Download as pptx, pdf, or txt
You might also like
- Nicu Checklist Bundles Infection Control 1Document60 pagesNicu Checklist Bundles Infection Control 1Mithlesh Dewangan92% (13)
- Mini Question Bank - Vety Sci - For Students PDFDocument106 pagesMini Question Bank - Vety Sci - For Students PDFRakesh Prajapati100% (3)
- Pedia-TicklerDocument9 pagesPedia-TicklerElizabeth MaderazoNo ratings yet
- CC 2 Okt Hcu NeoDocument26 pagesCC 2 Okt Hcu NeolatifahNo ratings yet
- Ob Endorsement BackupDocument18 pagesOb Endorsement BackupKevin AgbonesNo ratings yet
- Pagi Klinik Rs Usu Edit 27 Jan 2019Document126 pagesPagi Klinik Rs Usu Edit 27 Jan 2019syelsie amanda sariNo ratings yet
- Morning Report 18 April 2016 (KPD)Document29 pagesMorning Report 18 April 2016 (KPD)ArizkamhNo ratings yet
- Pagi Klinik 3 Mei 2018Document29 pagesPagi Klinik 3 Mei 2018Albert SitepuNo ratings yet
- Case ReportDocument37 pagesCase ReportKarina SurakusumaNo ratings yet
- CC NICU Rabu Malam 16 Jan 19Document41 pagesCC NICU Rabu Malam 16 Jan 19Primadiati Nickyta SariNo ratings yet
- Mrs. C. 56tn. 01032844, BIU, Uterine Prolapse Stage IVDocument23 pagesMrs. C. 56tn. 01032844, BIU, Uterine Prolapse Stage IVJonathan GnwNo ratings yet
- Obstetrics & Gynecology Department MORNING REPORT (Outpatient Clinic) Tuesday, April 13 2021Document19 pagesObstetrics & Gynecology Department MORNING REPORT (Outpatient Clinic) Tuesday, April 13 2021Rizkilbs LbsNo ratings yet
- Laporan Jaga Sabtu Malam, 26 Januari 2019: Supervisor: Dr. Tgk. Puspa Dewi SP - OGDocument10 pagesLaporan Jaga Sabtu Malam, 26 Januari 2019: Supervisor: Dr. Tgk. Puspa Dewi SP - OGAnonymous 6Us8y9wwLNo ratings yet
- Kematian Janin Dalam KandunganDocument30 pagesKematian Janin Dalam KandunganpriscaharahapNo ratings yet
- Morning Report Mrs. M (11 Januari 2022)Document11 pagesMorning Report Mrs. M (11 Januari 2022)fadhil ridhoNo ratings yet
- Penugasan Morning Report Pediatric - H1A021103 - Andi Muhammad Al Fatih HaqDocument17 pagesPenugasan Morning Report Pediatric - H1A021103 - Andi Muhammad Al Fatih HaqPentolNo ratings yet
- SC Oligo + IUGRDocument21 pagesSC Oligo + IUGRIrwin FitriansyahNo ratings yet
- CC KBRT 21 Sept 2018 Ibu VarisellaDocument27 pagesCC KBRT 21 Sept 2018 Ibu Variselladinarasri8966No ratings yet
- CC 31agustus 2017 KBRT Inggris EditDocument38 pagesCC 31agustus 2017 KBRT Inggris EditdelfiaNo ratings yet
- Case Study Obstetric PatientDocument19 pagesCase Study Obstetric PatientPrinz Lozano100% (1)
- Case Study Obstetric PatientDocument19 pagesCase Study Obstetric PatientPrinz LozanoNo ratings yet
- Case NoDocument18 pagesCase NorizkaNo ratings yet
- Panik VKDocument18 pagesPanik VKFadhilaMahlainiLubisNo ratings yet
- Obstetric Outpatient: Monday, April 2 2018Document22 pagesObstetric Outpatient: Monday, April 2 2018Riyan W. PratamaNo ratings yet
- Case No. 55Document33 pagesCase No. 55HovlantaNo ratings yet
- BARRI SIREESHA DischargeDocument4 pagesBARRI SIREESHA DischargeDaffaNo ratings yet
- Newborn NotesDocument44 pagesNewborn NotesHaziq KamardinNo ratings yet
- Previous CS Due To Contracted PelvicDocument23 pagesPrevious CS Due To Contracted PelvicIrwin FitriansyahNo ratings yet
- HieDocument9 pagesHieAnfas VNo ratings yet
- Duty Report Monday, February 4 2019Document55 pagesDuty Report Monday, February 4 2019Sylvan LaminaNo ratings yet
- Anc Case PresentationDocument24 pagesAnc Case PresentationNirupa RamachandranNo ratings yet
- Case PresentationDocument10 pagesCase PresentationnmreaperNo ratings yet
- Morning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriDocument9 pagesMorning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriIda Andalos TothaNo ratings yet
- Ectopic PregnancyDocument54 pagesEctopic Pregnancypatriciaatan1497No ratings yet
- Grand Case Presentation Group 1A Pedia PSHDocument70 pagesGrand Case Presentation Group 1A Pedia PSHAla'a Emerald AguamNo ratings yet
- Morning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriDocument9 pagesMorning Report March, 24: Supervisor: Dr.H. Doddy A.K., Spog DM: Akbar, Ariq, AsriAkbar GazaliNo ratings yet
- EklampsiaDocument8 pagesEklampsiamelatiigdNo ratings yet
- Preskas Boyolali Pandan ArangDocument25 pagesPreskas Boyolali Pandan Arangaoelia wardhanaNo ratings yet
- HPPDocument15 pagesHPPArizkamhNo ratings yet
- Ivena Case Fetal DistressDocument36 pagesIvena Case Fetal Distressdr nuriel anwarNo ratings yet
- REVISI FINAL - 20 - April - 2024 - Hirschsprung'sDocument18 pagesREVISI FINAL - 20 - April - 2024 - Hirschsprung'sHamdan SahlNo ratings yet
- MR (Prolaps Tali Pusat)Document16 pagesMR (Prolaps Tali Pusat)widyaanggariniNo ratings yet
- Ny KhairaniDocument16 pagesNy KhairaniHaris KurniawanNo ratings yet
- Panik Senin 10 September 2018 1 PasienDocument19 pagesPanik Senin 10 September 2018 1 PasienMegaSariDewiNo ratings yet
- Supervisor: Dr. Made Mahayasa, SP - OG Medical Students:: Morning ReportDocument6 pagesSupervisor: Dr. Made Mahayasa, SP - OG Medical Students:: Morning ReportNur LestaryNo ratings yet
- SalmahDocument17 pagesSalmahRian Segal HidajatNo ratings yet
- Case Presentation: Yousef Hassan Basman BazarDocument76 pagesCase Presentation: Yousef Hassan Basman BazarYousef Hassan BazarNo ratings yet
- L Neelaveni DischargeDocument4 pagesL Neelaveni DischargeDaffaNo ratings yet
- P A Partus Maturus With Caesarea Section E.C Breech Position With Ebw 3500 + SC HistoryDocument59 pagesP A Partus Maturus With Caesarea Section E.C Breech Position With Ebw 3500 + SC HistoryDema Syah FadliNo ratings yet
- Case Report - G1P0A0 Parturian 40-41 Weeks + Severe PE + ROMDocument29 pagesCase Report - G1P0A0 Parturian 40-41 Weeks + Severe PE + ROMsurbakti_christineNo ratings yet
- Marsella NSDocument3 pagesMarsella NSIlmiah Program studi ObginNo ratings yet
- Sample Obg Case SheetDocument10 pagesSample Obg Case SheetKamil AlchalisNo ratings yet
- 04-12-13 Letak Sugsang FinishDocument13 pages04-12-13 Letak Sugsang FinishAnonymous L3q7yHhhNo ratings yet
- Molar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDocument99 pagesMolar Pregnancy: November 2018 Jis Dungca, Delos Santos, CrisostomoDarnell DelgadoNo ratings yet
- TambhanDocument34 pagesTambhanBudiNo ratings yet
- Presentation Utk State Meetng (DR DAUD)Document45 pagesPresentation Utk State Meetng (DR DAUD)Mohd Daud Che YusofNo ratings yet
- Case Conference Tuesday, FEBRUARY 13, 2018Document41 pagesCase Conference Tuesday, FEBRUARY 13, 2018Ahimsa Yoga AninditaNo ratings yet
- Case Presentation Febrile FitDocument33 pagesCase Presentation Febrile FitNurul Syazwani RamliNo ratings yet
- 27-10-09 PagiDocument3 pages27-10-09 PagiLaili KhairaniNo ratings yet
- Panik Onko Ward HAM 15 Okt 2020Document75 pagesPanik Onko Ward HAM 15 Okt 2020PPDS Ivan PasaribuNo ratings yet
- Morning Report Saturday, 10 MARCH 2018Document33 pagesMorning Report Saturday, 10 MARCH 2018Efan StiawanNo ratings yet
- Prenatal AsphyxiaDocument15 pagesPrenatal AsphyxiaSampat KumawatNo ratings yet
- Basic Monitoring in Canine and Feline Emergency PatientsFrom EverandBasic Monitoring in Canine and Feline Emergency PatientsElizabeth J ThomovskyRating: 1 out of 5 stars1/5 (1)
- 10 1 1 563 4316 PDFDocument5 pages10 1 1 563 4316 PDFAuliaRahmanNo ratings yet
- Syarah Hikam 1Document108 pagesSyarah Hikam 1AuliaRahmanNo ratings yet
- Anamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPDocument4 pagesAnamnesis:: BB KG TB CM No - RM TGL - Masuk TGL - Lahir DPJPAuliaRahmanNo ratings yet
- 2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisDocument22 pages2006 118 1774 Subcommittee On Diagnosis and Management of BronchiolitisAuliaRahmanNo ratings yet
- Jurnal OkeDocument8 pagesJurnal OkeAuliaRahmanNo ratings yet
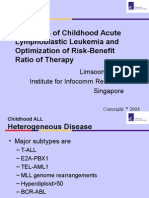
- Diagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyDocument24 pagesDiagnosis of Childhood Acute Lymphoblastic Leukemia and Optimization of Risk-Benefit Ratio of TherapyAuliaRahmanNo ratings yet
- Makalah Brain GYM International, BDocument17 pagesMakalah Brain GYM International, BAuliaRahmanNo ratings yet
- Wilayah 3'-DiterjemahkanDocument1 pageWilayah 3'-DiterjemahkanAuliaRahmanNo ratings yet
- Interesting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaDocument10 pagesInteresting Case: Masruri, Esha, Alex, Milza, Wicak, Gita, Zaki, Arin, Eni, FiaAuliaRahmanNo ratings yet
- Pediatric Dental CareDocument27 pagesPediatric Dental CareAuliaRahmanNo ratings yet
- 1-Month Weight Increments BOYS: Birth To 12 Months (Percentiles)Document1 page1-Month Weight Increments BOYS: Birth To 12 Months (Percentiles)AuliaRahmanNo ratings yet
- Weight Inc Birth To 60 Days Girls PDFDocument1 pageWeight Inc Birth To 60 Days Girls PDFAuliaRahmanNo ratings yet
- CholesteatomaDocument9 pagesCholesteatomasergeantchai068No ratings yet
- BCMJ 53 Vol6 Febrile SeizuresDocument6 pagesBCMJ 53 Vol6 Febrile SeizuresdyyyaNo ratings yet
- Trabalho Ingles Fake NewsDocument3 pagesTrabalho Ingles Fake NewsFelipe ZuriqueNo ratings yet
- LabReportNew - 2022-12-29 EKTAT213904.745Document5 pagesLabReportNew - 2022-12-29 EKTAT213904.745Ekta BaraskarNo ratings yet
- Bed BathDocument10 pagesBed BathjokazelNo ratings yet
- Infectious DiseasesDocument508 pagesInfectious DiseasesFlorentina-Alina CondoiuNo ratings yet
- Felocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Document1 pageFelocell Felv Helps Prevent Disease Cause by Feline Leukemia Virus (Felv)Reginaldo ParcianelloNo ratings yet
- Prev Med Mar 2022Document8 pagesPrev Med Mar 2022Sanielle Karla Garcia LorenzoNo ratings yet
- A Study About Importance of Biosafety and Biosecurity On Aspect of Good Laboratory Practice (GLP) in A Quality Control (QC) Laboratory of BangladeshDocument11 pagesA Study About Importance of Biosafety and Biosecurity On Aspect of Good Laboratory Practice (GLP) in A Quality Control (QC) Laboratory of BangladeshPremier PublishersNo ratings yet
- Transfusion Transmited Diseases WpordDocument4 pagesTransfusion Transmited Diseases WpordNyxa AbdullaNo ratings yet
- Respiratory PathologyDocument62 pagesRespiratory PathologyErnest ReddcliffvcksuNo ratings yet
- Wound InfectionDocument21 pagesWound Infectionmaak85No ratings yet
- Micro - SupDocument9 pagesMicro - SupAbdoulhaleem MoNo ratings yet
- Drug Study For HepatitisDocument4 pagesDrug Study For Hepatitisunyokies100% (1)
- One Point Acupressure TreatmentDocument81 pagesOne Point Acupressure TreatmentNarasannapeta Patanjali100% (2)
- Oral Sex Myths and FactsDocument3 pagesOral Sex Myths and FactsarpitmatlabNo ratings yet
- 5th Year Pediatric Exam 2016Document14 pages5th Year Pediatric Exam 2016pal_pal_palNo ratings yet
- Writing 1 Composition - Laura RomeroDocument2 pagesWriting 1 Composition - Laura RomeroLaura RomeroNo ratings yet
- Common Foodborne PathogensDocument3 pagesCommon Foodborne PathogensO PNo ratings yet
- Mcqs EpidemeologyDocument28 pagesMcqs Epidemeologymd aquibNo ratings yet
- Free GRE Practice Test - 100+ GRE Sample TestsDocument7 pagesFree GRE Practice Test - 100+ GRE Sample TestsPrajwal Praj GNo ratings yet
- National Cancer Control Programmes in ThailandDocument93 pagesNational Cancer Control Programmes in ThailandIndonesian Journal of CancerNo ratings yet
- Infections of The EyesDocument49 pagesInfections of The EyesBea Bianca CruzNo ratings yet
- Cultural Anthropophagy As A From of Cannibalism Based On The Phenomenon of IconophagyDocument35 pagesCultural Anthropophagy As A From of Cannibalism Based On The Phenomenon of IconophagydomingofsanzNo ratings yet
- Can Oral Sex Transmit HIV?Document52 pagesCan Oral Sex Transmit HIV?Leo LamsNo ratings yet
- Case For Acute GastroenteritisDocument26 pagesCase For Acute GastroenteritisSheana TmplNo ratings yet
- Biology Project PDFDocument28 pagesBiology Project PDFViraz PrajapatiNo ratings yet