Download as ppt, pdf, or txt
You might also like
- Inernal Hernia (Recovered)Document26 pagesInernal Hernia (Recovered)Islam MagdyNo ratings yet
- Conservative Management of Perforated Peptic UlcerDocument4 pagesConservative Management of Perforated Peptic UlcerAfiani JannahNo ratings yet
- ComponentsDocument5 pagesComponentsprakashmathewNo ratings yet
- Lung AnatomyDocument19 pagesLung AnatomyScott Yee100% (2)
- Open Inguinal Hernia RepairDocument6 pagesOpen Inguinal Hernia RepairKris TejereroNo ratings yet
- Inguinal Hernias: CaseDocument6 pagesInguinal Hernias: Casechomz14No ratings yet
- Types of Hernia and Its ManagementDocument80 pagesTypes of Hernia and Its ManagementVisaagan Kalaithasan50% (2)
- Gastrointestinal System Block: Case 5ADocument9 pagesGastrointestinal System Block: Case 5ARonald ChrisbiantoNo ratings yet
- Intestinal Polyps and PolyposisDocument244 pagesIntestinal Polyps and PolyposisVladislav KotovNo ratings yet
- UCT Urology NotesDocument70 pagesUCT Urology NotesdrstaatsNo ratings yet
- Hérnias - Classificação NyhusDocument1 pageHérnias - Classificação NyhusgscapeNo ratings yet
- Clinical Surgery in General RCS Course ManualDocument2 pagesClinical Surgery in General RCS Course ManualsafiNo ratings yet
- Dr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliDocument25 pagesDr. Asif Mian Ansari DNB Resident Dept. of General Surgery Max Hospital, MohaliKarem Maali100% (1)
- Anal ProblemsDocument35 pagesAnal ProblemsSandip VaghelaNo ratings yet
- Vascular InjuryDocument85 pagesVascular InjuryWildaNo ratings yet
- Polyps and PolyposisDocument52 pagesPolyps and PolyposisorianattNo ratings yet
- Acute AbdomenDocument4 pagesAcute Abdomensarguss14No ratings yet
- Colon, Rectum and AnusDocument30 pagesColon, Rectum and AnusKiara GovenderNo ratings yet
- Combined Okell NotesDocument202 pagesCombined Okell Notessameeramw100% (5)
- Umbilical HerniaDocument1 pageUmbilical HerniaI Putu Adi Palguna100% (1)
- HerniaDocument11 pagesHerniaRizka JamaraNo ratings yet
- Turp 160328193838Document36 pagesTurp 160328193838Right VentricleNo ratings yet
- A System of Operative Surgery, Volume IV (of 4)From EverandA System of Operative Surgery, Volume IV (of 4)Rating: 4 out of 5 stars4/5 (1)
- Seminar 4Document49 pagesSeminar 4Yamuna SubramaniamNo ratings yet
- Drains in SurgeryDocument66 pagesDrains in SurgeryBalaji MallaNo ratings yet
- Vascular Presentation - Visceral Artery Aneurysms - MCGDocument22 pagesVascular Presentation - Visceral Artery Aneurysms - MCGYasir BouchiNo ratings yet
- Abdominal Trauma: Dr. Sri Indah Aruminingsih, SP - RadDocument135 pagesAbdominal Trauma: Dr. Sri Indah Aruminingsih, SP - RadwidyastutiNo ratings yet
- Intestinal Stomas PDFDocument10 pagesIntestinal Stomas PDFAmyandNo ratings yet
- Gall Stone Disease: DR M.farhad General SurgeonDocument56 pagesGall Stone Disease: DR M.farhad General SurgeondrelvNo ratings yet
- Techniques of Bowel Resection and AnastomosisDocument7 pagesTechniques of Bowel Resection and Anastomosisfaris nagib100% (1)
- Acute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHDocument45 pagesAcute Abdominal Pain: Associate Professor, Dept. of Surgery Mti, KMC, KTHWaleed MaboodNo ratings yet
- Acute Limb IschemiaDocument16 pagesAcute Limb IschemiaMohammad Husni BanisalmanNo ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- Rise of Modern Surgery OrigiDocument46 pagesRise of Modern Surgery OrigiPriyanka KaranamNo ratings yet
- Bile Duct InjuryDocument62 pagesBile Duct InjuryShashidhara Puttaraj100% (1)
- History of Surgery Oct 2016Document134 pagesHistory of Surgery Oct 2016Ahmed GendiaNo ratings yet
- Acute Pain Abdomen in Surgical PracticeDocument34 pagesAcute Pain Abdomen in Surgical PracticedrakashnardeNo ratings yet
- Melanoma: Meku Damtie (M.D.) July 18, 2006Document38 pagesMelanoma: Meku Damtie (M.D.) July 18, 2006Worku KifleNo ratings yet
- Acute Abdomen The "Black Hole" of MedicineDocument99 pagesAcute Abdomen The "Black Hole" of MedicinedebarajuNo ratings yet
- Preparing Severely Jaundiced Patient For SurgeryDocument2 pagesPreparing Severely Jaundiced Patient For Surgerylentini@maltanet.netNo ratings yet
- SURGERY Lecture 3 - Abdominal Hernia (Dr. Mendoza)Document12 pagesSURGERY Lecture 3 - Abdominal Hernia (Dr. Mendoza)Medisina101100% (1)
- Diagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020Document16 pagesDiagnosis, Treatment and Follow-Up in Extracranial Carotid Stenosis, 2020CAMILO ARMANDO BENAVIDES BURBANONo ratings yet
- SurgeryDocument13 pagesSurgerykarendelarosa06100% (2)
- Abdominal Surgery All in OneDocument50 pagesAbdominal Surgery All in OneAnne ChoyNo ratings yet
- Abdominal LumpDocument19 pagesAbdominal LumpDeepak AnNo ratings yet
- An Updated Review of Cystic Hepatic LesionsDocument8 pagesAn Updated Review of Cystic Hepatic LesionsMayerlin CalvacheNo ratings yet
- Abdominal Trauma RevisitedDocument11 pagesAbdominal Trauma Revisitedsanchez_polo_eNo ratings yet
- Vein Ligation and StrippingDocument4 pagesVein Ligation and StrippingNiken Feladita SantosoNo ratings yet
- Incisional Hernia RepairDocument6 pagesIncisional Hernia RepairLouis FortunatoNo ratings yet
- DiverticulitisDocument34 pagesDiverticulitisSahirNo ratings yet
- Gastrointestinal SurgeryDocument78 pagesGastrointestinal Surgeryjjmail100% (1)
- ANDI DR Louis Jordaan - 2Document9 pagesANDI DR Louis Jordaan - 2aprooolNo ratings yet
- AbscessDocument26 pagesAbscessThusith WijayawardenaNo ratings yet
- Slides 2 - Wounds, UlcersDocument80 pagesSlides 2 - Wounds, UlcersCWT2010No ratings yet
- ROJA RANI Abstract For PosterDocument4 pagesROJA RANI Abstract For Postersaikrishnamedico100% (1)
- Atlas of Gastrointestinal Endoscopy and Related PathologyDocument2 pagesAtlas of Gastrointestinal Endoscopy and Related PathologyMaria PatituNo ratings yet
- Abdominal Incisions: A Simple Guide For NursesDocument25 pagesAbdominal Incisions: A Simple Guide For Nursesfaris.surgeonNo ratings yet
- Carcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaDocument63 pagesCarcinoma Penis Management: Dr. Lilamani Rajthala MS Resident Moderator: Dr. Samir ShresthaBibek GhimireNo ratings yet
- Sudil Paudyal: 11/01/12 Abdomen Presentation by Sudil 1Document58 pagesSudil Paudyal: 11/01/12 Abdomen Presentation by Sudil 1Haba CristianNo ratings yet
- AbdWall, Hernia Atbp - AnnoDocument34 pagesAbdWall, Hernia Atbp - AnnoJuan Lorenzo RequironNo ratings yet
- HerniaDocument100 pagesHerniaangelaanapaku100% (3)
- Anatomy in Practice: The Sacrotuberous LigamentDocument4 pagesAnatomy in Practice: The Sacrotuberous LigamentAjay Pal NattNo ratings yet
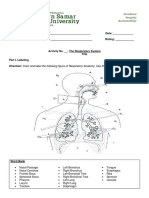
- The Respiratory System ActivityDocument4 pagesThe Respiratory System ActivityVina DiscarNo ratings yet
- Manual Muscle Test of Cervical SpineDocument4 pagesManual Muscle Test of Cervical SpineDr Ahmed NabilNo ratings yet
- Brochure Ultrasonograph y of The Live Ru 42 eDocument132 pagesBrochure Ultrasonograph y of The Live Ru 42 ealiceinwinterNo ratings yet
- Image Interpretation 4Document93 pagesImage Interpretation 4NanaJaeNo ratings yet
- 0443065640Document447 pages0443065640Helena Sopen-Luoma100% (5)
- Part 2 Anatomy and PhysiologyDocument8 pagesPart 2 Anatomy and Physiologyzy- SBGNo ratings yet
- Kolar 2014Document6 pagesKolar 2014Arnold Barra100% (1)
- Abdomen and Acute Abdominal SeriesDocument7 pagesAbdomen and Acute Abdominal SeriesLlv VidalNo ratings yet
- Diaphragmatic Breathing vs. Belly BreathingDocument8 pagesDiaphragmatic Breathing vs. Belly BreathingTatiana JosanNo ratings yet
- 4 Essential Strategies For The Correction of Anterior Pelvic TiltDocument10 pages4 Essential Strategies For The Correction of Anterior Pelvic TiltAlexander NarváezNo ratings yet
- Chest X Ray - BasicsDocument4 pagesChest X Ray - BasicsEd ChangNo ratings yet
- MCQs On GITDocument3 pagesMCQs On GITsamuel waiswaNo ratings yet
- Cazuri-ColoanapptDocument69 pagesCazuri-ColoanapptmiravoineaNo ratings yet
- Petit TriangleDocument4 pagesPetit TriangleSlim SaaryNo ratings yet
- Thorax ScriptDocument3 pagesThorax ScriptEspiritu, ChriscelNo ratings yet
- Anaphy Act 1Document2 pagesAnaphy Act 1TheaNo ratings yet
- 3P Power, Passage, Passenger: Amri Ashshiddieq 1 3 1 0 2 1 1 1 4 5Document14 pages3P Power, Passage, Passenger: Amri Ashshiddieq 1 3 1 0 2 1 1 1 4 5Amri AshshiddieqNo ratings yet
- Pneumo PeritoneumDocument14 pagesPneumo PeritoneumMuhammad Fikru RizalNo ratings yet
- Guide To Agni SaraDocument11 pagesGuide To Agni SaraEnoch Gandhislilbrother Abraham100% (1)
- Regional Le: Hip and Thigh: Fuerte-Felicano-Pasha Tabajonda-VillahermosaDocument176 pagesRegional Le: Hip and Thigh: Fuerte-Felicano-Pasha Tabajonda-VillahermosaOlenFuerte100% (1)
- Akut Abdomen: Divisi Bedah Digestif Bagian Ilmu Bedah Fk. Unair - SurabayaDocument24 pagesAkut Abdomen: Divisi Bedah Digestif Bagian Ilmu Bedah Fk. Unair - SurabayaYasdika ImamNo ratings yet
- Female Genitalia and RectumDocument3 pagesFemale Genitalia and Rectumadrian lozanoNo ratings yet
- Adobe Scan Jan 16, 2023Document15 pagesAdobe Scan Jan 16, 2023Juan HarshaNo ratings yet
- BBMS2004 L13 Respiratory System - Thoracic Cavity and Respiration 2022Document26 pagesBBMS2004 L13 Respiratory System - Thoracic Cavity and Respiration 2022JinyoungNo ratings yet
- PeritonioDocument5 pagesPeritonioSandro PinhoNo ratings yet
- Esophagus and StomachDocument33 pagesEsophagus and StomachIrfan Falah100% (1)
- Digestive ExamDocument13 pagesDigestive Examapi-294622133No ratings yet
- Lower Crossed SyndromeDocument5 pagesLower Crossed SyndromeD. HrmsNo ratings yet