Download as pptx, pdf, or txt
You might also like
- Postpartum HemorrhageDocument5 pagesPostpartum Hemorrhageapi-354418387No ratings yet
- MALNUTRITIONDocument23 pagesMALNUTRITIONPrincess Alane MorenoNo ratings yet
- Botswana NnyepiDocument19 pagesBotswana NnyepiBang BojesNo ratings yet
- Vocabulary of English For NursingDocument37 pagesVocabulary of English For Nursingkelvin BinhNo ratings yet
- Malnutrition: FatimaDocument25 pagesMalnutrition: FatimaFatima Jamshaid100% (2)
- Syllogistic Rules and Syllogistic FallaciesDocument4 pagesSyllogistic Rules and Syllogistic FallaciesJel Yn Ne0% (1)
- Promoting Healthy Diets: Nutrition Officer IV Nutrition Information and Education Division National Nutrition CouncilDocument72 pagesPromoting Healthy Diets: Nutrition Officer IV Nutrition Information and Education Division National Nutrition CouncilHydra Olivar - Pantilgan100% (1)
- Nutrition Chapter 1-5Document49 pagesNutrition Chapter 1-5Maria MarieNo ratings yet
- ECOLOGY Let ReviewDocument26 pagesECOLOGY Let ReviewDonn SabalNo ratings yet
- Micronutrient Deficiency Among FilipinosDocument20 pagesMicronutrient Deficiency Among FilipinosAlnyssa Cornell100% (1)
- Child and AdolescenceDocument22 pagesChild and Adolescencejungkook'sNo ratings yet
- Biochemical Markers For Clinical Monitoring of Tissue PerfusionDocument14 pagesBiochemical Markers For Clinical Monitoring of Tissue PerfusionTrọng MPNo ratings yet
- Bandwagon Fallacy: ExamplesDocument8 pagesBandwagon Fallacy: ExamplesEliasNo ratings yet
- Grade 12 Biology Module1Document86 pagesGrade 12 Biology Module1Gabbie CruzNo ratings yet
- Postpartum LectureDocument64 pagesPostpartum LectureStephen Gabriel TitoNo ratings yet
- GDM PDFDocument20 pagesGDM PDFAnn Michelle TarrobagoNo ratings yet
- Ineffectve NCP PediaDocument1 pageIneffectve NCP PediaKarlo ReyesNo ratings yet
- MalnutritionDocument12 pagesMalnutritionSi R100% (1)
- Family Case Study GarciaJ Khate Zaira SDocument7 pagesFamily Case Study GarciaJ Khate Zaira Salbert delos santosNo ratings yet
- Normal Pregnancy: Dr. Achala Sahai SharmaDocument25 pagesNormal Pregnancy: Dr. Achala Sahai Sharmaachala sahaiNo ratings yet
- Food PyramidDocument2 pagesFood PyramidAubrey Ann FolloscoNo ratings yet
- Physical Examination and Review of Systems: Patient's Name / Room No. - 1Document3 pagesPhysical Examination and Review of Systems: Patient's Name / Room No. - 1Raf DalidigNo ratings yet
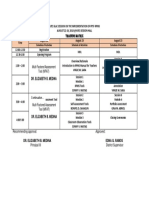
- Training Matrix: Schedule of Activities Schedule of Activities Schedule of ActivitiesDocument1 pageTraining Matrix: Schedule of Activities Schedule of Activities Schedule of ActivitiesSonny Matias100% (1)
- Power Point in Teaching StratDocument26 pagesPower Point in Teaching StratbabyanangNo ratings yet
- Effects of Leguminous Plants (Centrosema Pubescens) As Feed Additive For Growth Stimulation On BroilersDocument4 pagesEffects of Leguminous Plants (Centrosema Pubescens) As Feed Additive For Growth Stimulation On BroilersChern YuanNo ratings yet
- CHN1 LP 2 QuianoDocument27 pagesCHN1 LP 2 QuianoMargarette GeresNo ratings yet
- Stem Cell technology-PROS-CONSDocument2 pagesStem Cell technology-PROS-CONSjpmNo ratings yet
- Diltiazem Hydro ChlorideDocument3 pagesDiltiazem Hydro Chlorideapi-3797941100% (1)
- FOOD Pyramid What Is A Food Pyramid?Document9 pagesFOOD Pyramid What Is A Food Pyramid?Saadia TariqNo ratings yet
- Cmca at RiskDocument11 pagesCmca at RiskAyanami PascuaNo ratings yet
- IDNTv4 CaseStudy-OutptDocument8 pagesIDNTv4 CaseStudy-OutptMr.GoneNo ratings yet
- Basic Body Mechanics Moving & Positioning: Nursing 114A Care of The Older AdultsDocument44 pagesBasic Body Mechanics Moving & Positioning: Nursing 114A Care of The Older AdultsJonalyn EtongNo ratings yet
- Seminar LeadershipDocument72 pagesSeminar LeadershipKavi rajputNo ratings yet
- 24 Hour Diet RecallDocument1 page24 Hour Diet Recallapi-289747837No ratings yet
- Reflective Journal TemplateDocument4 pagesReflective Journal TemplateKey Ann Macatol GaliciaNo ratings yet
- 3 OB 1 - Hypertensive DisordersDocument5 pages3 OB 1 - Hypertensive DisordersIrene FranzNo ratings yet
- Reorganization of DOHDocument9 pagesReorganization of DOHHikariNo ratings yet
- Polycystic Ovarian Syndrome (PCOS)Document119 pagesPolycystic Ovarian Syndrome (PCOS)Jasani JayrajNo ratings yet
- NGT Ogt FeedingDocument3 pagesNGT Ogt FeedingDARWIN JAY SANG-ANNo ratings yet
- Differentiating Malnutrition Screening and Assessment A Nutrition Care Process PerspectiveDocument5 pagesDifferentiating Malnutrition Screening and Assessment A Nutrition Care Process Perspectivemariosan81No ratings yet
- A S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildDocument56 pagesA S P E N Clinical Guidelines - Nutrition Support of The Critically Ill ChildPaulina Kristiani BangunNo ratings yet
- Productivity Study Patient Tray LineDocument7 pagesProductivity Study Patient Tray Lineapi-451418701No ratings yet
- CircumcisionDocument4 pagesCircumcisionFernando Ribeiro JúniorNo ratings yet
- Megaloblastic AnaemiaDocument14 pagesMegaloblastic AnaemiaDaniel OnyenucheyaNo ratings yet
- NCP Gestational HypertensionDocument3 pagesNCP Gestational HypertensionCameron De GuzmanNo ratings yet
- Types of DietDocument1 pageTypes of DietNathalee WalkerNo ratings yet
- Group 7 Statement Agreed ToDocument3 pagesGroup 7 Statement Agreed ToShane TabunggaoNo ratings yet
- Maternal and Child Health NursingDocument6 pagesMaternal and Child Health NursingRoanne DivinagraciaNo ratings yet
- Nutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineDocument26 pagesNutrition Program: Common Nutritional Deficiencies 1. Vitamin A 2. Iron 3. IodineKyla OcampoNo ratings yet
- Hes 005 Session 14sasDocument8 pagesHes 005 Session 14sasJose Melmar Autida AutenticoNo ratings yet
- Kinds of SyllogismsDocument4 pagesKinds of Syllogismsinah_3050% (2)
- Fats & LipidsDocument32 pagesFats & LipidsSUNNY YADAVNo ratings yet
- Lesson 3: Vitamins For LifeDocument16 pagesLesson 3: Vitamins For LifeJo-Ann Santiago PadillaNo ratings yet
- Diet Computation Diet Prescription and Meal Planning NCM 105Document4 pagesDiet Computation Diet Prescription and Meal Planning NCM 105issaiahnicolleNo ratings yet
- Bioethics CH4Document26 pagesBioethics CH4AnimeOtaku GirlNo ratings yet
- Malnutrition Morris Adams MDocument31 pagesMalnutrition Morris Adams Mokwadha simionNo ratings yet
- CAJA, RENZO GABRIEL, BSN 2-1 NCM109-Midterm ModuleDocument14 pagesCAJA, RENZO GABRIEL, BSN 2-1 NCM109-Midterm ModuleRenzo GabrielNo ratings yet
- Physiologic and Psychologic Changes in PregnancyDocument41 pagesPhysiologic and Psychologic Changes in PregnancyAlessandra Franchesca CortezNo ratings yet
- Presented By: Anlet Jasmine T.M: Protein-Energy MalnutritionDocument24 pagesPresented By: Anlet Jasmine T.M: Protein-Energy MalnutritionanletNo ratings yet
- Protein Energy MalnutritionDocument37 pagesProtein Energy MalnutritionVishu100% (1)
- Assignment: ON Role of Community Health Nurse in Management of Malnourished ChildDocument48 pagesAssignment: ON Role of Community Health Nurse in Management of Malnourished ChildSuman MondalNo ratings yet
- Physical Education and Health 12 Quarter 2-Module 3Document6 pagesPhysical Education and Health 12 Quarter 2-Module 3Reyanne Mae VillajuanNo ratings yet
- P.E Final Quiz 1Document4 pagesP.E Final Quiz 1Miguel Angelo GarciaNo ratings yet
- Assessing The Integumentary System RubricsDocument2 pagesAssessing The Integumentary System RubricsSamantha ZacharyNo ratings yet
- Mobileframe Healthcare Application Suite: Configurable Mobile ApplicationsDocument4 pagesMobileframe Healthcare Application Suite: Configurable Mobile ApplicationsSteveEpsteinNo ratings yet
- Press Release: JMX International Oncology Cancer Institute Surat, GujaratDocument2 pagesPress Release: JMX International Oncology Cancer Institute Surat, GujaratPankaj Narendrasinh RajNo ratings yet
- Assessments Are Biased - Socioeconomiclens - Acad MedDocument12 pagesAssessments Are Biased - Socioeconomiclens - Acad Mededensbatmitzvah2018No ratings yet
- Occimun Sanctum Tulsi DeviDocument9 pagesOccimun Sanctum Tulsi DeviBenancio DorantessNo ratings yet
- Drug Study: Republic of The Philippines City of Makati University of Makati College of Allied Health StudiesDocument35 pagesDrug Study: Republic of The Philippines City of Makati University of Makati College of Allied Health StudiesKrystel PeñosoNo ratings yet
- Exercises On Paragraph WritingDocument4 pagesExercises On Paragraph Writingburçin yaşarNo ratings yet
- Evan-Reference LetterDocument1 pageEvan-Reference Letterapi-311888118No ratings yet
- Physical Fitness PPT 2Document31 pagesPhysical Fitness PPT 2Johainna SalesNo ratings yet
- Sigma Theta Tau InternationalDocument10 pagesSigma Theta Tau InternationalpsubetasigmaNo ratings yet
- Transfer LetterDocument4 pagesTransfer LetterSarena GillNo ratings yet
- Postpartum DepressionDocument1 pagePostpartum DepressionNirmala BhattNo ratings yet
- Health Benefits of Spices - Kisan WorldDocument4 pagesHealth Benefits of Spices - Kisan WorldSomak MaitraNo ratings yet
- Anna Garcia Death Timeline 1Document19 pagesAnna Garcia Death Timeline 1api-245176779No ratings yet
- Wound CareDocument3 pagesWound Caregrangerhermionep100% (1)
- Cleft Sentences Review 3 - Ôn Tập Câu Chẻ 3Document3 pagesCleft Sentences Review 3 - Ôn Tập Câu Chẻ 3Vân Nguyễn Thảo100% (1)
- Case Presentation BY Dr. Prashanti Ophthalmology Ist YrDocument22 pagesCase Presentation BY Dr. Prashanti Ophthalmology Ist YrAyushman100% (3)
- Utk Thesis DefenseDocument5 pagesUtk Thesis Defenseafcnwwgnt100% (2)
- PPT Medicine Labels (Attachment 1)Document21 pagesPPT Medicine Labels (Attachment 1)DonnNo ratings yet
- MSDS Cocoa Powder PDFDocument3 pagesMSDS Cocoa Powder PDFkemang 35No ratings yet
- Cholelithiasis: Introduction: General Illness InformationDocument9 pagesCholelithiasis: Introduction: General Illness InformationJhangot Abad GabucoNo ratings yet
- Episiotomi Repair Vicryl Rapide Vs VicrylDocument3 pagesEpisiotomi Repair Vicryl Rapide Vs VicrylamilyapraditaNo ratings yet
- First Summative Test in Physical EducationDocument2 pagesFirst Summative Test in Physical EducationDainielle Marie PascualNo ratings yet
- Ahss 1170 Term Paper - Allison BakerDocument8 pagesAhss 1170 Term Paper - Allison Bakerapi-300330301No ratings yet
- Alzheimer's DisorderDocument1 pageAlzheimer's DisorderKassandra MerrillNo ratings yet
- SSRSDocument20 pagesSSRSElle ManalangNo ratings yet
- Metacognitive Reading Report # 1: General InstructionsDocument2 pagesMetacognitive Reading Report # 1: General InstructionsSeth Jarl G. AgustinNo ratings yet