 pagesAdult Advanced Life Support: Resuscitation Council (UK)Masuma SarkerNo ratings yet
- Basic Life Support 2017Document40 pagesBasic Life Support 2017Vega E Rahma WNo ratings yet
- NRC - Skill Competency Checklist - PainAsessmentOlderAdults - SkillChecklistDocument2 pagesNRC - Skill Competency Checklist - PainAsessmentOlderAdults - SkillChecklist紅玉練No ratings yet
- CPR & Electrical TherapiesDocument67 pagesCPR & Electrical TherapiesRizaldy Yoga67% (3)
- Advanced Cardiac Life SupportDocument42 pagesAdvanced Cardiac Life SupportDennis MiritiNo ratings yet
- 2015 AHA Science Updates - Ali HaedarDocument39 pages2015 AHA Science Updates - Ali HaedarEndar EszterNo ratings yet
- 2010 Guidelines For CPR Winner MalangDocument55 pages2010 Guidelines For CPR Winner MalangDARA INDAH PRATIWINo ratings yet
- UntitledDocument11 pagesUntitledAnkita BramheNo ratings yet
- Advanced Cardiovascular Life Support (ACLS)Document27 pagesAdvanced Cardiovascular Life Support (ACLS)Sara Ali100% (4)
- Paediatric Advanced Life Support: Resuscitation Council (UK)Document12 pagesPaediatric Advanced Life Support: Resuscitation Council (UK)zacklim_2000100% (1)
- Cardiac Arrest - BLS-ACLS - Dr. KhaledDocument93 pagesCardiac Arrest - BLS-ACLS - Dr. Khaledrony ghoshNo ratings yet
- Basic Life Support: BY Himanshu Rathore M.Sc. Nursing 1 YearDocument30 pagesBasic Life Support: BY Himanshu Rathore M.Sc. Nursing 1 YearHimanshu RathoreNo ratings yet
- From MedscapeCME Clinical BriefsDocument4 pagesFrom MedscapeCME Clinical Briefssraji64No ratings yet
- CPR LectureDocument9 pagesCPR LecturejacnpoyNo ratings yet
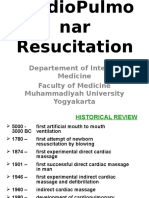
- Departement of Internal Medicine Faculty of Medicine Muhammadiyah University YogyakartaDocument59 pagesDepartement of Internal Medicine Faculty of Medicine Muhammadiyah University YogyakartaMohammad ArifiantoNo ratings yet
- Basic Life SupportDocument4 pagesBasic Life Supportraven_claw25No ratings yet
- Cardio Pulmonary R Ry Resuscitation 2010Document26 pagesCardio Pulmonary R Ry Resuscitation 2010Fatahillah NazarNo ratings yet
- Cardiopulmonary Resuscitation 2015Document31 pagesCardiopulmonary Resuscitation 2015Clarissa Maya TjahjosarwonoNo ratings yet
- BLS Study Guide PDFDocument12 pagesBLS Study Guide PDFPingChavez100% (1)
- AclsDocument44 pagesAclsArchana GaonkarNo ratings yet
- Basic Life SupportDocument10 pagesBasic Life SupportAlvin M AlcaynoNo ratings yet
- The Main Changes in The Resuscitation GuidelinesDocument79 pagesThe Main Changes in The Resuscitation GuidelinesFikri AlfarisyiNo ratings yet
- Cardio Pulmonary Resuscitation 2010: Djayanti SariDocument26 pagesCardio Pulmonary Resuscitation 2010: Djayanti SariAlessandro AlfieriNo ratings yet
- The 2015 Bls Acls Guidelines EnaDocument36 pagesThe 2015 Bls Acls Guidelines EnaAstriTaufiRamadhaniNo ratings yet
- 2010 AHA Guidelines For CPR and ECC Summary TableDocument0 pages2010 AHA Guidelines For CPR and ECC Summary TableUtami HandayaniNo ratings yet
- CPR - 2022Document37 pagesCPR - 2022nguyentaduymy2005No ratings yet
- CPR PDFDocument37 pagesCPR PDFArdhi AgustjikNo ratings yet
- Cardio-Pulmonary Resuscitation (CPR)Document18 pagesCardio-Pulmonary Resuscitation (CPR)Savita HanamsagarNo ratings yet
- Saudi CPR Guidlines in EnglishDocument16 pagesSaudi CPR Guidlines in EnglishpiyushbamsNo ratings yet
- Comparison Sheet Based On 2010 AHA Guidelines For CPR and ECC BLS ChangesDocument5 pagesComparison Sheet Based On 2010 AHA Guidelines For CPR and ECC BLS ChangesCupit NubillisNo ratings yet
- Lectii ScoalaDocument43 pagesLectii ScoalaGaudiMateiNo ratings yet
- Basic Life SupportDocument15 pagesBasic Life SupportMizzy Wat EvaNo ratings yet
- Basic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)Document35 pagesBasic Life Support (BLS) and Advanced Cardiovascular Life Support (ACLS)rajNo ratings yet
- CPR Guidelines. W. WieczorekDocument61 pagesCPR Guidelines. W. WieczorekMarga KouryNo ratings yet
- Basic Cardiac Life Support 2011Document6 pagesBasic Cardiac Life Support 2011Tashfeen Bin NazeerNo ratings yet
- Executive Summary VF20101018Document24 pagesExecutive Summary VF20101018Dana SoimuNo ratings yet
- 9 - ACLS - Part 1Document50 pages9 - ACLS - Part 1Mohnmad ZaitoonNo ratings yet
- Cardiopulmonar Y ResuscitationDocument34 pagesCardiopulmonar Y ResuscitationRatuSitiKhadijahSarahNo ratings yet
- Guidelines Adult Advanced Life SupportDocument34 pagesGuidelines Adult Advanced Life SupportParvathy R NairNo ratings yet
- CPR 2014 SeminarDocument43 pagesCPR 2014 SeminarMinale MenberuNo ratings yet
- Guidelines Adult Advanced Life SupportDocument35 pagesGuidelines Adult Advanced Life SupportindahNo ratings yet
- Bls Update: (The Following Was Taken From AHA Currents Magazine)Document7 pagesBls Update: (The Following Was Taken From AHA Currents Magazine)Allan DangloseNo ratings yet
- Civic Welfare Training ServiceDocument13 pagesCivic Welfare Training ServiceVanessa Rose RofloNo ratings yet
- Basic Life Support Perubahan Guideline AHA 2005-2010Document22 pagesBasic Life Support Perubahan Guideline AHA 2005-2010Momoh AlkaffNo ratings yet
- ACLS Study Guide 1Document19 pagesACLS Study Guide 1CARTAGENA1No ratings yet
- Cardio Pulm ResuscitationDocument7 pagesCardio Pulm Resuscitationdaniphilip777No ratings yet
- Acls 2015Document13 pagesAcls 2015I Gede Aditya100% (5)
- Basic Concept of BLS: Muhammad SaleemDocument27 pagesBasic Concept of BLS: Muhammad Saleemms khanNo ratings yet
- American Heart Association Guidelines For CPR 2015: Christopher RyalinoDocument50 pagesAmerican Heart Association Guidelines For CPR 2015: Christopher RyalinoLightNo ratings yet
- Advanced Life Support-RESSU CouncilDocument30 pagesAdvanced Life Support-RESSU CouncilGigel DumitruNo ratings yet
- On CPRDocument32 pagesOn CPRPiyush Dutta100% (1)
- ACLS Online Training Material: Unit One: General ConceptsDocument34 pagesACLS Online Training Material: Unit One: General ConceptsJohn JenjinsNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- College of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPDocument7 pagesCollege of Physical and Respiratory Therapy S.Y. 2016-2017: Bernardo Tayaban JR., PTRP Maverick Kaypee Colet, PTRPVanessa Yvonne GurtizaNo ratings yet
- Dorn Method Certification CourseDocument10 pagesDorn Method Certification Coursejpepe100% (1)
- Reiki BrochureDocument2 pagesReiki BrochureShikha AgarwalNo ratings yet
- Diagnosis and Management of Post-Traumatic Stress DisorderDocument6 pagesDiagnosis and Management of Post-Traumatic Stress DisorderGeorge PruteanuNo ratings yet
- Role of Clinical Nurse Specialist and EbpDocument10 pagesRole of Clinical Nurse Specialist and Ebpapi-255626529No ratings yet
- Assessment in Geriatric PatientsDocument14 pagesAssessment in Geriatric Patientsنور حسليندا اسحاقNo ratings yet
- NicotexDocument7 pagesNicotexnaina_cutie0% (1)
- 8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudyDocument8 pages8 - Clinical Outcome in Periradicular Surgery Effect of Patient - and Tooth-Related Factors - A Multicenter StudykochikaghochiNo ratings yet
- Poliadenitis NodosaDocument5 pagesPoliadenitis NodosaRicardo Uzcategui ArreguiNo ratings yet
- Ernest Rossi Mind Body PsychotherapyDocument8 pagesErnest Rossi Mind Body PsychotherapyFernandoNo ratings yet
- ThymomasDocument6 pagesThymomasAsmara SyedNo ratings yet
- Blood Chemistry TestsDocument3 pagesBlood Chemistry TestsMarcelina ElizabethNo ratings yet
- Seminar 5 - Traumatic Dislocation and Common Soft Tissue Injury - 2Document149 pagesSeminar 5 - Traumatic Dislocation and Common Soft Tissue Injury - 2Star CruiseNo ratings yet
- Normal Factor LevelsDocument2 pagesNormal Factor LevelsY. MadhuriNo ratings yet
- On Co Nephrology CurriculumDocument130 pagesOn Co Nephrology CurriculumPopy TheresiaNo ratings yet
- Pulp Dentin BiologyDocument21 pagesPulp Dentin BiologyCristiane VazNo ratings yet
- Massive Transfusion Protocol-BbhDocument17 pagesMassive Transfusion Protocol-Bbhkrgdurai100% (2)
- Causes and Treatment For MeningitisDocument21 pagesCauses and Treatment For MeningitisJoyce Suzzane HyuugaNo ratings yet
- 13 Signs of Narcissists Who Sabotage Your Happiness - Diseases CureDocument6 pages13 Signs of Narcissists Who Sabotage Your Happiness - Diseases Curetigerlo75100% (1)
- Defintion of Yoga Therapy 6Document1 pageDefintion of Yoga Therapy 6Sneh Saroj Yeshwant SankpalNo ratings yet
- Coaching Young AthletesDocument51 pagesCoaching Young AthletesMuss BombNo ratings yet
- CPI CriteriaDocument8 pagesCPI CriteriaMichael KoernerNo ratings yet
- Femto LDV Z6Document4 pagesFemto LDV Z6Francisco GomezNo ratings yet
- Isolation of The Operating FieldDocument15 pagesIsolation of The Operating FieldHawzheen SaeedNo ratings yet
- Bielenda Professional Catalogue enDocument88 pagesBielenda Professional Catalogue enBielendaProfessionalNo ratings yet
- Penicillins: Presented By, DR Noor JahanDocument58 pagesPenicillins: Presented By, DR Noor JahanSally PujaNo ratings yet
- Pharmaceutical ExcipientsDocument5 pagesPharmaceutical Excipientsmads56091No ratings yet
- Sciencedirect: Principles of Skills Assessment in Dialectical Behavior TherapyDocument12 pagesSciencedirect: Principles of Skills Assessment in Dialectical Behavior Therapysylvia_plath27No ratings yet