Download as ppt, pdf, or txt
You might also like
- FEMA Kitsap Risk ReportDocument47 pagesFEMA Kitsap Risk Reporttristan baurick67% (3)
- Nipple Reconstruction: Clinicsin Plastic SurgeryDocument7 pagesNipple Reconstruction: Clinicsin Plastic SurgeryJose Mauricio Suarez BecerraNo ratings yet
- Nipple ReconstructionDocument116 pagesNipple ReconstructionMaxim PekarevNo ratings yet
- A Step-by-Step Approach To A Successful Cosmetic Breast ReductionDocument3 pagesA Step-by-Step Approach To A Successful Cosmetic Breast ReductionMarco Antonio MiraveteNo ratings yet
- Lore's FasciaDocument7 pagesLore's FasciaR KNo ratings yet
- Internal MastopexyDocument7 pagesInternal MastopexyfumblefumbleNo ratings yet
- Evolution of Vertical Mammaplasty ReductionDocument15 pagesEvolution of Vertical Mammaplasty Reductionrandomaeiou7273No ratings yet
- Nipple Reconstruction FINALDocument39 pagesNipple Reconstruction FINALBarath Kumar SinghNo ratings yet
- Spiral FlapDocument20 pagesSpiral FlapDiolanda De AbreuNo ratings yet
- Bozola 2009Document7 pagesBozola 2009Mariangel HinojosaNo ratings yet
- Artigo Mastopexia Interna Dual PlaneDocument10 pagesArtigo Mastopexia Interna Dual PlaneanaalicearaNo ratings yet
- MastopexyDocument16 pagesMastopexyalinutza_childNo ratings yet
- Superior Pedicle Reduction Mammaplasty: Operative Strategies Operative StrategiesDocument7 pagesSuperior Pedicle Reduction Mammaplasty: Operative Strategies Operative StrategiesitsvamshikrishNo ratings yet
- MammoDocument58 pagesMammoNaresh GargNo ratings yet
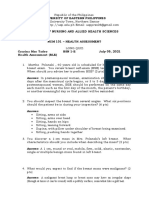
- Long Quiz NCM 101Document11 pagesLong Quiz NCM 101Czarina Mae Quinones TadeoNo ratings yet
- Four Flaps Technique For Neoumbilicoplasty: Young Taek Lee, Chan Kwon, Seung Chul Rhee, Sang Hun Cho, Su Rak EoDocument5 pagesFour Flaps Technique For Neoumbilicoplasty: Young Taek Lee, Chan Kwon, Seung Chul Rhee, Sang Hun Cho, Su Rak Eojuan carlos pradaNo ratings yet
- Jurnal Breast Rekon Presentasi 10 Okt 18 RevisiDocument57 pagesJurnal Breast Rekon Presentasi 10 Okt 18 RevisiFebriadi RNo ratings yet
- Extra Long Superior Pedicle For Gigantomastia ReductionDocument10 pagesExtra Long Superior Pedicle For Gigantomastia Reductionrandomaeiou7273No ratings yet
- Revision in Autologous Breast ReconstructionDocument24 pagesRevision in Autologous Breast ReconstructionJose Mauricio Suarez Becerra100% (1)
- Aysal-Sever2022 Article ANewTechniqueInCorrectionOfNipDocument7 pagesAysal-Sever2022 Article ANewTechniqueInCorrectionOfNipGöksuNo ratings yet
- Nur 146 RleDocument47 pagesNur 146 RleKeziah Marie Chua Santa-AnaNo ratings yet
- Updates in Aesthetic Surgery II 1112 Article.10Document14 pagesUpdates in Aesthetic Surgery II 1112 Article.10Hải Dương MinhNo ratings yet
- Creating Youthful UmbilicusDocument5 pagesCreating Youthful Umbilicusjuan carlos pradaNo ratings yet
- Otoplasty Surgical TechniqueDocument12 pagesOtoplasty Surgical TechniqueHNo ratings yet
- 10 1002@micr 30633Document6 pages10 1002@micr 30633carlosNo ratings yet
- Otoplasty Surgical TechniqueDocument12 pagesOtoplasty Surgical TechniqueLacramioaraBalanNo ratings yet
- Costochondral GraftsDocument5 pagesCostochondral Graftssmartdoc36100% (1)
- Breast ReconstructionDocument58 pagesBreast ReconstructionSumi TranNo ratings yet
- Necklift Fixation To Deep Cervical Fascia and HyoidDocument11 pagesNecklift Fixation To Deep Cervical Fascia and Hyoidrandomaeiou7273No ratings yet
- Breast Reconstruction With Free Anterolateral Thigh FlapDocument5 pagesBreast Reconstruction With Free Anterolateral Thigh Flapcusom34No ratings yet
- 122005secondary Nipple Reconstruction Using AlloDermDocument6 pages122005secondary Nipple Reconstruction Using AlloDermkomlanihou_890233161No ratings yet
- Scarless Reverse Umbilicoplasty A New Tech - 2019 - Journal of Plastic ReconDocument6 pagesScarless Reverse Umbilicoplasty A New Tech - 2019 - Journal of Plastic Reconjuan carlos pradaNo ratings yet
- BR 17102023Document19 pagesBR 17102023Maxi AbalosNo ratings yet
- Master Degree in Plastic Surgery ThesisDocument117 pagesMaster Degree in Plastic Surgery ThesisMohamed Ahmed El-RoubyNo ratings yet
- Breast Sonography: Gopal KhanalDocument96 pagesBreast Sonography: Gopal KhanalDr KhanNo ratings yet
- Capítulo 11 SerdevDocument19 pagesCapítulo 11 SerdevErik BrooksNo ratings yet
- Bille Et Al 2019Document5 pagesBille Et Al 2019Walid SasiNo ratings yet
- Vinit Rectus AbdominisDocument6 pagesVinit Rectus AbdominisVaneet KumarNo ratings yet
- Dual Plane Breast Augmentation: Optimizing Implant-Soft-Tissue Relationships in A Wide Range of Breast TypesDocument18 pagesDual Plane Breast Augmentation: Optimizing Implant-Soft-Tissue Relationships in A Wide Range of Breast TypesBeatriz BelottiNo ratings yet
- Hammond 2009Document9 pagesHammond 2009edkattaNo ratings yet
- 19-Mammography Positioning (FreeDownloadBooksForRadiographer)Document105 pages19-Mammography Positioning (FreeDownloadBooksForRadiographer)إسلام الجزيري100% (2)
- MRI MAmaDocument67 pagesMRI MAmaManuel Leonardo CaetanoNo ratings yet
- Intra-Capsular Versus Extra-Capsular Breast Mastopexy of Previously Augmented BreastDocument6 pagesIntra-Capsular Versus Extra-Capsular Breast Mastopexy of Previously Augmented BreastdiogenesNo ratings yet
- MastopexyDocument15 pagesMastopexyLuiggi FayadNo ratings yet
- Nipple-Areolar Complex ReconstructionDocument680 pagesNipple-Areolar Complex ReconstructionStephania Torres Pastrana y Rivera100% (3)
- Augmentasi Mammae & MastopexyDocument52 pagesAugmentasi Mammae & MastopexySitha ChristineNo ratings yet
- Management: 3rd Degree RepairDocument2 pagesManagement: 3rd Degree RepairBiway RegalaNo ratings yet
- 20-3-253 Giampapa 2000 Suturre Suspension Technique Offers PredictableDocument3 pages20-3-253 Giampapa 2000 Suturre Suspension Technique Offers PredictableGustavo MunizNo ratings yet
- Lejour Reduction MammoplastyDocument6 pagesLejour Reduction MammoplastyMiguelito JohnsonNo ratings yet
- A Classification and Algorithm For Treatment of Breast PtosisDocument9 pagesA Classification and Algorithm For Treatment of Breast PtosisreylaberintoNo ratings yet
- Sinmasta CorreccionDocument6 pagesSinmasta CorreccionEugenia KowriginNo ratings yet
- Ogawa2008 PDFDocument2 pagesOgawa2008 PDFsmansa123No ratings yet
- Inferior Pedicle Reduction Technique For Larger Forms of GynecomastiaDocument6 pagesInferior Pedicle Reduction Technique For Larger Forms of GynecomastiaΔρ Βαιος ΑγγελοπουλοςNo ratings yet
- Head and Neck Cancer - Reconstruction: HistoryDocument6 pagesHead and Neck Cancer - Reconstruction: HistorySri MahyantiNo ratings yet
- Breast Augmentation 2Document74 pagesBreast Augmentation 2Naveen SNo ratings yet
- Mammography PresentationDocument84 pagesMammography Presentationsarose bhandari67% (3)
- 04-B. Abnormal Labor - 2 PDFDocument4 pages04-B. Abnormal Labor - 2 PDFAyu Tien Thayibatudiniyah DaNo ratings yet
- SinulDocument38 pagesSinulCucos NataliaNo ratings yet
- SinulDocument86 pagesSinulCucos NataliaNo ratings yet
- David Lieberman Make Anyone LoyalDocument28 pagesDavid Lieberman Make Anyone Loyalnorman_osborn100% (2)
- Soc Di Term Paper K12Document25 pagesSoc Di Term Paper K12Labli Mercado100% (2)
- D.2 - Business Continuity Plan DocumentDocument35 pagesD.2 - Business Continuity Plan DocumentNikitasKladakis100% (1)
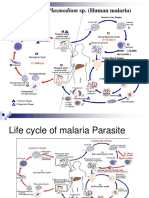
- The Life Cycle & The Transmission Dynamic Versi 1Document14 pagesThe Life Cycle & The Transmission Dynamic Versi 1rayNo ratings yet
- 1 - Cdi-7 Drug Education and Vice ControlDocument8 pages1 - Cdi-7 Drug Education and Vice ControlAnthony Ehapon100% (1)
- The Sensations ofDocument13 pagesThe Sensations ofLuisa duenasNo ratings yet
- Detailed System Design: 4.1. Use Case DiagramDocument4 pagesDetailed System Design: 4.1. Use Case DiagramammaraNo ratings yet
- Strengths (S) Weaknesses (W)Document3 pagesStrengths (S) Weaknesses (W)Daniela CoNo ratings yet
- Subsurface Sewage DisposalDocument174 pagesSubsurface Sewage DisposalSanthi KrishnaNo ratings yet
- Psychoanalysis and Psychodynamic TherapiesDocument51 pagesPsychoanalysis and Psychodynamic Therapieskuro hanabusaNo ratings yet
- Hon. Ramon Chito R. MendozaDocument6 pagesHon. Ramon Chito R. MendozaSweet SimyunnNo ratings yet
- Pengaruh Dosis Serbuk Biji Kelor (Moringa Oliefera) Terhadap Kadar Biochemical Oxygen Demand Air Limbah Rumah Pemotongan Ayam TAHUN 2021Document9 pagesPengaruh Dosis Serbuk Biji Kelor (Moringa Oliefera) Terhadap Kadar Biochemical Oxygen Demand Air Limbah Rumah Pemotongan Ayam TAHUN 2021meiliaNo ratings yet
- Management of Anastomotic Leakage After Rectal Surgery: A Review ArticleDocument9 pagesManagement of Anastomotic Leakage After Rectal Surgery: A Review ArticledrelvNo ratings yet
- Advance Notice Required To Increase Childcare Fees, Reply To Forum Letter, 19 Sep 2009Document2 pagesAdvance Notice Required To Increase Childcare Fees, Reply To Forum Letter, 19 Sep 2009dbmcysNo ratings yet
- CAD/CAM en Protesis Parcial FijaDocument13 pagesCAD/CAM en Protesis Parcial FijaodjhoselingNo ratings yet
- Aerial Lift TrainingDocument81 pagesAerial Lift TrainingCesar Augusto Vera JaimesNo ratings yet
- MSDS EthanolDocument13 pagesMSDS EthanolShahida Norizan100% (1)
- How The COVID-19 Epidemic Changed Working Conditions in FranceDocument4 pagesHow The COVID-19 Epidemic Changed Working Conditions in FranceRenata JapurNo ratings yet
- Pneumoperitoneum: Abdominal X-Rays Made Easy. 2nd Edition, James D. BeggDocument30 pagesPneumoperitoneum: Abdominal X-Rays Made Easy. 2nd Edition, James D. BeggFaizal AzizNo ratings yet
- Capstone Project SomervilleDocument6 pagesCapstone Project Somervilleapi-281112049No ratings yet
- Oet 2.0 Writing Practice and Exercises Book For Nurses Vol 2Document184 pagesOet 2.0 Writing Practice and Exercises Book For Nurses Vol 2Dandlers MurrayNo ratings yet
- Year 8 TimetablesDocument200 pagesYear 8 Timetableseverytaj617No ratings yet
- Top 5 Healthcare AI Startups To Watch For in 2021Document6 pagesTop 5 Healthcare AI Startups To Watch For in 2021appengine.ai100% (2)
- Jama Raj 2022 Po 220015 1652813400.47174Document2 pagesJama Raj 2022 Po 220015 1652813400.47174JNo ratings yet
- Post-Traumatic Frontal Mucocele Exceptional Cause and Frequent RecurrenceDocument3 pagesPost-Traumatic Frontal Mucocele Exceptional Cause and Frequent RecurrenceInternational Journal of Innovative Science and Research Technology100% (1)
- Speech Pathologists' Professional Identity in Response To Working With AssistantsDocument1 pageSpeech Pathologists' Professional Identity in Response To Working With AssistantsKaren DanielaNo ratings yet
- Centennial Vs QuiambaoDocument4 pagesCentennial Vs QuiambaoKornessa ParasNo ratings yet
- National Nutrition Strategy and Action PlanDocument97 pagesNational Nutrition Strategy and Action PlanBglpoo OfficerNo ratings yet
- Imediate Effect of Cold and Neutral Spinal Spray On Autonomic PDFDocument7 pagesImediate Effect of Cold and Neutral Spinal Spray On Autonomic PDFPrajwal G GowdaNo ratings yet