Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gonioscopy A Text and Atlas (With Goniovideos)Document188 pagesGonioscopy A Text and Atlas (With Goniovideos)Luis Angel Jarajimenez100% (1)
- Home Health Manager RN in Los Angeles CA Resume Neil RayDocument2 pagesHome Health Manager RN in Los Angeles CA Resume Neil RayNeilRay2No ratings yet
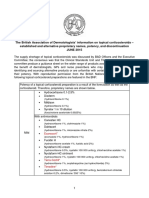
- Topical Corticosteroid Supply Shortage GuidanceDocument3 pagesTopical Corticosteroid Supply Shortage GuidancesyahrulroziNo ratings yet
- Malignant Hyperthermia: Clinical Diagnosis and Management of Acute CrisisDocument42 pagesMalignant Hyperthermia: Clinical Diagnosis and Management of Acute CrisisSamiir DNo ratings yet
- Anestheology Latest PDFDocument254 pagesAnestheology Latest PDFSamiir DNo ratings yet
- Tap BlocksDocument14 pagesTap BlocksSamiir DNo ratings yet
- Hyponatremia ManagementDocument13 pagesHyponatremia ManagementSamiir D100% (2)
- Drug Induced Movement DisordersDocument35 pagesDrug Induced Movement DisordersLucas PhiNo ratings yet
- Reconnective Healing: Beyond IntentionDocument2 pagesReconnective Healing: Beyond IntentionBentiv50% (2)
- Hospital Furniture NO Nama Produk Keterangan Price (RP) : Bed PasienDocument14 pagesHospital Furniture NO Nama Produk Keterangan Price (RP) : Bed PasienMonalisa ArmaniNo ratings yet
- Reference Regulatory AuthoritiesDocument2 pagesReference Regulatory AuthoritiesziadddNo ratings yet
- Nursing Board Review IDocument9 pagesNursing Board Review IShella Marie UsquisaNo ratings yet
- Squirting What You Need To Know... and MoreDocument9 pagesSquirting What You Need To Know... and MoreFarid Hamidou0% (1)
- Anatomy and Physiology of The Lymphatic SystemDocument153 pagesAnatomy and Physiology of The Lymphatic SystemNellie Grace Montes Aba-aNo ratings yet
- Malaria: Michelle Carandang-Cuvin, M.D. FPPS, Fpidsp Pediatric Infectious Disease ConsultantDocument77 pagesMalaria: Michelle Carandang-Cuvin, M.D. FPPS, Fpidsp Pediatric Infectious Disease ConsultantHanako AranillaNo ratings yet
- I. Choose The Word Whose Underlined Part Is Pronounced Differently From That of The OthersDocument3 pagesI. Choose The Word Whose Underlined Part Is Pronounced Differently From That of The Othershuy phạmNo ratings yet
- Chlorogenic Acid From Green Coffee Extract Are Highky Bioavailable in HumansDocument7 pagesChlorogenic Acid From Green Coffee Extract Are Highky Bioavailable in HumansGregory KalonaNo ratings yet
- Winnipeg Crisis Response CentreDocument2 pagesWinnipeg Crisis Response CentreqthermalNo ratings yet
- NCPDocument6 pagesNCPJoni Lyn Ba-as BayengNo ratings yet
- Turmeric Cream Mask B16 Edison G1Document25 pagesTurmeric Cream Mask B16 Edison G1Lance HeindrickNo ratings yet
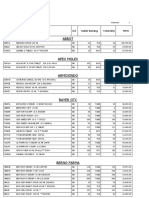
- Stok 15Document34 pagesStok 15Atik Marfu'ahNo ratings yet
- Pharmaceuticals & Biologics One-PagerDocument2 pagesPharmaceuticals & Biologics One-PagerBrianNo ratings yet
- Icdas IDocument9 pagesIcdas IBharath RatnakaramNo ratings yet
- Nano RobotDocument23 pagesNano RobotAnbazhagan Selvanathan100% (1)
- Velopharyngeal InsufficiencyDocument9 pagesVelopharyngeal InsufficiencyJASPREETKAUR0410No ratings yet
- 4357 - 22.Dr - Ravindra B. Gunale1 DR - Prajakta S. JagtapDocument2 pages4357 - 22.Dr - Ravindra B. Gunale1 DR - Prajakta S. Jagtap21 RakshitNo ratings yet
- Ahuja, Motiani - 2004 - Current and Evolving Issues in Transfusion PracticeDocument8 pagesAhuja, Motiani - 2004 - Current and Evolving Issues in Transfusion Practicesushmakumari009No ratings yet
- Apha 2012Document1 pageApha 2012ririn677No ratings yet
- Aminoff's Electrodiagnosis in Clinical NeurologyDocument20 pagesAminoff's Electrodiagnosis in Clinical NeurologyAbdul NasarNo ratings yet
- 3m Scotchbrite Quick Clean Griddle Cleaning SystemDocument12 pages3m Scotchbrite Quick Clean Griddle Cleaning Systemarturo gmoNo ratings yet
- CULHI - 5087 - Evolution of Pharmacy EssayDocument2 pagesCULHI - 5087 - Evolution of Pharmacy EssayRalph Aubrey CulhiNo ratings yet
- Chapter 151 - Cellulitis and ErysipelasDocument8 pagesChapter 151 - Cellulitis and ErysipelasDorothy BullecerNo ratings yet
- Concept of Pharmacodynamics and Pharmacokinetics in AyurvedaDocument8 pagesConcept of Pharmacodynamics and Pharmacokinetics in AyurvedaBalaji Kumar PanigrahiNo ratings yet
- Teori Keperawatan: T. Pangandaheng., S.Kep., NS., MSNDocument22 pagesTeori Keperawatan: T. Pangandaheng., S.Kep., NS., MSNTommy PangandahengNo ratings yet