Download as ppt, pdf, or txt
You might also like
- The Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachDocument8 pagesThe Ten-Step Vaginal Hysterectomy - A Newer and Better ApproachqisthiaufaNo ratings yet
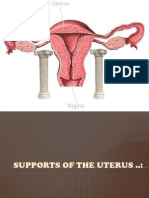
- Supports of The UterusDocument20 pagesSupports of The UterusAshwin Prem Solomon100% (1)
- UTI On A Background of Obstructive NephropathyDocument26 pagesUTI On A Background of Obstructive NephropathyAminath MeesanNo ratings yet
- Unlearn Your Pain Chapter 5 TMSDocument17 pagesUnlearn Your Pain Chapter 5 TMSSyedNo ratings yet
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Diagnosis and Management of Pelvic Organ ProlapseDocument47 pagesDiagnosis and Management of Pelvic Organ ProlapseWindy Puspa Kusumah100% (1)
- Menstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoDocument36 pagesMenstrual Disorders: Olufemi Aworinde Lecturer/ Consultant Obstetrician and Gynaecologist, Bowen University, IwoAkinbani MoyosoreNo ratings yet
- Blood Supply Pelvic OrgansDocument39 pagesBlood Supply Pelvic OrgansoliviaNo ratings yet
- Ultrasound - A GuideDocument9 pagesUltrasound - A GuideDebasish KunduNo ratings yet
- Anatomy of Female Genital TractDocument99 pagesAnatomy of Female Genital TractIuliana StefanucaNo ratings yet
- POP June 10,2021 1Document48 pagesPOP June 10,2021 1Kerod AbebeNo ratings yet
- Anal Fissure: BY Alisha SaleemDocument7 pagesAnal Fissure: BY Alisha Saleemashar khanNo ratings yet
- Deep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateDocument11 pagesDeep Vein Thrombosis and Pulmonary Embolism in Pregnancy - Prevention - UpToDateGabyta007No ratings yet
- Hormonal ContraceptivesDocument25 pagesHormonal Contraceptivesmd easarur rahmanNo ratings yet
- Instrumental Vaginal Delivery: Professor Roshan Ara QaziDocument27 pagesInstrumental Vaginal Delivery: Professor Roshan Ara Qazikaram008No ratings yet
- Genital ProlapseDocument13 pagesGenital ProlapsesmbawasainiNo ratings yet
- Ob - Operative ObstetricsDocument224 pagesOb - Operative Obstetricsapi-385605133% (3)
- Dystocia 2010Document55 pagesDystocia 2010Meigy NitalessyNo ratings yet
- AMTSL BrieferDocument2 pagesAMTSL BrieferNewborn2013No ratings yet
- Choriocarcinoma 11Document23 pagesChoriocarcinoma 11Fakhir HasanNo ratings yet
- Non-Surgical and Surgical Management of Pelvic OrgDocument10 pagesNon-Surgical and Surgical Management of Pelvic OrgAhmed AnwarNo ratings yet
- 8surgical Management of Dysfunctional Uterine Bleeding - KabilanDocument14 pages8surgical Management of Dysfunctional Uterine Bleeding - KabilanNavani TharanNo ratings yet
- Genital FistulaeDocument15 pagesGenital Fistulaesangeetha francisNo ratings yet
- GYNE UltrasoundgyneDocument11 pagesGYNE UltrasoundgyneMara AbantoNo ratings yet
- Laparoscopic Gynecologist Surgeon in HSR Layout BangaloreDocument8 pagesLaparoscopic Gynecologist Surgeon in HSR Layout BangaloreDr.Beena JeysinghNo ratings yet
- Trial of LabourDocument2 pagesTrial of Labourgeorgeloto12No ratings yet
- Instrumental DeliveryDocument8 pagesInstrumental DeliveryJustine Bianca NayreNo ratings yet
- Instrumental DeliveryDocument25 pagesInstrumental DeliveryAhmed ElmohandesNo ratings yet
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 pagesد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedNo ratings yet
- Pop QDocument45 pagesPop QObgyn Maret2016No ratings yet
- Assessment of Fetal Well BeingDocument46 pagesAssessment of Fetal Well BeingAumrin Fathima100% (1)
- Malformation of Female Reproductive SystemDocument170 pagesMalformation of Female Reproductive SystemKriti BanstolaNo ratings yet
- Secondary AmenorrheaDocument18 pagesSecondary AmenorrheaMaria Gill100% (1)
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- Abnormal Uterin ActionDocument65 pagesAbnormal Uterin Actionshweta raiNo ratings yet
- PerineumDocument4 pagesPerineumwiwin09No ratings yet
- Submitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDocument9 pagesSubmitted By: Diana M. Resultay A301/Group-3B Submitted To: Ms. ReyesDiannetotz MoralesNo ratings yet
- C SectionDocument50 pagesC SectionAlano S. LimgasNo ratings yet
- AUBDocument26 pagesAUByayaslaras96No ratings yet
- Vesico Vaginal FistulaDocument6 pagesVesico Vaginal Fistulaapi-3705046No ratings yet
- Benign Disease of The UterusDocument27 pagesBenign Disease of The UterusnyangaraNo ratings yet
- Normal Changes During PregnancyDocument48 pagesNormal Changes During PregnancyMariebel EbeNo ratings yet
- Obstetric EmergenciesDocument15 pagesObstetric EmergenciesAndi SaputraNo ratings yet
- Shubrat Singh: EctopicDocument25 pagesShubrat Singh: Ectopicshubham royalNo ratings yet
- Scaohoid Fracture 4Document34 pagesScaohoid Fracture 4Noor Al Zahraa Ali100% (1)
- Ectopic PregnancyDocument14 pagesEctopic Pregnancymilka agustinaNo ratings yet
- Endometrial PolypsDocument14 pagesEndometrial PolypsMusaNo ratings yet
- Dr. Sharda Jain: Director: Secretary GeneralDocument91 pagesDr. Sharda Jain: Director: Secretary GeneraljijaniNo ratings yet
- Anatomy of Female Genital Tract by Sidra IftikharDocument33 pagesAnatomy of Female Genital Tract by Sidra IftikharWaqas Tahir100% (1)
- Genital ProlapseDocument9 pagesGenital Prolapsesher singhNo ratings yet
- Reproductive Endocrinology FinalDocument98 pagesReproductive Endocrinology FinalChino Paolo SamsonNo ratings yet
- Uterine FibroidsDocument47 pagesUterine FibroidsMoh Aldhy HusaintNo ratings yet
- Cervical EncirclageDocument8 pagesCervical EncirclageAnnapurna DangetiNo ratings yet
- Obstetric FistulaeDocument24 pagesObstetric FistulaenyangaraNo ratings yet
- Pelvic Organ Prolapse - Dr. QueDocument55 pagesPelvic Organ Prolapse - Dr. QueMenjale JulaoNo ratings yet
- 16-Genital ProlapseDocument37 pages16-Genital Prolapseapi-3703352No ratings yet
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- UntitledDocument43 pagesUntitledDakshayini MbNo ratings yet
- O&G Counselling - TSPDocument6 pagesO&G Counselling - TSPTarran PhagooNo ratings yet
- Pelvic AnatomyDocument106 pagesPelvic AnatomyRosu George100% (1)
- CMS - Ob - Gyn 1-Answers PDFDocument13 pagesCMS - Ob - Gyn 1-Answers PDFSelena GajićNo ratings yet
- AUS 05 History and Physical ExaminationDocument39 pagesAUS 05 History and Physical ExaminationhalayehiahNo ratings yet
- Physiology and Pharmacology of The Bladder and Urethra: Gregorio, Frances Mari Mendoza, AlyannaDocument29 pagesPhysiology and Pharmacology of The Bladder and Urethra: Gregorio, Frances Mari Mendoza, AlyannaLic MendozaNo ratings yet
- Nursing Care - Roxana BucurDocument40 pagesNursing Care - Roxana BucurMarin AndreiNo ratings yet
- Guidelines On: Chronic Pelvic PainDocument90 pagesGuidelines On: Chronic Pelvic PainPatrascu CristiNo ratings yet
- Evaluation of Dysuria in AdultsDocument8 pagesEvaluation of Dysuria in AdultspapermintNo ratings yet
- Program-SUFU 2020 Winter Meeting-2252020Document39 pagesProgram-SUFU 2020 Winter Meeting-2252020Christopher KinsellaNo ratings yet
- EFIC European Pain Diploma Reading ListDocument7 pagesEFIC European Pain Diploma Reading ListJoana MoreiraNo ratings yet
- Considering The Potential For An Increase in Chronic Pain After The COVID-19 PandemicDocument4 pagesConsidering The Potential For An Increase in Chronic Pain After The COVID-19 Pandemic幸福KoreaNo ratings yet
- Pentosan Polysulfate SodiumDocument1 pagePentosan Polysulfate SodiumOdessa FileNo ratings yet
- Female Urinary SystemDocument5 pagesFemale Urinary SystemVikas SarkarNo ratings yet
- عجائب دودة العلقDocument28 pagesعجائب دودة العلقمريم عودةNo ratings yet
- Chronic Pelvic Pain and Dysfunction Practical Physical Medicine 2012Document461 pagesChronic Pelvic Pain and Dysfunction Practical Physical Medicine 2012Milos Djuric100% (4)
- Urinalysis (Ua) and The Diagnosis of UtisDocument5 pagesUrinalysis (Ua) and The Diagnosis of UtisErawati ArmayaniNo ratings yet
- Cheat Sheet - EAU Pelvic PainDocument1 pageCheat Sheet - EAU Pelvic PainJan HiblbauerNo ratings yet
- Music Lifts Dementia's Constant Fog - The AustralianDocument1 pageMusic Lifts Dementia's Constant Fog - The AustralianJane LyonsNo ratings yet
- Top 17 Questions in Urology: in This Chapter, We'll Go Over Common Health Problems in UrologyDocument13 pagesTop 17 Questions in Urology: in This Chapter, We'll Go Over Common Health Problems in UrologyadenwijayaNo ratings yet
- Hyacyst ClinicalDocument24 pagesHyacyst ClinicalEnrique S OcampoNo ratings yet
- Management of Chronic Pelvic Pain A Practical Manual by Michael HibnerDocument275 pagesManagement of Chronic Pelvic Pain A Practical Manual by Michael HibnerromarcNo ratings yet
- Chronic Pelvic PainDocument35 pagesChronic Pelvic PainAbong Che InnocentNo ratings yet
- Ic Food ListDocument7 pagesIc Food ListKim Othic100% (1)
- Dmso Natures Best HealerDocument2 pagesDmso Natures Best HealerJan Pran100% (1)
- Interstitial Cystitis & Painful Bladder Syndrome: A Guide For WomenDocument2 pagesInterstitial Cystitis & Painful Bladder Syndrome: A Guide For Womencateterdoblejota100% (1)
- Elmiron - E Janssen Nov 2011 Sodium Pentosan PolysulfateDocument18 pagesElmiron - E Janssen Nov 2011 Sodium Pentosan PolysulfateManjit WadhwaNo ratings yet
- CystitisDocument13 pagesCystitisTin VidovićNo ratings yet
- Biomedicines 10 00675Document17 pagesBiomedicines 10 00675tasialalalaNo ratings yet
- IPPS 2012 Program Book PDFDocument392 pagesIPPS 2012 Program Book PDFJanet L WarrenNo ratings yet
- Interstitial Cystitis (Painful Bladder Syndrome) - Causes & TreatmentDocument12 pagesInterstitial Cystitis (Painful Bladder Syndrome) - Causes & TreatmentJimmy GillNo ratings yet
- Introduction To Pelvic Pain 2019Document20 pagesIntroduction To Pelvic Pain 2019MrEnttNo ratings yet