
Modified-Release Dosage Forms and Drug Delevery Systems
Modified-Release Dosage Forms and Drug Delevery Systems
You might also like
- Solid Modified Release Dosage FormsDocument40 pagesSolid Modified Release Dosage FormsKristine Aubrey AlvarezNo ratings yet
- TabletsDocument174 pagesTabletsAhmed Ali100% (1)
- Indenx IP 2018 PDFDocument17 pagesIndenx IP 2018 PDFAkshay MongaNo ratings yet
- Phardose Lec Chapter 9Document3 pagesPhardose Lec Chapter 9Diah MarianoNo ratings yet
- Modified Release Dosage FormsDocument36 pagesModified Release Dosage FormsCHARLES RONALD GENATONo ratings yet
- Unit IV. Solid Modified Release Dosage FormsDocument24 pagesUnit IV. Solid Modified Release Dosage FormsMary-Ann Valencia SapnuNo ratings yet
- Modified Release Dosage FormsDocument29 pagesModified Release Dosage FormsMiham SsajnNo ratings yet
- Chapter 9Document66 pagesChapter 9Geline Anne BenozaNo ratings yet
- SOLID ORAL MODIFIED RELEASE LectureDocument13 pagesSOLID ORAL MODIFIED RELEASE LectureMa Rodelyn VivarNo ratings yet
- 201.controlled Release Oral Drug Delivery SystemDocument35 pages201.controlled Release Oral Drug Delivery SystemRajesh Akki0% (1)
- Phardose Lec Chapter 9Document11 pagesPhardose Lec Chapter 9megmayorNo ratings yet
- Dosage Forms 2Document91 pagesDosage Forms 2Palak BatraNo ratings yet
- Sustained ReleasedDocument25 pagesSustained ReleasedKhalid HussainNo ratings yet
- Drug Delivery SystemDocument23 pagesDrug Delivery SystemZafran KhanNo ratings yet
- 13 - Drug TargetingDocument61 pages13 - Drug TargetingBima AnestyaNo ratings yet
- Sustained-Controlled Release DDSDocument52 pagesSustained-Controlled Release DDSUsama NaushahiNo ratings yet
- Sustained ReleaseDocument59 pagesSustained ReleaseDipankar Sarkhel100% (1)
- Control Release G1Document35 pagesControl Release G1Victory ChinedumNo ratings yet
- Gastroretentive Drug Delivery SystemDocument33 pagesGastroretentive Drug Delivery SystemSaid Muhammad WazirNo ratings yet
- PHCT 302 SuppositoryDocument16 pagesPHCT 302 Suppositoryhardio damselgold.No ratings yet
- A Study of Dissolution Enhancement and Invitro Evaluation of RoxithromycinDocument6 pagesA Study of Dissolution Enhancement and Invitro Evaluation of Roxithromycinanto_pharma7784No ratings yet
- Concepts of Buccal Drug Delivery System: Bioadhesion and MucoadhesionDocument6 pagesConcepts of Buccal Drug Delivery System: Bioadhesion and Mucoadhesionpathuri rangaNo ratings yet
- Oral Controlled Release Drug Delivery SystemDocument59 pagesOral Controlled Release Drug Delivery SystemYanulia HandayaniNo ratings yet
- 12.floating NanoparticlesDocument5 pages12.floating NanoparticlesBaru Chandrasekhar RaoNo ratings yet
- Pharma Chapter 2_modDocument57 pagesPharma Chapter 2_modAlex CheungNo ratings yet
- 698 PDF PDFDocument8 pages698 PDF PDFMuh Indra SudirjaNo ratings yet
- Biopharmaceutics PPT, 20704002, Abhartireddy, FinalpptDocument37 pagesBiopharmaceutics PPT, 20704002, Abhartireddy, FinalpptBharti.Reddy ReddyNo ratings yet
- SRDDS Matrix TabletDocument17 pagesSRDDS Matrix TabletMISBAH KAUSARNo ratings yet
- Module 08Document7 pagesModule 08Dogbey AlbertNo ratings yet
- Gastro Retentive Drug Delivery SystemDocument20 pagesGastro Retentive Drug Delivery SystemokNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument27 pagesNew Microsoft Office PowerPoint PresentationGaini ChakravarthyNo ratings yet
- Chapter 9 - Solid Oral Modified-Release Dosage Forms PDFDocument7 pagesChapter 9 - Solid Oral Modified-Release Dosage Forms PDFRence Kier Sieth RubiasNo ratings yet
- MODIFIED RELEASE ORAL DRUG DELIVERY SummaryDocument7 pagesMODIFIED RELEASE ORAL DRUG DELIVERY Summarybenjelloun.boutayna2004No ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- GRDDS and EvaluationDocument54 pagesGRDDS and Evaluationgayatri maldhureNo ratings yet
- Extended Release Formulation: Available Online ThroughDocument60 pagesExtended Release Formulation: Available Online ThroughSomasundaram JeevanandhamNo ratings yet
- Advance Pharmaceutics Topic: Floating Drug Delivery System Group No. 10Document9 pagesAdvance Pharmaceutics Topic: Floating Drug Delivery System Group No. 10Noor ChwdriiNo ratings yet
- Modified Release Drug ProductsDocument4 pagesModified Release Drug ProductsHarshaNo ratings yet
- Lec 1 Industrial Pharmacy II 2023Document36 pagesLec 1 Industrial Pharmacy II 2023saifmohanad.usNo ratings yet
- Formulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochlorideDocument12 pagesFormulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochloridevbadsNo ratings yet
- Floating Tablets - Final With CorrectionDocument70 pagesFloating Tablets - Final With Correctionkharemix100% (1)
- Makalah Farmasetika Dasar MDRDocument10 pagesMakalah Farmasetika Dasar MDRWinda WindaNo ratings yet
- Suppositories and EnemasDocument35 pagesSuppositories and EnemasMr.ShazNo ratings yet
- GRH - 1aph - 1Document9 pagesGRH - 1aph - 1Grace HernandezNo ratings yet
- Modified Release Drug Delivery System AssignmentDocument13 pagesModified Release Drug Delivery System AssignmentArvi KhanNo ratings yet
- Tablet KompresiDocument9 pagesTablet KompresiRatuNo ratings yet
- NDDS AnswersDocument56 pagesNDDS AnswersPrajwal PatankarNo ratings yet
- Chapter 17. Modified-Release Drug Products Applied Biopharmaceutics & Pharmacokinetics, 6e AccessPharmacy McGraw Hill MediDocument1 pageChapter 17. Modified-Release Drug Products Applied Biopharmaceutics & Pharmacokinetics, 6e AccessPharmacy McGraw Hill Mediswr88kv5p2No ratings yet
- Gastro-Retentive Drug Delivery System: By: Mr. Lalit RanaDocument39 pagesGastro-Retentive Drug Delivery System: By: Mr. Lalit RanaShubham SrivastavaNo ratings yet
- 7-Drug Delivery Systems 3Document26 pages7-Drug Delivery Systems 3Ibrahim Al ShantiNo ratings yet
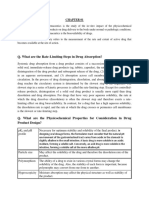
- Q. What Are The Rate-Limiting Steps in Drug Absorption?Document10 pagesQ. What Are The Rate-Limiting Steps in Drug Absorption?Arifur RahmanNo ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Zahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowDocument24 pagesZahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowQA Dhq OkaraNo ratings yet
- Modified Release Dosage FormsDocument50 pagesModified Release Dosage FormszedodansaNo ratings yet
- Group 3 FinalDocument30 pagesGroup 3 FinalKhara TeanoTanNo ratings yet
- ceutics 8-1-99Document99 pagesceutics 8-1-99gousepashaNo ratings yet
- Sustained Release Drug Delivery System - A ReviewDocument14 pagesSustained Release Drug Delivery System - A ReviewPranav PatelNo ratings yet
- Absorption by Jatin RatheeDocument47 pagesAbsorption by Jatin RatheeJatin RatheeNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Microneedle-mediated Transdermal and Intradermal Drug DeliveryFrom EverandMicroneedle-mediated Transdermal and Intradermal Drug DeliveryNo ratings yet
- Daftar Harga Sanbe EthicalDocument14 pagesDaftar Harga Sanbe EthicalOsbon SitumorangNo ratings yet
- Through Circulation Dryer: Used ForDocument4 pagesThrough Circulation Dryer: Used ForYosses Sang NahkodaNo ratings yet
- Betnesol InformationDocument6 pagesBetnesol InformationsmazNo ratings yet
- Kollidon CL Technical InformationDocument14 pagesKollidon CL Technical InformationhomarearisugawaNo ratings yet
- 1145E Rectal Preparations 2Document2 pages1145E Rectal Preparations 2Maja TashtanoskaNo ratings yet
- BP603T Unit 1-6 Lecturer's SlideDocument660 pagesBP603T Unit 1-6 Lecturer's SlideGyampoh SolomonNo ratings yet
- Chapter 79 - Pharmaceutical IndustryDocument20 pagesChapter 79 - Pharmaceutical IndustryarundhatiNo ratings yet
- Annual Product Quality ReviewDocument3 pagesAnnual Product Quality ReviewMITON CHOWDHURY100% (2)
- ST Report 11Document23 pagesST Report 11Niki PatelNo ratings yet
- 114 MCQs +Mid+Final PTech Syllabus-Merged-MergedDocument798 pages114 MCQs +Mid+Final PTech Syllabus-Merged-Mergedkamran.ghafoor.302100% (1)
- Daftar PustakaDocument6 pagesDaftar PustakaNadya Nur KusumoNo ratings yet
- Nppa Updated Price List of 216 Scheduled Formulations From 19.12.2022 To 06.01.2023.Document19 pagesNppa Updated Price List of 216 Scheduled Formulations From 19.12.2022 To 06.01.2023.redracer002No ratings yet
- Quantitative and Qualitative Analysis of Different Generic Paracetamol 500mg TabletDocument4 pagesQuantitative and Qualitative Analysis of Different Generic Paracetamol 500mg TabletEileen Eika Dela Cruz-LeeNo ratings yet
- Egc DehDocument8 pagesEgc DehNur Asni NurNo ratings yet
- AlbendazoleDocument7 pagesAlbendazoleSami SamiNo ratings yet
- Ads Opadry II Coat MoistDocument5 pagesAds Opadry II Coat MoistRani YundaNo ratings yet
- Industrial Pharmaceutical Tecnology: (Essentials)Document44 pagesIndustrial Pharmaceutical Tecnology: (Essentials)Selvakumar MuthumanickamNo ratings yet
- Dissolution Testing of Bilayer TabletsDocument10 pagesDissolution Testing of Bilayer TabletsAmjad KhanNo ratings yet
- Drug Registration Guidance Document DRGD Second Edition Revised January 2019Document693 pagesDrug Registration Guidance Document DRGD Second Edition Revised January 2019ฺฺฺBBB.AAANo ratings yet
- Applications of X-Ray Powder Diffraction in The Pharmaceutical IndustryDocument14 pagesApplications of X-Ray Powder Diffraction in The Pharmaceutical IndustryrafispereiraNo ratings yet
- Senarai Produk Yang Diluluskan Dalam PBKD385 8 JUN 2023 WebsiteDocument20 pagesSenarai Produk Yang Diluluskan Dalam PBKD385 8 JUN 2023 WebsiteasmawieandifazliNo ratings yet
- Starch 1500 - Sta-Rx 1500 (p.691-694) 720-723 PDFDocument4 pagesStarch 1500 - Sta-Rx 1500 (p.691-694) 720-723 PDFMarsha Fendria PrastikaNo ratings yet
- Essential Medicines List 2020Document67 pagesEssential Medicines List 2020Eman ShalabyNo ratings yet
- Nepal Pharmacy Council License Preparation Model Questions AllDocument209 pagesNepal Pharmacy Council License Preparation Model Questions AllSonu YdvNo ratings yet
- Montelukast MedicineDocument4 pagesMontelukast MedicineAman ChoudharyNo ratings yet
- TJPS 19 153Document8 pagesTJPS 19 153Korsa SandrinaNo ratings yet
- Osmotic Drug Delivery SystemDocument51 pagesOsmotic Drug Delivery Systemanburajj100% (1)
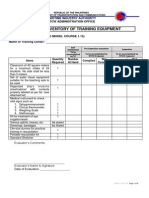
- Form 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDocument9 pagesForm 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDemp AlmiranezNo ratings yet
- Floating Tablets of FamotidineDocument8 pagesFloating Tablets of FamotidineRomah Cliquers LelledNo ratings yet
























































































Download as ppt, pdf, or txt
You might also like
- Solid Modified Release Dosage FormsDocument40 pagesSolid Modified Release Dosage FormsKristine Aubrey AlvarezNo ratings yet
- TabletsDocument174 pagesTabletsAhmed Ali100% (1)
- Indenx IP 2018 PDFDocument17 pagesIndenx IP 2018 PDFAkshay MongaNo ratings yet
- Phardose Lec Chapter 9Document3 pagesPhardose Lec Chapter 9Diah MarianoNo ratings yet
- Modified Release Dosage FormsDocument36 pagesModified Release Dosage FormsCHARLES RONALD GENATONo ratings yet
- Unit IV. Solid Modified Release Dosage FormsDocument24 pagesUnit IV. Solid Modified Release Dosage FormsMary-Ann Valencia SapnuNo ratings yet
- Modified Release Dosage FormsDocument29 pagesModified Release Dosage FormsMiham SsajnNo ratings yet
- Chapter 9Document66 pagesChapter 9Geline Anne BenozaNo ratings yet
- SOLID ORAL MODIFIED RELEASE LectureDocument13 pagesSOLID ORAL MODIFIED RELEASE LectureMa Rodelyn VivarNo ratings yet
- 201.controlled Release Oral Drug Delivery SystemDocument35 pages201.controlled Release Oral Drug Delivery SystemRajesh Akki0% (1)
- Phardose Lec Chapter 9Document11 pagesPhardose Lec Chapter 9megmayorNo ratings yet
- Dosage Forms 2Document91 pagesDosage Forms 2Palak BatraNo ratings yet
- Sustained ReleasedDocument25 pagesSustained ReleasedKhalid HussainNo ratings yet
- Drug Delivery SystemDocument23 pagesDrug Delivery SystemZafran KhanNo ratings yet
- 13 - Drug TargetingDocument61 pages13 - Drug TargetingBima AnestyaNo ratings yet
- Sustained-Controlled Release DDSDocument52 pagesSustained-Controlled Release DDSUsama NaushahiNo ratings yet
- Sustained ReleaseDocument59 pagesSustained ReleaseDipankar Sarkhel100% (1)
- Control Release G1Document35 pagesControl Release G1Victory ChinedumNo ratings yet
- Gastroretentive Drug Delivery SystemDocument33 pagesGastroretentive Drug Delivery SystemSaid Muhammad WazirNo ratings yet
- PHCT 302 SuppositoryDocument16 pagesPHCT 302 Suppositoryhardio damselgold.No ratings yet
- A Study of Dissolution Enhancement and Invitro Evaluation of RoxithromycinDocument6 pagesA Study of Dissolution Enhancement and Invitro Evaluation of Roxithromycinanto_pharma7784No ratings yet
- Concepts of Buccal Drug Delivery System: Bioadhesion and MucoadhesionDocument6 pagesConcepts of Buccal Drug Delivery System: Bioadhesion and Mucoadhesionpathuri rangaNo ratings yet
- Oral Controlled Release Drug Delivery SystemDocument59 pagesOral Controlled Release Drug Delivery SystemYanulia HandayaniNo ratings yet
- 12.floating NanoparticlesDocument5 pages12.floating NanoparticlesBaru Chandrasekhar RaoNo ratings yet
- Pharma Chapter 2_modDocument57 pagesPharma Chapter 2_modAlex CheungNo ratings yet
- 698 PDF PDFDocument8 pages698 PDF PDFMuh Indra SudirjaNo ratings yet
- Biopharmaceutics PPT, 20704002, Abhartireddy, FinalpptDocument37 pagesBiopharmaceutics PPT, 20704002, Abhartireddy, FinalpptBharti.Reddy ReddyNo ratings yet
- SRDDS Matrix TabletDocument17 pagesSRDDS Matrix TabletMISBAH KAUSARNo ratings yet
- Module 08Document7 pagesModule 08Dogbey AlbertNo ratings yet
- Gastro Retentive Drug Delivery SystemDocument20 pagesGastro Retentive Drug Delivery SystemokNo ratings yet
- New Microsoft Office PowerPoint PresentationDocument27 pagesNew Microsoft Office PowerPoint PresentationGaini ChakravarthyNo ratings yet
- Chapter 9 - Solid Oral Modified-Release Dosage Forms PDFDocument7 pagesChapter 9 - Solid Oral Modified-Release Dosage Forms PDFRence Kier Sieth RubiasNo ratings yet
- MODIFIED RELEASE ORAL DRUG DELIVERY SummaryDocument7 pagesMODIFIED RELEASE ORAL DRUG DELIVERY Summarybenjelloun.boutayna2004No ratings yet
- A Prolonged Release Parenteral Drug Delivery SystemDocument11 pagesA Prolonged Release Parenteral Drug Delivery SystemronnymcmNo ratings yet
- GRDDS and EvaluationDocument54 pagesGRDDS and Evaluationgayatri maldhureNo ratings yet
- Extended Release Formulation: Available Online ThroughDocument60 pagesExtended Release Formulation: Available Online ThroughSomasundaram JeevanandhamNo ratings yet
- Advance Pharmaceutics Topic: Floating Drug Delivery System Group No. 10Document9 pagesAdvance Pharmaceutics Topic: Floating Drug Delivery System Group No. 10Noor ChwdriiNo ratings yet
- Modified Release Drug ProductsDocument4 pagesModified Release Drug ProductsHarshaNo ratings yet
- Lec 1 Industrial Pharmacy II 2023Document36 pagesLec 1 Industrial Pharmacy II 2023saifmohanad.usNo ratings yet
- Formulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochlorideDocument12 pagesFormulation and Evaluation of Multiunit Pellet System of Venlafaxine HydrochloridevbadsNo ratings yet
- Floating Tablets - Final With CorrectionDocument70 pagesFloating Tablets - Final With Correctionkharemix100% (1)
- Makalah Farmasetika Dasar MDRDocument10 pagesMakalah Farmasetika Dasar MDRWinda WindaNo ratings yet
- Suppositories and EnemasDocument35 pagesSuppositories and EnemasMr.ShazNo ratings yet
- GRH - 1aph - 1Document9 pagesGRH - 1aph - 1Grace HernandezNo ratings yet
- Modified Release Drug Delivery System AssignmentDocument13 pagesModified Release Drug Delivery System AssignmentArvi KhanNo ratings yet
- Tablet KompresiDocument9 pagesTablet KompresiRatuNo ratings yet
- NDDS AnswersDocument56 pagesNDDS AnswersPrajwal PatankarNo ratings yet
- Chapter 17. Modified-Release Drug Products Applied Biopharmaceutics & Pharmacokinetics, 6e AccessPharmacy McGraw Hill MediDocument1 pageChapter 17. Modified-Release Drug Products Applied Biopharmaceutics & Pharmacokinetics, 6e AccessPharmacy McGraw Hill Mediswr88kv5p2No ratings yet
- Gastro-Retentive Drug Delivery System: By: Mr. Lalit RanaDocument39 pagesGastro-Retentive Drug Delivery System: By: Mr. Lalit RanaShubham SrivastavaNo ratings yet
- 7-Drug Delivery Systems 3Document26 pages7-Drug Delivery Systems 3Ibrahim Al ShantiNo ratings yet
- Q. What Are The Rate-Limiting Steps in Drug Absorption?Document10 pagesQ. What Are The Rate-Limiting Steps in Drug Absorption?Arifur RahmanNo ratings yet
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- Zahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowDocument24 pagesZahid Husain M.Pharm (Pharmaceutics) Faculty of Pharmacy, IU, LucknowQA Dhq OkaraNo ratings yet
- Modified Release Dosage FormsDocument50 pagesModified Release Dosage FormszedodansaNo ratings yet
- Group 3 FinalDocument30 pagesGroup 3 FinalKhara TeanoTanNo ratings yet
- ceutics 8-1-99Document99 pagesceutics 8-1-99gousepashaNo ratings yet
- Sustained Release Drug Delivery System - A ReviewDocument14 pagesSustained Release Drug Delivery System - A ReviewPranav PatelNo ratings yet
- Absorption by Jatin RatheeDocument47 pagesAbsorption by Jatin RatheeJatin RatheeNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Microneedle-mediated Transdermal and Intradermal Drug DeliveryFrom EverandMicroneedle-mediated Transdermal and Intradermal Drug DeliveryNo ratings yet
- Daftar Harga Sanbe EthicalDocument14 pagesDaftar Harga Sanbe EthicalOsbon SitumorangNo ratings yet
- Through Circulation Dryer: Used ForDocument4 pagesThrough Circulation Dryer: Used ForYosses Sang NahkodaNo ratings yet
- Betnesol InformationDocument6 pagesBetnesol InformationsmazNo ratings yet
- Kollidon CL Technical InformationDocument14 pagesKollidon CL Technical InformationhomarearisugawaNo ratings yet
- 1145E Rectal Preparations 2Document2 pages1145E Rectal Preparations 2Maja TashtanoskaNo ratings yet
- BP603T Unit 1-6 Lecturer's SlideDocument660 pagesBP603T Unit 1-6 Lecturer's SlideGyampoh SolomonNo ratings yet
- Chapter 79 - Pharmaceutical IndustryDocument20 pagesChapter 79 - Pharmaceutical IndustryarundhatiNo ratings yet
- Annual Product Quality ReviewDocument3 pagesAnnual Product Quality ReviewMITON CHOWDHURY100% (2)
- ST Report 11Document23 pagesST Report 11Niki PatelNo ratings yet
- 114 MCQs +Mid+Final PTech Syllabus-Merged-MergedDocument798 pages114 MCQs +Mid+Final PTech Syllabus-Merged-Mergedkamran.ghafoor.302100% (1)
- Daftar PustakaDocument6 pagesDaftar PustakaNadya Nur KusumoNo ratings yet
- Nppa Updated Price List of 216 Scheduled Formulations From 19.12.2022 To 06.01.2023.Document19 pagesNppa Updated Price List of 216 Scheduled Formulations From 19.12.2022 To 06.01.2023.redracer002No ratings yet
- Quantitative and Qualitative Analysis of Different Generic Paracetamol 500mg TabletDocument4 pagesQuantitative and Qualitative Analysis of Different Generic Paracetamol 500mg TabletEileen Eika Dela Cruz-LeeNo ratings yet
- Egc DehDocument8 pagesEgc DehNur Asni NurNo ratings yet
- AlbendazoleDocument7 pagesAlbendazoleSami SamiNo ratings yet
- Ads Opadry II Coat MoistDocument5 pagesAds Opadry II Coat MoistRani YundaNo ratings yet
- Industrial Pharmaceutical Tecnology: (Essentials)Document44 pagesIndustrial Pharmaceutical Tecnology: (Essentials)Selvakumar MuthumanickamNo ratings yet
- Dissolution Testing of Bilayer TabletsDocument10 pagesDissolution Testing of Bilayer TabletsAmjad KhanNo ratings yet
- Drug Registration Guidance Document DRGD Second Edition Revised January 2019Document693 pagesDrug Registration Guidance Document DRGD Second Edition Revised January 2019ฺฺฺBBB.AAANo ratings yet
- Applications of X-Ray Powder Diffraction in The Pharmaceutical IndustryDocument14 pagesApplications of X-Ray Powder Diffraction in The Pharmaceutical IndustryrafispereiraNo ratings yet
- Senarai Produk Yang Diluluskan Dalam PBKD385 8 JUN 2023 WebsiteDocument20 pagesSenarai Produk Yang Diluluskan Dalam PBKD385 8 JUN 2023 WebsiteasmawieandifazliNo ratings yet
- Starch 1500 - Sta-Rx 1500 (p.691-694) 720-723 PDFDocument4 pagesStarch 1500 - Sta-Rx 1500 (p.691-694) 720-723 PDFMarsha Fendria PrastikaNo ratings yet
- Essential Medicines List 2020Document67 pagesEssential Medicines List 2020Eman ShalabyNo ratings yet
- Nepal Pharmacy Council License Preparation Model Questions AllDocument209 pagesNepal Pharmacy Council License Preparation Model Questions AllSonu YdvNo ratings yet
- Montelukast MedicineDocument4 pagesMontelukast MedicineAman ChoudharyNo ratings yet
- TJPS 19 153Document8 pagesTJPS 19 153Korsa SandrinaNo ratings yet
- Osmotic Drug Delivery SystemDocument51 pagesOsmotic Drug Delivery Systemanburajj100% (1)
- Form 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDocument9 pagesForm 2B: Inventory of Training Equipment: Maritime Industry Authority STCW Administration OfficeDemp AlmiranezNo ratings yet
- Floating Tablets of FamotidineDocument8 pagesFloating Tablets of FamotidineRomah Cliquers LelledNo ratings yet