Download as ppt, pdf, or txt
You might also like
- Modul Task: Tanisha Biaspal 0910714016Document5 pagesModul Task: Tanisha Biaspal 0910714016Bali PalNo ratings yet
- Ectopic Pregnancy PathophysiologyDocument5 pagesEctopic Pregnancy Pathophysiologyjoyrena ochondraNo ratings yet
- Family Planning: What Are The Advantages of A Contraceptive Injection?Document2 pagesFamily Planning: What Are The Advantages of A Contraceptive Injection?Adrian Clyde BautistaNo ratings yet
- Incomplete Abortion 1Document40 pagesIncomplete Abortion 1Denise FranciscoNo ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- StratOG Vaginal BreechDocument17 pagesStratOG Vaginal BreechNalin AbeysingheNo ratings yet
- Abnormal Uterine BleedingDocument5 pagesAbnormal Uterine Bleedingwuryan dewiNo ratings yet
- Acute Abdomen During Pregnancy BelaynehDocument47 pagesAcute Abdomen During Pregnancy BelaynehYohannis AsefaNo ratings yet
- Acute Uterine InversionDocument6 pagesAcute Uterine InversionBima GhovaroliyNo ratings yet
- Induction of Labor: Nor Fareshah BT Mohd Nasir 071303057 Batch 21/ F2Document47 pagesInduction of Labor: Nor Fareshah BT Mohd Nasir 071303057 Batch 21/ F2Nor Fareshah100% (1)
- Common Gynaecological Conditions Leading To Referral - 071118Document20 pagesCommon Gynaecological Conditions Leading To Referral - 071118zehra khowaja100% (1)
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- Anomalies of The Placenta and Umbilical CordDocument2 pagesAnomalies of The Placenta and Umbilical CordAyessa D. Rosalita100% (1)
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- Prom 1Document48 pagesProm 1Tesfahun TekleNo ratings yet
- Abnormal Vaginal BleedingDocument41 pagesAbnormal Vaginal BleedingmarkkerwinNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- Uterine FibroidsDocument47 pagesUterine FibroidsMoh Aldhy HusaintNo ratings yet
- Pelvic Inflammatory DiseaseDocument6 pagesPelvic Inflammatory DiseaseJoel Tito100% (1)
- Benign and Malignant Tumors of Female Genital TractDocument14 pagesBenign and Malignant Tumors of Female Genital TractDimitrios PapadopoulosNo ratings yet
- Ectopic Pregnancy1Document34 pagesEctopic Pregnancy1Kreshimaricon FurigayNo ratings yet
- Choriocarcinoma 11Document23 pagesChoriocarcinoma 11Fakhir HasanNo ratings yet
- Genital FistulaeDocument27 pagesGenital Fistulaeapi-3705046100% (1)
- Obs&Gyn MDC Q and ADocument36 pagesObs&Gyn MDC Q and ARufai Abdul WahabNo ratings yet
- Breast DiseasesDocument28 pagesBreast DiseasesLyk TiglaoNo ratings yet
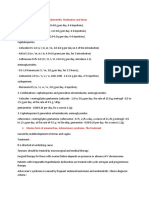
- Treatment of Acute Endometritis. Medication and DosesDocument3 pagesTreatment of Acute Endometritis. Medication and DosesTitoun LettounNo ratings yet
- Breech - Management Of: 1. PurposeDocument15 pagesBreech - Management Of: 1. PurposeMuathNo ratings yet
- Obstetric FistulaeDocument24 pagesObstetric FistulaenyangaraNo ratings yet
- 01embryology of Genitalia TawhariDocument10 pages01embryology of Genitalia TawhariMelissa Aina Mohd YusofNo ratings yet
- Abdul Hakeem Hady.: Done byDocument29 pagesAbdul Hakeem Hady.: Done byعمر احمد شاكرNo ratings yet
- Hypertensive Disorders in Pregnancy: Maisuri T. ChalidDocument44 pagesHypertensive Disorders in Pregnancy: Maisuri T. ChalidinhaNo ratings yet
- OSCE Revision OBG DocumentDocument60 pagesOSCE Revision OBG DocumentshreyaNo ratings yet
- Nancy E Fay MD Facog Division of Reproductive MedicineDocument32 pagesNancy E Fay MD Facog Division of Reproductive MedicineAdityo MulyonoNo ratings yet
- Essays For Obs N GYn 1Document8 pagesEssays For Obs N GYn 1whoosh2008No ratings yet
- Management of Pregnancy Related BleedingDocument75 pagesManagement of Pregnancy Related BleedingChuah Wei Hong100% (1)
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Hypertensive Disorders in Pregnancy (Williams 22 Edition)Document88 pagesHypertensive Disorders in Pregnancy (Williams 22 Edition)bagir_dm1067% (3)
- Mullarian AnomoliesDocument85 pagesMullarian AnomoliesPrathibha GuruguriNo ratings yet
- Obstetric Gynaecology Jan 11Document32 pagesObstetric Gynaecology Jan 11selvie87No ratings yet
- Heavy Menstrual BleedingDocument29 pagesHeavy Menstrual BleedingsanjupainNo ratings yet
- Identification and Management of Ambiguous GenitaliaDocument31 pagesIdentification and Management of Ambiguous Genitaliateslimolakunleraji100% (1)
- Obstetric ExaminationDocument4 pagesObstetric ExaminationSusan GeorgeNo ratings yet
- POP June 10,2021 1Document48 pagesPOP June 10,2021 1Kerod AbebeNo ratings yet
- Cesarean Section: Associate Professor Ph.D. E.A. EinyshDocument33 pagesCesarean Section: Associate Professor Ph.D. E.A. EinyshPrerit Aggarwal100% (1)
- Simposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1Document20 pagesSimposium 1 - Controversies - Dr. Teguh - HPV Vaccine Vs HPV Test-1isnayu drNo ratings yet
- Malignant Diseases of The CervixDocument128 pagesMalignant Diseases of The Cervixnicewan0% (1)
- Operative GynaecologyDocument59 pagesOperative GynaecologyArun Shree R0% (1)
- K16 - Pharmacology of Hormonal ContraceptionDocument51 pagesK16 - Pharmacology of Hormonal Contraceptiondhiyas100% (1)
- OSCE Gynae-OSCE-MMSSDocument24 pagesOSCE Gynae-OSCE-MMSSMohammad Saifullah100% (1)
- OSCE On 14/3/2008: Describe Gynaecoid PelvisDocument82 pagesOSCE On 14/3/2008: Describe Gynaecoid PelvisKahing LiNo ratings yet
- Printable - Thesis On Bishop ScoreDocument103 pagesPrintable - Thesis On Bishop Scoreanuaurv100% (3)
- Ectopic Pregnancy (Autosaved)Document56 pagesEctopic Pregnancy (Autosaved)susmita shresthaNo ratings yet
- Operative Vaginal Delivery PDFDocument56 pagesOperative Vaginal Delivery PDFFarehan Md Isa100% (1)
- Vesico Vaginal FistulaDocument6 pagesVesico Vaginal Fistulaapi-3705046No ratings yet
- Iugr & IufdDocument25 pagesIugr & IufdÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Anatomy Lec 22 (FGOs)Document49 pagesAnatomy Lec 22 (FGOs)Humraz100% (1)
- Gestational Trophoblastic Disease Pt2Document75 pagesGestational Trophoblastic Disease Pt2yurie_ameliaNo ratings yet
- 6-Post-Term PregnancyDocument5 pages6-Post-Term PregnancyOmar MohammedNo ratings yet
- InfertilityDocument14 pagesInfertilityDrChauhanNo ratings yet
- Obs & Gyne OSCE CasesDocument58 pagesObs & Gyne OSCE CasesMegan BolduanNo ratings yet
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 pagesMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreNo ratings yet
- Types of Female OrgasmDocument10 pagesTypes of Female Orgasmcarl1985100% (1)
- UQUMed 5 PAP SmearDocument19 pagesUQUMed 5 PAP SmearAHMED .KNo ratings yet
- 300+ Top Obstetrics and Gynecology Mcqs and Answers: Any Skill SearchDocument34 pages300+ Top Obstetrics and Gynecology Mcqs and Answers: Any Skill SearchARUSHI ARVIND100% (1)
- Science-10 Q3 Module-2 Week-2Document5 pagesScience-10 Q3 Module-2 Week-2Marl Rina EsperanzaNo ratings yet
- Reproductive System Concept MapDocument16 pagesReproductive System Concept MapQK CLARONo ratings yet
- Mammalian Reproductive SystemDocument50 pagesMammalian Reproductive SystemLeena MuniandyNo ratings yet
- Anfis Sistem Reproduksi Pria Dan WanitaDocument62 pagesAnfis Sistem Reproduksi Pria Dan WanitaLili HamdianaNo ratings yet
- Wa0030Document16 pagesWa0030DefaNo ratings yet
- Male PiercingsDocument12 pagesMale PiercingsLadyWillowlinnNo ratings yet
- Pene Palmeado Una Nueva ClasificacionDocument9 pagesPene Palmeado Una Nueva ClasificacionJorgy Ayala PinedaNo ratings yet
- Differentiation of Male and Female Sex and ClinicalDocument9 pagesDifferentiation of Male and Female Sex and ClinicalAKHIRUL SIREGARNo ratings yet
- Huerto, Kathrina B. - OvuviewDocument2 pagesHuerto, Kathrina B. - OvuviewKathrina Huerto100% (1)
- Ovarian Cysts Treatment & Management - Approach Considerations, Fetal and Neonatal Cysts, Ovarian Cysts in PregnancyDocument6 pagesOvarian Cysts Treatment & Management - Approach Considerations, Fetal and Neonatal Cysts, Ovarian Cysts in PregnancyTrần Hà TrangNo ratings yet
- Genital ProlapseDocument39 pagesGenital ProlapseFenias BoaneNo ratings yet
- Female Genital Organsangol2018Document37 pagesFemale Genital Organsangol2018Elizabeth GNo ratings yet
- Uterovaginal ProlapseDocument52 pagesUterovaginal ProlapseAmeera K Khan75% (4)
- Ovarian CystDocument2 pagesOvarian Cystf archiveNo ratings yet
- FinalDocument3 pagesFinalAnupam Saraf IINo ratings yet
- 10-OBGYN-Glory GroupDocument46 pages10-OBGYN-Glory Groupanmar alkhudhriNo ratings yet
- Intraoperative Complications After Total Laparoscopic Hysterectomy: A Retrospective Study in Training Institute Richa Patel, Arun MorayDocument5 pagesIntraoperative Complications After Total Laparoscopic Hysterectomy: A Retrospective Study in Training Institute Richa Patel, Arun MorayArun MorayNo ratings yet
- L1.3-GYNE-History - Physical Examination (Aug1822)Document2 pagesL1.3-GYNE-History - Physical Examination (Aug1822)Marc Lyndon CafinoNo ratings yet
- Artificial Reproductive Technologies: Zygote Intrafallopian Transfer (ZIFT) Is ADocument4 pagesArtificial Reproductive Technologies: Zygote Intrafallopian Transfer (ZIFT) Is AWarp RealityNo ratings yet
- OB RLE DC Instrument With ScaleDocument4 pagesOB RLE DC Instrument With ScaleCzarina Mae Quinones TadeoNo ratings yet
- Assisted Reproductive Technologies (ART) : Doaa HegabDocument23 pagesAssisted Reproductive Technologies (ART) : Doaa HegabLinguum100% (1)
- Science 10 LAS Quarter 3Document89 pagesScience 10 LAS Quarter 3Christopher John Natividad100% (3)
- 1341-Article Text-4651-2-10-20211223Document7 pages1341-Article Text-4651-2-10-20211223Alwiyah amd. kebNo ratings yet
- PCODDocument178 pagesPCODAbhishek Vijayakumar100% (1)