Download as pptx, pdf, or txt
You might also like
- View Duplicate Invoice - Apple IphoneDocument1 pageView Duplicate Invoice - Apple IphoneGas67% (3)
- Contraceptive Injection Calendar: Given Due Given Due Given Due Given DueDocument2 pagesContraceptive Injection Calendar: Given Due Given Due Given Due Given Dueiniciate07No ratings yet
- Posonic HomeAlarm EX10 & EX18 Installation Manual - Rev1.0Document54 pagesPosonic HomeAlarm EX10 & EX18 Installation Manual - Rev1.0Vlad Florescu100% (3)
- Dr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueDocument20 pagesDr. Uun Sumardi, SPPD, K-PTI, KIC, FINASIM-Fluid Management in Severe DengueOlivia DwimaswastiNo ratings yet
- LECTURE 1 Introduction of InfectionDocument29 pagesLECTURE 1 Introduction of Infectiontari riyastiNo ratings yet
- TROMBOSISDocument49 pagesTROMBOSISAgung WistaraNo ratings yet
- Update Diagnosis and TherapyDocument29 pagesUpdate Diagnosis and TherapyRosi AmaliaNo ratings yet
- Emergency Medicine-Aru W. SudoyoDocument44 pagesEmergency Medicine-Aru W. SudoyoArdhiNo ratings yet
- DyspneaDocument34 pagesDyspneaAlvin BrilianNo ratings yet
- Acute Myocard InfarcDocument2 pagesAcute Myocard InfarcGun TargunaNo ratings yet
- 4.18 Mankad Echo in Systemic DiseaseDocument97 pages4.18 Mankad Echo in Systemic DiseaseDiana_anca6No ratings yet
- Diagnosa Icd 10 SilDocument51 pagesDiagnosa Icd 10 SilinayaNo ratings yet
- 1 SpotterDocument41 pages1 Spotterrakhisurya_15No ratings yet
- Chapter 12, Transfer To Definitive CareDocument13 pagesChapter 12, Transfer To Definitive CareDeka Dharma PutraNo ratings yet
- National ART Clinical Guideline 2023 - 04 - 28 SignedDocument44 pagesNational ART Clinical Guideline 2023 - 04 - 28 SignedZimkita Zintle MakeleniNo ratings yet
- Trulicity Webinar PAPDI Makassar 20 November 2021 MakbulDocument40 pagesTrulicity Webinar PAPDI Makassar 20 November 2021 MakbulNur Sabriany LihawaNo ratings yet
- Malaria Treatment UpdateDocument45 pagesMalaria Treatment UpdateGyabaah Yeboah AndrewsNo ratings yet
- Protap NTG DripDocument4 pagesProtap NTG DripAinil MardiahNo ratings yet
- ATLSDocument52 pagesATLSBelLa EakoiNo ratings yet
- Case Based Discussion: Cintya Dunihapsari 012116354 Coass Interna - Rsi Sultan Agung SemarangDocument25 pagesCase Based Discussion: Cintya Dunihapsari 012116354 Coass Interna - Rsi Sultan Agung SemarangCintyaNo ratings yet
- Cme Acs 2. Stemi (Izzah)Document36 pagesCme Acs 2. Stemi (Izzah)Hakimah K. SuhaimiNo ratings yet
- Morocco Top ScientistsDocument358 pagesMorocco Top Scientistsa.drioicheNo ratings yet
- Hypertensive Emergencies (ESC 2019)Document10 pagesHypertensive Emergencies (ESC 2019)Glen LazarusNo ratings yet
- Vascular Disease-Lecture Prof SyukriDocument109 pagesVascular Disease-Lecture Prof SyukriYayatRuslan100% (1)
- 3 Heart InternetNewDocument55 pages3 Heart InternetNewCoral Srinivasa RamaluNo ratings yet
- CAD - EBM September 2020 EditionDocument17 pagesCAD - EBM September 2020 EditionNaga Venkatamanoj Kumar PakalapatiNo ratings yet
- Suz 183Document29 pagesSuz 183Benny Chris TantoNo ratings yet
- Essential HypertensionDocument13 pagesEssential HypertensionIvan KurniadiNo ratings yet
- IAP ALS Handbook ErratumDocument6 pagesIAP ALS Handbook ErratumAnurag ReddyNo ratings yet
- Senile Cataract (Age-Related Cataract) Clinical Presentation - History, Physical, Causes PDFDocument4 pagesSenile Cataract (Age-Related Cataract) Clinical Presentation - History, Physical, Causes PDFAhmad FahroziNo ratings yet
- Drugs Used For Treatment Stable Angina PectorisDocument29 pagesDrugs Used For Treatment Stable Angina PectorisAditya Andra PerdanaNo ratings yet
- Neurology SlidesDocument38 pagesNeurology Slidesdrmalsharrakhi_32794100% (1)
- Diabetic NephropathyDocument62 pagesDiabetic Nephropathydevyani meshram100% (1)
- WHO MDR 2020 Handbook Treatment PDFDocument88 pagesWHO MDR 2020 Handbook Treatment PDFYuanita GunawanNo ratings yet
- Sample Observed HX - Ms J - AsthmaDocument5 pagesSample Observed HX - Ms J - AsthmaZi SongNo ratings yet
- Venous ThromboembolismDocument49 pagesVenous Thromboembolismadamu mohammadNo ratings yet
- CV SuryaniDocument3 pagesCV SuryaniErna HakimNo ratings yet
- Nutrition Support in Critically Ill PatientDocument19 pagesNutrition Support in Critically Ill PatienttantoNo ratings yet
- Effect of Weekly Subcutaneous Semaglutide Vs Daily LiraglutideDocument13 pagesEffect of Weekly Subcutaneous Semaglutide Vs Daily LiraglutideChanikarn Julputipong100% (1)
- Perioperative Management in Diabetes MellitusDocument20 pagesPerioperative Management in Diabetes MellitusChristopher RyalinoNo ratings yet
- Permanent FormDocument4 pagesPermanent FormdgfuiNo ratings yet
- Palliative EnciesDocument96 pagesPalliative EnciesnandanNo ratings yet
- Legacy Effect in Diabetes MnanagementDocument9 pagesLegacy Effect in Diabetes MnanagementSouradipta GangulyNo ratings yet
- VAP SlidesDocument25 pagesVAP SlidesGladys OliviaNo ratings yet
- Intradialytic Hypertension Time To Act 10Document7 pagesIntradialytic Hypertension Time To Act 10Nia FirdiantyNo ratings yet
- PneumothoraxDocument24 pagesPneumothoraxItharshan IndreswaranNo ratings yet
- CVS K39 Antiphospholipid Prof. HarimanDocument38 pagesCVS K39 Antiphospholipid Prof. HarimanYohanna SinuhajiNo ratings yet
- CVC Care Policy and Procedure RevisedDocument5 pagesCVC Care Policy and Procedure RevisedCynthia RinosNo ratings yet
- Integrated Medical Seminar Diabetes MellitusDocument33 pagesIntegrated Medical Seminar Diabetes MellitusKyo Jie MingNo ratings yet
- Practice Guidelines: For Family PhysiciansDocument0 pagesPractice Guidelines: For Family PhysiciansMuhammad GoharNo ratings yet
- Pre Anesthetic Evaluation in DM - Liya AbrahamDocument16 pagesPre Anesthetic Evaluation in DM - Liya Abrahamvenky2430% (1)
- Nitrates andDocument61 pagesNitrates andMrunalini DandamudiNo ratings yet
- Question ID Title Last Revision: Page 30) Page 32)Document4 pagesQuestion ID Title Last Revision: Page 30) Page 32)AnisulHaqueNo ratings yet
- Empagliflozin in Heart Failure With A Preserved Ejection FractionDocument11 pagesEmpagliflozin in Heart Failure With A Preserved Ejection Fractionsri wahyuniNo ratings yet
- Gallbladder and Extrahepatic Biliary System - FinlDocument14 pagesGallbladder and Extrahepatic Biliary System - FinlJoevet T. TadlasNo ratings yet
- 4 - Endocrinology Tiki TakaDocument32 pages4 - Endocrinology Tiki TakaHemaNo ratings yet
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234No ratings yet
- Acls Mega Code 1Document31 pagesAcls Mega Code 1mj8bfgxbyjNo ratings yet
- Abdominal ExaminationDocument11 pagesAbdominal Examinationibra100% (1)
- Meningitis - Practice Essentials, Background, PathophysiologyDocument26 pagesMeningitis - Practice Essentials, Background, PathophysiologydilaNo ratings yet
- DR Aida Lombok 3 Mei 2017 - HisfarsiDocument39 pagesDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamNo ratings yet
- Diabetes MelitusDocument57 pagesDiabetes MelitusArzyad Analis KesehatanNo ratings yet
- MATA - 7. Bank MataDocument21 pagesMATA - 7. Bank MataAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter13CNSPart2MariebDocument23 pagesANATOMI - Chapter13CNSPart2MariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter25ReproFemaleMariebDocument30 pagesANATOMI - Chapter25ReproFemaleMariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter24UrinaryMariebDocument28 pagesANATOMI - Chapter24UrinaryMariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter23DigestivePart2MariebDocument23 pagesANATOMI - Chapter23DigestivePart2MariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter13CNSPart1MariebDocument25 pagesANATOMI - Chapter13CNSPart1MariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter11MusclesPart1MariebDocument19 pagesANATOMI - Chapter11MusclesPart1MariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter10MuscleTissueMariebDocument33 pagesANATOMI - Chapter10MuscleTissueMariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter7AxialSkeletonMariebDocument30 pagesANATOMI - Chapter7AxialSkeletonMariebAdhi TjahyadiNo ratings yet
- ANATOMI - Chapter4TissuesMariebPart1Document23 pagesANATOMI - Chapter4TissuesMariebPart1Adhi TjahyadiNo ratings yet
- Hematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Document52 pagesHematology Review: by Felicia Magee Tardy, M.S., MT (Ascp)Adhi TjahyadiNo ratings yet
- Anak - AsfiksiaDocument28 pagesAnak - AsfiksiaAdhi TjahyadiNo ratings yet
- Bpjs Case Study DiabetesDocument33 pagesBpjs Case Study DiabetesAdhi TjahyadiNo ratings yet
- Investment Analysis and Portfolio ManagementDocument5 pagesInvestment Analysis and Portfolio ManagementMuhammad QasimNo ratings yet
- Intermediate Microeconomics and Its Application 11Th Edition Nicholson Solutions Manual Full Chapter PDFDocument30 pagesIntermediate Microeconomics and Its Application 11Th Edition Nicholson Solutions Manual Full Chapter PDFJulieHaasyjzp100% (13)
- 50 Years Data Science by Dave DonohoDocument41 pages50 Years Data Science by Dave DonohoVikram JayaramNo ratings yet
- "Pab Rules": Denr - Emb XiDocument38 pages"Pab Rules": Denr - Emb XiLeslie Balneg RubinNo ratings yet
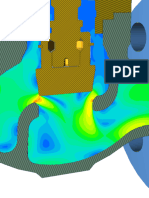
- Flow Simulation of A DN100 Globe Valve Performance Report Generated Using SimulationHub's Autonomous Valve CFD AppDocument19 pagesFlow Simulation of A DN100 Globe Valve Performance Report Generated Using SimulationHub's Autonomous Valve CFD AppSneha ShettyNo ratings yet
- Eureka Coin White Paper DraftDocument24 pagesEureka Coin White Paper DraftImdad AliNo ratings yet
- Law On Public Officers 05.06.14Document27 pagesLaw On Public Officers 05.06.14Imman DCPNo ratings yet
- Treasury RCM 2022-2023Document1 pageTreasury RCM 2022-2023Aman ParchaniNo ratings yet
- Profile 2-2023 (2)Document51 pagesProfile 2-2023 (2)Osama SharakyNo ratings yet
- OPP Log FileDocument2 pagesOPP Log FileVenkatesh VenkatNo ratings yet
- Nationalism in IndiaDocument9 pagesNationalism in Indiathinkiit0% (1)
- Network Layer Routing in Packet Networks Shortest Path RoutingDocument45 pagesNetwork Layer Routing in Packet Networks Shortest Path RoutingHalder SubhasNo ratings yet
- Studycase Week 4 Kelompok Breakout 3Document7 pagesStudycase Week 4 Kelompok Breakout 3Mutiara PadangNo ratings yet
- Literature Review FinalDocument4 pagesLiterature Review Finalapi-549244735No ratings yet
- Business Proposal Hubli PDFDocument3 pagesBusiness Proposal Hubli PDFKavithaNo ratings yet
- 1100 Series Magnetic Level Indicator - CAT1596 1Document18 pages1100 Series Magnetic Level Indicator - CAT1596 1Smith CBNo ratings yet
- Technical CollegesDocument228 pagesTechnical CollegesRupak TiwariNo ratings yet
- Robin ZupancDocument3 pagesRobin Zupancnemanja aleksicNo ratings yet
- Project Report GuidelinesDocument8 pagesProject Report GuidelinesHarshil TejaniNo ratings yet
- Scope of Work For Canopy Replacement of DRS/MRS: 1.0 GeneralDocument9 pagesScope of Work For Canopy Replacement of DRS/MRS: 1.0 GeneralDevang PatelNo ratings yet
- AP57.2-0608-3 (IR) Fuel Quantity Measuring Stick Data For Ground Attitudes 757-200Document65 pagesAP57.2-0608-3 (IR) Fuel Quantity Measuring Stick Data For Ground Attitudes 757-200brains26No ratings yet
- PQ 266 SL II P 03 Legal Framework Case Study PDFDocument3 pagesPQ 266 SL II P 03 Legal Framework Case Study PDFUshani CabralNo ratings yet
- List of Barricades:: Sr. No. Section Line No DescriptionDocument4 pagesList of Barricades:: Sr. No. Section Line No DescriptionSafety DeptNo ratings yet
- Alabang Vs MuntinlupaDocument2 pagesAlabang Vs MuntinlupaLauriz EsquivelNo ratings yet
- Personal Assistant ContractDocument5 pagesPersonal Assistant Contractjamieclarkson75No ratings yet
- Westinghouse Lighting Price List Outdoor Lighting 5-71Document16 pagesWestinghouse Lighting Price List Outdoor Lighting 5-71Alan MastersNo ratings yet
- Email Apology SolutionDocument5 pagesEmail Apology SolutionlinhntmNo ratings yet
- Retail Fin IntegrationDocument4 pagesRetail Fin IntegrationNabeel RashidNo ratings yet