Download as ppt, pdf, or txt
You might also like
- CH 3.4-3.6 Meiosis Gizmo - StudentDocument11 pagesCH 3.4-3.6 Meiosis Gizmo - StudentKaylia SimmondsNo ratings yet
- Functions of PlacentaDocument18 pagesFunctions of PlacentaMohammad NabeelNo ratings yet
- Fertilization and Implantation Copy To StudentsDocument40 pagesFertilization and Implantation Copy To StudentsRiya SinghNo ratings yet
- Pregnancy - Human ReproductionDocument36 pagesPregnancy - Human ReproductionDICKSONNo ratings yet
- Physiology of Pregnancy & Functions of Placenta-1Document31 pagesPhysiology of Pregnancy & Functions of Placenta-1Ajit ShahNo ratings yet
- Fertilization, Pregnancy, and LactationDocument57 pagesFertilization, Pregnancy, and Lactationmega anggunNo ratings yet
- OvulationDocument31 pagesOvulationhacker ammerNo ratings yet
- Female Reproductive Ogans Internal Organs of ReproductionDocument22 pagesFemale Reproductive Ogans Internal Organs of ReproductionAngela NeriNo ratings yet
- Female Reproductive Ogans Internal Organs of ReproductionDocument22 pagesFemale Reproductive Ogans Internal Organs of ReproductionAecille VillarNo ratings yet
- Lecture 1physiology of PregnancyDocument42 pagesLecture 1physiology of PregnancyBlessie Zyren BasinangNo ratings yet
- Lecture 1physiology of PregnancyDocument58 pagesLecture 1physiology of PregnancyОлександра ЗагородняNo ratings yet
- Physiology of Pregnancy PDFDocument43 pagesPhysiology of Pregnancy PDFObsaNo ratings yet
- Menstrual Cycle:: MenarcheDocument21 pagesMenstrual Cycle:: MenarcheAlpesh PatelNo ratings yet
- Pregnancy 1Document70 pagesPregnancy 1Annapurna DangetiNo ratings yet
- 4. week ovulation, fertilization, implantation (١)Document41 pages4. week ovulation, fertilization, implantation (١)Maisy JohnNo ratings yet
- GA&E 13 - Fertilization & ImplantationDocument49 pagesGA&E 13 - Fertilization & ImplantationSu ZikaiNo ratings yet
- Fertilization, Pregnancy, and Fetal Development: Paul F. Terranova, PH.DDocument23 pagesFertilization, Pregnancy, and Fetal Development: Paul F. Terranova, PH.DChairul Nurdin AzaliNo ratings yet
- Placenta FunctionsDocument46 pagesPlacenta Functionsvenkata sryanamala50% (2)
- Physiology of PregnancyDocument27 pagesPhysiology of PregnancysabaNo ratings yet
- Embryology 2Document40 pagesEmbryology 2Sri Ram 07No ratings yet
- MCN Nursing 1Document107 pagesMCN Nursing 1Fau Fau DheoboNo ratings yet
- Fertilization, Pregnancy and Lactation: Dedi ArdinataDocument26 pagesFertilization, Pregnancy and Lactation: Dedi ArdinataHalseyNo ratings yet
- Chapter - 3 Human Reproduction - WatermarkDocument23 pagesChapter - 3 Human Reproduction - WatermarkDurgesh SainiNo ratings yet
- Human Reproduction.Document81 pagesHuman Reproduction.akulroy130507No ratings yet
- Anatomy and Physiology GCSDocument7 pagesAnatomy and Physiology GCSSherry Ann FayeNo ratings yet
- Chapter 29 - Development and Inheritance: ST ND RD STDocument5 pagesChapter 29 - Development and Inheritance: ST ND RD STtomorrow.today.yesterday .yesterdayNo ratings yet
- 1 ConceptionDocument104 pages1 ConceptionAnuchithraRKNo ratings yet
- Material Downloaded From SUPERCOPDocument10 pagesMaterial Downloaded From SUPERCOPkritika0% (1)
- The Growing FetusDocument62 pagesThe Growing Fetuscoosa liquorsNo ratings yet
- Prof. Dr. Çiğdem ElmasDocument49 pagesProf. Dr. Çiğdem ElmasMuhammet Fatih CantepeNo ratings yet
- Unit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityDocument62 pagesUnit 2 - Fertilization, Impantation, Development of Placenta and Its Function, AbnormalityN. Siva100% (1)
- Science 3rd QuarterDocument22 pagesScience 3rd QuarterBethel AquinoNo ratings yet
- Chapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusDocument8 pagesChapter 9: Nursing Care During Normal Pregnancy and Care of The Developing FetusAlyssaGrandeMontimor100% (1)
- Ferterlization and ImplantationDocument113 pagesFerterlization and Implantationmoreen kipkemoiNo ratings yet
- Reproduction NotesDocument27 pagesReproduction NotesAyra AlbairaNo ratings yet
- Placenta and Amniotic Fluid Structure FunctionDocument77 pagesPlacenta and Amniotic Fluid Structure FunctionZerica JohnNo ratings yet
- Placenta and Placental Hormones Lecture+PPT PDFDocument29 pagesPlacenta and Placental Hormones Lecture+PPT PDFPamela Marie Cope100% (1)
- Phases of Embryonic DevelopmentDocument9 pagesPhases of Embryonic DevelopmentIshu ChoudharyNo ratings yet
- Maternal and Child (Healthy Pregnancy)Document37 pagesMaternal and Child (Healthy Pregnancy)Lenny SucalditoNo ratings yet
- Conception and Diagnosis of Early PregnancyDocument48 pagesConception and Diagnosis of Early PregnancyjerrydanfordfxNo ratings yet
- Tutorial 4 Biology 2 Group 3 HN2Document3 pagesTutorial 4 Biology 2 Group 3 HN2Firdaus ZulkifliNo ratings yet
- 1.1c Implantation & Placental DevelopmentDocument5 pages1.1c Implantation & Placental DevelopmentBea Samonte100% (1)
- Review of Fetal DevelopmentDocument71 pagesReview of Fetal DevelopmentlisafelixNo ratings yet
- Charles Z. Ariola JR., MSN., LPT, Rn. Instructor IDocument22 pagesCharles Z. Ariola JR., MSN., LPT, Rn. Instructor ICharlz ZipaganNo ratings yet
- Lesson 5 - Structure and Functions of The Human PlacentaDocument4 pagesLesson 5 - Structure and Functions of The Human PlacentasununguraimasundaNo ratings yet
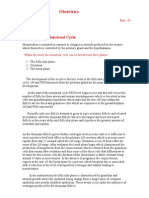
- Obstetrics: The Normal Menstrual CycleDocument4 pagesObstetrics: The Normal Menstrual Cycleapi-3829364No ratings yet
- Contraception S7 BDocument14 pagesContraception S7 BArsh KaiwanNo ratings yet
- Embryology Lecture Note 2Document19 pagesEmbryology Lecture Note 2jestreametefiaNo ratings yet
- Physiological Breast Development and Involution - CompressedDocument7 pagesPhysiological Breast Development and Involution - CompressedmohamedhazemelfollNo ratings yet
- Ovarian and Uterine Cycle - My PDocument23 pagesOvarian and Uterine Cycle - My PAzifah Zakaria100% (2)
- Bachelor of Science in Nursing: Care of Mother, Child and ADOLESCENT (Well Clients)Document7 pagesBachelor of Science in Nursing: Care of Mother, Child and ADOLESCENT (Well Clients)Big DaddyNo ratings yet
- Fertilization, Pregnancy, and Fetal Development: Paul F. Terranova, PH.DDocument23 pagesFertilization, Pregnancy, and Fetal Development: Paul F. Terranova, PH.DriswanfebriantoNo ratings yet
- Embryology - Fertilization: Paper 1 - Part BDocument5 pagesEmbryology - Fertilization: Paper 1 - Part BViswa GiriNo ratings yet
- Fertilization and Tubal FunctionsDocument35 pagesFertilization and Tubal Functionsv_vijayakanth7656No ratings yet
- Reproduction Part 2Document12 pagesReproduction Part 2Yuh moddaNo ratings yet
- Pregnancy N Lactation: Dr. Javaria LatifDocument41 pagesPregnancy N Lactation: Dr. Javaria LatifSyeda Naveen BatoolNo ratings yet
- Perkembangan Plasenta (Autosaved) .En - IdDocument18 pagesPerkembangan Plasenta (Autosaved) .En - IdFATIMAHNo ratings yet
- Pregnancy, Parturition, Breastfeeding - Physiology For Medical StudentsDocument34 pagesPregnancy, Parturition, Breastfeeding - Physiology For Medical StudentsLamy SNo ratings yet
- Good Afternoon: Prepared byDocument102 pagesGood Afternoon: Prepared byKrishna PatelNo ratings yet
- Physiology of Labor AND Lactation: Ermin Rachmawati, MDDocument37 pagesPhysiology of Labor AND Lactation: Ermin Rachmawati, MDAulia OlvianaNo ratings yet
- Planning and Organizing An Educational InstitutionDocument43 pagesPlanning and Organizing An Educational InstitutionjonyNo ratings yet
- Performance AppraisalDocument30 pagesPerformance AppraisaljonyNo ratings yet
- ObtertricDocument6 pagesObtertricjonyNo ratings yet
- Pilot StudyDocument8 pagesPilot Studyjony100% (1)
- CMCA ASSIGNMENT #1b PDFDocument3 pagesCMCA ASSIGNMENT #1b PDFAyanami PascuaNo ratings yet
- ReproductionDocument20 pagesReproductiontalon73256No ratings yet
- Bab 3 Keturunan Dan VariasiDocument13 pagesBab 3 Keturunan Dan VariasijaxsparrowNo ratings yet
- LP Menstrual CycleDocument3 pagesLP Menstrual CycleKaren Joy LendayaoNo ratings yet
- Anatomy of Normal PlacentaDocument8 pagesAnatomy of Normal Placentaareejk_94No ratings yet
- Cloning Human BeingsDocument310 pagesCloning Human BeingsThe Hastings CenterNo ratings yet
- Endocrinology of Genitourinary SystemDocument4 pagesEndocrinology of Genitourinary SystemGerardLumNo ratings yet
- Mechanisms of EvolutionDocument23 pagesMechanisms of EvolutionVeancy WangNo ratings yet
- Reproduction CLASS 10Document2 pagesReproduction CLASS 10Anushka ManatwalNo ratings yet
- Investigatory Infertility ProjectDocument16 pagesInvestigatory Infertility ProjectMahiNo ratings yet
- 2 Quarter Examination in Mapeh 8: Motiong National High SchoolDocument4 pages2 Quarter Examination in Mapeh 8: Motiong National High SchoolRJ GabuyaNo ratings yet
- Grade 8 Integrated Science Week 2 Lesson 2Document5 pagesGrade 8 Integrated Science Week 2 Lesson 2Balram HaroldNo ratings yet
- Vaginal MassDocument12 pagesVaginal MassShem DelolaNo ratings yet
- Induce Spawning of FishDocument17 pagesInduce Spawning of FishAli HamzaNo ratings yet
- CHAPTER 5 Microbial Growth Module BSED-ScienceDocument16 pagesCHAPTER 5 Microbial Growth Module BSED-ScienceXy-Za OlivaNo ratings yet
- The Essential Facts of FungusDocument2 pagesThe Essential Facts of FungusCantika Quita100% (2)
- Kendriya VidyalayaDocument10 pagesKendriya VidyalayaVanshNo ratings yet
- Study Material Simplified Biology Session 2023-24Document34 pagesStudy Material Simplified Biology Session 2023-24singhxraman00No ratings yet
- Reproduction and GeneticsDocument29 pagesReproduction and GeneticsDHEERAJ ADINo ratings yet
- Lecture On Biodiversity: Introduction To Environmental ScienceDocument70 pagesLecture On Biodiversity: Introduction To Environmental ScienceJubair SyedNo ratings yet
- CoturnixDocument24 pagesCoturnixrahul1809No ratings yet
- Biology Question BankDocument105 pagesBiology Question BankKeerthana D SNo ratings yet
- Test - IB Biology 3.3 - QuizletDocument6 pagesTest - IB Biology 3.3 - QuizletSumi VjNo ratings yet
- Aristotle S Generation of Animals On TheDocument25 pagesAristotle S Generation of Animals On TheDiana StroeNo ratings yet
- Completed Evolution Packet 2017-2018Document42 pagesCompleted Evolution Packet 2017-2018Talijah JamesNo ratings yet
- Plant Structure and FunctionDocument73 pagesPlant Structure and FunctionHIRA ALTEYA AYOPNo ratings yet
- Test Bank For Life 1st Edition PostlethwaitDocument15 pagesTest Bank For Life 1st Edition PostlethwaitBruce Faustini100% (38)
- MERRIE COT PPT-SCIE10-Roles of Hormones in Reproductive SystemDocument61 pagesMERRIE COT PPT-SCIE10-Roles of Hormones in Reproductive SystemMerrie Anne Pascual BagsicNo ratings yet
- Action PillDocument7 pagesAction Pillnajdah fakhirahNo ratings yet