Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- How To Become A Pro Player at Cs 1.6Document5 pagesHow To Become A Pro Player at Cs 1.6john95_s100% (2)
- Notre Dame of Masiag, Inc.: What Formativ e Question S Shall Lead To The Completi On of Efaa? ToDocument2 pagesNotre Dame of Masiag, Inc.: What Formativ e Question S Shall Lead To The Completi On of Efaa? ToLANY T. CATAMINNo ratings yet
- Chapter 10: Virtual Memory: Silberschatz, Galvin and Gagne ©2018 Operating System Concepts - 10 EditionDocument85 pagesChapter 10: Virtual Memory: Silberschatz, Galvin and Gagne ©2018 Operating System Concepts - 10 EditionSuhaib masalhaNo ratings yet
- Gold ETFDocument11 pagesGold ETFPravin ChoughuleNo ratings yet
- The Pre-Production Process EvaluationDocument8 pagesThe Pre-Production Process EvaluationMC_Onnell100% (1)
- ASM Interview QuestionDocument14 pagesASM Interview QuestiondayascNo ratings yet
- Yealink Phone UserGuide PDFDocument2 pagesYealink Phone UserGuide PDFEric SmithNo ratings yet
- CS701 - Theory of Computation Assignment No.1: InstructionsDocument2 pagesCS701 - Theory of Computation Assignment No.1: InstructionsIhsanullah KhanNo ratings yet
- Commercial Paper: Presented by Dharani Dharan.m Vijaya Kumar S.BDocument16 pagesCommercial Paper: Presented by Dharani Dharan.m Vijaya Kumar S.Budaya37No ratings yet
- PetretecDocument8 pagesPetretecVenkatesan KrishnachariNo ratings yet
- Project On Trigonometry: Designed By:-Shubham Kumar 10 D Roll No: - 6Document36 pagesProject On Trigonometry: Designed By:-Shubham Kumar 10 D Roll No: - 6Surbhi Nagpal AhujaNo ratings yet
- Pregnancy-Related Pelvic Girdle Pain: Second Stage of LabourDocument4 pagesPregnancy-Related Pelvic Girdle Pain: Second Stage of LabourSravan Ganji100% (1)
- Cela NeseDocument1 pageCela NeseitskapilgargNo ratings yet
- Spa Music 10 SLM3 q1Document21 pagesSpa Music 10 SLM3 q1Noldan King FranciscoNo ratings yet
- Crypt Arithmatic Problem SolutionDocument10 pagesCrypt Arithmatic Problem SolutionHariom Patel100% (4)
- West Elm Digital CatalogueDocument131 pagesWest Elm Digital CatalogueogkanishkNo ratings yet
- Block 3Document17 pagesBlock 3Dianne ChristineNo ratings yet
- RFP Human Resource Management SystemDocument15 pagesRFP Human Resource Management SystemMd. Mofakker Morshed Khan ChowdhuryNo ratings yet
- Toad For OracleDocument1,157 pagesToad For OraclesatsriniNo ratings yet
- What Is Multilayer Fr4 PCB Substrate MaterialDocument10 pagesWhat Is Multilayer Fr4 PCB Substrate MaterialjackNo ratings yet
- ULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Document1 pageULTIMATE-CI-ST-090 - 2 Stages - Compact - SIEMENS - 1FL6044Francesco SchioppaNo ratings yet
- Bhopal Chapter of ISSS 1st NewsletterDocument8 pagesBhopal Chapter of ISSS 1st NewsletterBankesh ChatterjeeNo ratings yet
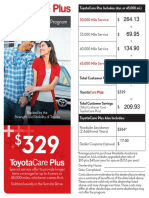
- ToyotaCare Plus CalculationDocument2 pagesToyotaCare Plus CalculationShao MaNo ratings yet
- Plug Valves To API 599Document11 pagesPlug Valves To API 599Marten HaneNo ratings yet
- Chapter 10 - Eco LiteracyDocument15 pagesChapter 10 - Eco LiteracyMichelle Bandoquillo100% (1)
- Arnold Schwarzenegger ThesisDocument4 pagesArnold Schwarzenegger Thesislanatedrummondfortwayne100% (2)
- 22 BÀI MẪU TASK 2 TỪ ĐỀ THI THẬT 2020 BY NGOCBACHDocument101 pages22 BÀI MẪU TASK 2 TỪ ĐỀ THI THẬT 2020 BY NGOCBACHCô TốngNo ratings yet
- Introduction To Econometrics Ii (Econ-3062) : Mohammed Adem (PHD)Document83 pagesIntroduction To Econometrics Ii (Econ-3062) : Mohammed Adem (PHD)ፍቅር እስከ መቃብር100% (2)
- Sunsynk Hybrid Inverter 3.6 5 UserManual v28 EnglishDocument81 pagesSunsynk Hybrid Inverter 3.6 5 UserManual v28 Englishprobeeriets6No ratings yet
- Upper Primary Division Competition Paper: ThursdayDocument10 pagesUpper Primary Division Competition Paper: ThursdayOlga Rudenko BradfordNo ratings yet