
Unit II Heart Failure Spring 2014-1
Unit II Heart Failure Spring 2014-1
You might also like
- 1 Clinical Veterinary Advisor - Dogs and Cats 1-100 - RemovedDocument49 pages1 Clinical Veterinary Advisor - Dogs and Cats 1-100 - RemovedArieromNo ratings yet
- Treatment Planning Functional OcclusionDocument8 pagesTreatment Planning Functional OcclusionLandon Allen100% (1)
- 4.heart Failure HandoutDocument108 pages4.heart Failure HandoutGetachewNo ratings yet
- Final NTSB Report On Lockhart CrashDocument65 pagesFinal NTSB Report On Lockhart CrashAnonymous QUzIACmcB100% (1)
- Lyn Watson Level TwoDocument4 pagesLyn Watson Level TwoAlastair HarrisNo ratings yet
- Congestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho StudentsDocument27 pagesCongestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho Studentsmuluneh birhaneNo ratings yet
- Heart To HeartDocument110 pagesHeart To HeartmahyorwaNo ratings yet
- Heart FailureDocument52 pagesHeart Failurerania salsabilaNo ratings yet
- Congestive Heart Failure: Elias S. (MD+) March 2015 DBUDocument35 pagesCongestive Heart Failure: Elias S. (MD+) March 2015 DBUkikiNo ratings yet
- Sinaia 2 Oct 2014 - Final-Acute Heart FailureDocument285 pagesSinaia 2 Oct 2014 - Final-Acute Heart FailureBogdanel MihaiNo ratings yet
- Congestive Heart FailureDocument28 pagesCongestive Heart Failuresarguss1480% (5)
- Acute Heart FailureDocument18 pagesAcute Heart FailureGeorge GeorgeNo ratings yet
- Congestive Heart FailureDocument39 pagesCongestive Heart FailureEthiopia TekdemNo ratings yet
- Cardiac Failure: Dr. Abdul Ghani WaseemDocument33 pagesCardiac Failure: Dr. Abdul Ghani WaseemFarwaNo ratings yet
- Heart FailureDocument47 pagesHeart Failureedry901No ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- CHF Blok KardiovaskularDocument39 pagesCHF Blok KardiovaskularAnonymous Cz5xlxyU9VNo ratings yet
- Post Op Care PH Yogya-Ok - SipDocument29 pagesPost Op Care PH Yogya-Ok - SipTaufik KurniawanNo ratings yet
- Pathophys CHFDocument2 pagesPathophys CHFjayembee5308No ratings yet
- Cardiac Failure: Definition: Compensatory Changes in Heart FailureDocument5 pagesCardiac Failure: Definition: Compensatory Changes in Heart FailureMatyie SmkasNo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Chronic Congestive Heart FailureDocument10 pagesChronic Congestive Heart FailureEllappa GhanthanNo ratings yet
- Cardiovascular HO Final GROUP2Document72 pagesCardiovascular HO Final GROUP2Siraj ShiferawNo ratings yet
- MDSC 3311 PBL 1 (Without Group)Document5 pagesMDSC 3311 PBL 1 (Without Group)joshy221196No ratings yet
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaNo ratings yet
- Heart Failure - Practice Essentials, Background, PathophysiologyDocument15 pagesHeart Failure - Practice Essentials, Background, PathophysiologyAizel ManiagoNo ratings yet
- Congestive Heart FailureDocument6 pagesCongestive Heart Failureseigelystic100% (1)
- CardioDocument9 pagesCardioVirgilio Reyes ManuelNo ratings yet
- Clinical PresentationsDocument37 pagesClinical PresentationsJim Christian EllaserNo ratings yet
- CHFDocument22 pagesCHFshazia kaziNo ratings yet
- Heart Failure - Practice Essentials, Background, PathophysiologyDocument17 pagesHeart Failure - Practice Essentials, Background, PathophysiologyAshutosh SinghNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Heart FailureDocument8 pagesHeart FailureSophia MarieNo ratings yet
- An Unusual, Reversible Cause of Acute High-Outpout HFDocument5 pagesAn Unusual, Reversible Cause of Acute High-Outpout HFPeter Albeiro Falla CortesNo ratings yet
- Chronic Heart FailureDocument11 pagesChronic Heart FailurelaydyNo ratings yet
- ThiroidDocument9 pagesThiroidAhmed EmadNo ratings yet
- Congestive Heart FailureDocument42 pagesCongestive Heart FailureApriany Cordias Arlita SilalahiNo ratings yet
- Heart Failure: Dr. Andika Sitepu, SPJPDocument48 pagesHeart Failure: Dr. Andika Sitepu, SPJPWi KuNo ratings yet
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasNo ratings yet
- Thursday Nov 3rd - BayehDocument12 pagesThursday Nov 3rd - BayehFatima MaazNo ratings yet
- ShockDocument14 pagesShockNatia UtmelidzeNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart Failurelolo0880No ratings yet
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument48 pagesHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanAlbert SitepuNo ratings yet
- Lec 4Document9 pagesLec 4fbbqbcht6yNo ratings yet
- Acute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihaDocument98 pagesAcute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihablackcatNo ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Congestive Heart Failure FileDocument31 pagesCongestive Heart Failure FileAbas AhmedNo ratings yet
- Kuliah Pakar HF FKUMMDocument46 pagesKuliah Pakar HF FKUMMOkta Dwi Kusuma AyuNo ratings yet
- Acute Heart FailureDocument71 pagesAcute Heart FailureVivek Anandan100% (1)
- Decreased Cardiac OutputDocument9 pagesDecreased Cardiac OutputRae AnnNo ratings yet
- DIPIRO Gagal GinjalDocument19 pagesDIPIRO Gagal Ginjalselfa louhenapessyNo ratings yet
- Heart FailureDocument22 pagesHeart FailureYoussef MansourNo ratings yet
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanNo ratings yet
- Pharmacotherapy of Heart FailureDocument17 pagesPharmacotherapy of Heart FailurelisaNo ratings yet
- Dr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangDocument62 pagesDr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangKamelia MarcshendaNo ratings yet
- Falla Cardiaca ReviewDocument9 pagesFalla Cardiaca ReviewYasmin CarhuamacaNo ratings yet
- Unit II CVD Spring 2014-Ch 27Document63 pagesUnit II CVD Spring 2014-Ch 27Glory MimiNo ratings yet
- KP 2.5.5.1 Gagal Jantung KronikDocument39 pagesKP 2.5.5.1 Gagal Jantung Kronikayam kecapNo ratings yet
- CHFDocument35 pagesCHFireneNo ratings yet
- Heart FailureDocument4 pagesHeart FailureFaizan AbbasiNo ratings yet
- Essential Heart FailureDocument24 pagesEssential Heart FailuredeffyNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- SP 16 Week 5 Class 7 Bleeding in Late PregnancyDocument33 pagesSP 16 Week 5 Class 7 Bleeding in Late PregnancyGlory MimiNo ratings yet
- Addictive DisordersDocument117 pagesAddictive DisordersGlory MimiNo ratings yet
- SP 16 Week 5 Class 7 Bleeding in Late PregnancyDocument33 pagesSP 16 Week 5 Class 7 Bleeding in Late PregnancyGlory MimiNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- Schizophrenia Other Psychotic DisorderDocument57 pagesSchizophrenia Other Psychotic DisorderGlory MimiNo ratings yet
- AntipsychoticsDocument36 pagesAntipsychoticsGlory MimiNo ratings yet
- Week 10 Class 15 Preterm Labor With AnswersDocument29 pagesWeek 10 Class 15 Preterm Labor With AnswersGlory MimiNo ratings yet
- Chapter 52 Endocrine Disorders Unit 1Document55 pagesChapter 52 Endocrine Disorders Unit 1Glory Mimi100% (1)
- Week 10 Class 15 Intrapartum Complications With AnswersDocument55 pagesWeek 10 Class 15 Intrapartum Complications With AnswersGlory MimiNo ratings yet
- Chapter 51 Unit I Diabetes Mellitus-1Document70 pagesChapter 51 Unit I Diabetes Mellitus-1Glory MimiNo ratings yet
- Milieu MGT & Group TherapyDocument28 pagesMilieu MGT & Group TherapyGlory MimiNo ratings yet
- AtireviewDocument163 pagesAtireviewGlory Mimi0% (1)
- Unit I Scope and Standards of Med-Surg Nursing PracticeDocument9 pagesUnit I Scope and Standards of Med-Surg Nursing PracticeGlory Mimi100% (1)
- Chapter 17 Unit IDocument23 pagesChapter 17 Unit IGlory MimiNo ratings yet
- Chapter 13 Unit 1 Fluid and ElectrolytesDocument59 pagesChapter 13 Unit 1 Fluid and ElectrolytesGlory MimiNo ratings yet
- Cannibalism British English Teacher BWDocument11 pagesCannibalism British English Teacher BWDIONELIO MORENONo ratings yet
- Comparing Homatropine and Atropine in Pediatric Cycloplegic RefractionsDocument6 pagesComparing Homatropine and Atropine in Pediatric Cycloplegic RefractionsDwi Yuli YantoNo ratings yet
- UNAS B.inggrisDocument6 pagesUNAS B.inggrisintan kartikaNo ratings yet
- CHAPTER 6 Workplace Environment and ErgonomicsDocument30 pagesCHAPTER 6 Workplace Environment and Ergonomicsadlirazin24No ratings yet
- NHAI Recruitment 2022 Notification and FormDocument30 pagesNHAI Recruitment 2022 Notification and FormVikas SharmaNo ratings yet
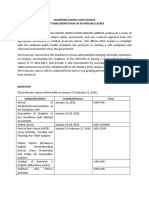
- Philippine Science High School Pilot Implementation of In-Person ClassesDocument5 pagesPhilippine Science High School Pilot Implementation of In-Person ClassesJonathan AladinNo ratings yet
- 205 Câu Hỏi Ngữ Pháp Trọng Điểm Trước Kì Thi Tốt Nghiệp THPT 2023Document12 pages205 Câu Hỏi Ngữ Pháp Trọng Điểm Trước Kì Thi Tốt Nghiệp THPT 2023leeyangmin28No ratings yet
- Advanced Trauma Life Support (Atls) : DR Eko Setiawan, SpotDocument67 pagesAdvanced Trauma Life Support (Atls) : DR Eko Setiawan, Spotyuliana khairiNo ratings yet
- q4sgc Medical Laboratory Science Review 4th EditionDocument632 pagesq4sgc Medical Laboratory Science Review 4th EditionAlexandr Trotsky0% (1)
- Clinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDateDocument16 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDatePablo ZeregaNo ratings yet
- Rechamp Gold Tablet Is A Unique Combination of Benfothiamine With MethylcobalaminDocument20 pagesRechamp Gold Tablet Is A Unique Combination of Benfothiamine With MethylcobalaminRoking KumarNo ratings yet
- Thesis Topics in EndodonticsDocument7 pagesThesis Topics in EndodonticsPapersHelpCanada100% (2)
- Surgery III MCQS 2023Document4 pagesSurgery III MCQS 2023mariam100% (1)
- (Code No. 044) : Term - IDocument6 pages(Code No. 044) : Term - IA KumarNo ratings yet
- Banana Nutrition Health BenefitsDocument9 pagesBanana Nutrition Health BenefitsUmar PervezNo ratings yet
- Drugs Affecting The Body SystemDocument3 pagesDrugs Affecting The Body SystemKhzNo ratings yet
- Lecture 2 PH & BUFFERSDocument56 pagesLecture 2 PH & BUFFERSJosephNo ratings yet
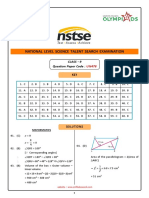
- CL 9 Nstse 2022 Paper 478 KeyDocument7 pagesCL 9 Nstse 2022 Paper 478 KeyVilas DewadeNo ratings yet
- Shinrin-Yoku Forest Bathing and Nature Therapy A S PDFDocument37 pagesShinrin-Yoku Forest Bathing and Nature Therapy A S PDFLaimis MotuzaNo ratings yet
- Nervous System WorksheetDocument3 pagesNervous System WorksheetaNo ratings yet
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsAulia RahmanNo ratings yet
- Gfad 118Document10 pagesGfad 118pepegiovannyNo ratings yet
- Siddhis PowweerDocument16 pagesSiddhis PowweerWilliam NormanNo ratings yet
- 9.3B The Baltimore Virus Classification - Biology LibreTextsDocument2 pages9.3B The Baltimore Virus Classification - Biology LibreTextsr60852009No ratings yet
- RyaltrisDocument6 pagesRyaltrisNaveen RaghavanNo ratings yet
- Programmable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7Document28 pagesProgrammable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7vin.vinylNo ratings yet






































































































Download as ppt, pdf, or txt
You might also like
- 1 Clinical Veterinary Advisor - Dogs and Cats 1-100 - RemovedDocument49 pages1 Clinical Veterinary Advisor - Dogs and Cats 1-100 - RemovedArieromNo ratings yet
- Treatment Planning Functional OcclusionDocument8 pagesTreatment Planning Functional OcclusionLandon Allen100% (1)
- 4.heart Failure HandoutDocument108 pages4.heart Failure HandoutGetachewNo ratings yet
- Final NTSB Report On Lockhart CrashDocument65 pagesFinal NTSB Report On Lockhart CrashAnonymous QUzIACmcB100% (1)
- Lyn Watson Level TwoDocument4 pagesLyn Watson Level TwoAlastair HarrisNo ratings yet
- Congestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho StudentsDocument27 pagesCongestive Heart Failure: Mulualem W.MD Dmu, Department of Internal Medicine For Ho Studentsmuluneh birhaneNo ratings yet
- Heart To HeartDocument110 pagesHeart To HeartmahyorwaNo ratings yet
- Heart FailureDocument52 pagesHeart Failurerania salsabilaNo ratings yet
- Congestive Heart Failure: Elias S. (MD+) March 2015 DBUDocument35 pagesCongestive Heart Failure: Elias S. (MD+) March 2015 DBUkikiNo ratings yet
- Sinaia 2 Oct 2014 - Final-Acute Heart FailureDocument285 pagesSinaia 2 Oct 2014 - Final-Acute Heart FailureBogdanel MihaiNo ratings yet
- Congestive Heart FailureDocument28 pagesCongestive Heart Failuresarguss1480% (5)
- Acute Heart FailureDocument18 pagesAcute Heart FailureGeorge GeorgeNo ratings yet
- Congestive Heart FailureDocument39 pagesCongestive Heart FailureEthiopia TekdemNo ratings yet
- Cardiac Failure: Dr. Abdul Ghani WaseemDocument33 pagesCardiac Failure: Dr. Abdul Ghani WaseemFarwaNo ratings yet
- Heart FailureDocument47 pagesHeart Failureedry901No ratings yet
- Pedal EdemaDocument45 pagesPedal Edemafirdaushassan2112No ratings yet
- Braunwald Lecture Series #2Document33 pagesBraunwald Lecture Series #2usfcards100% (2)
- CHF Blok KardiovaskularDocument39 pagesCHF Blok KardiovaskularAnonymous Cz5xlxyU9VNo ratings yet
- Post Op Care PH Yogya-Ok - SipDocument29 pagesPost Op Care PH Yogya-Ok - SipTaufik KurniawanNo ratings yet
- Pathophys CHFDocument2 pagesPathophys CHFjayembee5308No ratings yet
- Cardiac Failure: Definition: Compensatory Changes in Heart FailureDocument5 pagesCardiac Failure: Definition: Compensatory Changes in Heart FailureMatyie SmkasNo ratings yet
- Congestive Heart Failure ReportDocument6 pagesCongestive Heart Failure ReportSunshine_Bacla_4275100% (1)
- Chronic Congestive Heart FailureDocument10 pagesChronic Congestive Heart FailureEllappa GhanthanNo ratings yet
- Cardiovascular HO Final GROUP2Document72 pagesCardiovascular HO Final GROUP2Siraj ShiferawNo ratings yet
- MDSC 3311 PBL 1 (Without Group)Document5 pagesMDSC 3311 PBL 1 (Without Group)joshy221196No ratings yet
- Systolic Dysfunction:: Types of Heart FailureDocument13 pagesSystolic Dysfunction:: Types of Heart FailureElisabeth F. OjhaNo ratings yet
- Heart Failure - Practice Essentials, Background, PathophysiologyDocument15 pagesHeart Failure - Practice Essentials, Background, PathophysiologyAizel ManiagoNo ratings yet
- Congestive Heart FailureDocument6 pagesCongestive Heart Failureseigelystic100% (1)
- CardioDocument9 pagesCardioVirgilio Reyes ManuelNo ratings yet
- Clinical PresentationsDocument37 pagesClinical PresentationsJim Christian EllaserNo ratings yet
- CHFDocument22 pagesCHFshazia kaziNo ratings yet
- Heart Failure - Practice Essentials, Background, PathophysiologyDocument17 pagesHeart Failure - Practice Essentials, Background, PathophysiologyAshutosh SinghNo ratings yet
- Cardio Notes, Heart FailureDocument17 pagesCardio Notes, Heart FailureJoy DunwanNo ratings yet
- Heart FailureDocument8 pagesHeart FailureSophia MarieNo ratings yet
- An Unusual, Reversible Cause of Acute High-Outpout HFDocument5 pagesAn Unusual, Reversible Cause of Acute High-Outpout HFPeter Albeiro Falla CortesNo ratings yet
- Chronic Heart FailureDocument11 pagesChronic Heart FailurelaydyNo ratings yet
- ThiroidDocument9 pagesThiroidAhmed EmadNo ratings yet
- Congestive Heart FailureDocument42 pagesCongestive Heart FailureApriany Cordias Arlita SilalahiNo ratings yet
- Heart Failure: Dr. Andika Sitepu, SPJPDocument48 pagesHeart Failure: Dr. Andika Sitepu, SPJPWi KuNo ratings yet
- Heart Failure and ShockDocument34 pagesHeart Failure and Shockfrenee aradanasNo ratings yet
- Thursday Nov 3rd - BayehDocument12 pagesThursday Nov 3rd - BayehFatima MaazNo ratings yet
- ShockDocument14 pagesShockNatia UtmelidzeNo ratings yet
- Congestive Heart FailureDocument14 pagesCongestive Heart Failurelolo0880No ratings yet
- Heart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanDocument48 pagesHeart Failure: Departemen Kardiologi FK USU RSUP. H. Adam Malik MedanAlbert SitepuNo ratings yet
- Lec 4Document9 pagesLec 4fbbqbcht6yNo ratings yet
- Acute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihaDocument98 pagesAcute & Chronic Heart Failure: Dr. Nurkhalis, SPJP, FihablackcatNo ratings yet
- Cardiology Notes by Wasim AhmadDocument28 pagesCardiology Notes by Wasim AhmadAshna moeenNo ratings yet
- Congestive Heart Failure FileDocument31 pagesCongestive Heart Failure FileAbas AhmedNo ratings yet
- Kuliah Pakar HF FKUMMDocument46 pagesKuliah Pakar HF FKUMMOkta Dwi Kusuma AyuNo ratings yet
- Acute Heart FailureDocument71 pagesAcute Heart FailureVivek Anandan100% (1)
- Decreased Cardiac OutputDocument9 pagesDecreased Cardiac OutputRae AnnNo ratings yet
- DIPIRO Gagal GinjalDocument19 pagesDIPIRO Gagal Ginjalselfa louhenapessyNo ratings yet
- Heart FailureDocument22 pagesHeart FailureYoussef MansourNo ratings yet
- Congestive Cardiac FailureDocument38 pagesCongestive Cardiac FailureSalman KhanNo ratings yet
- Pharmacotherapy of Heart FailureDocument17 pagesPharmacotherapy of Heart FailurelisaNo ratings yet
- Dr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangDocument62 pagesDr. Az Rifki, Span - Kic Departemen Anestesiologi Dan Reanimasi Rsi Siti Rahmah/Fk-Fkg Universitas Baiturrahmah PadangKamelia MarcshendaNo ratings yet
- Falla Cardiaca ReviewDocument9 pagesFalla Cardiaca ReviewYasmin CarhuamacaNo ratings yet
- Unit II CVD Spring 2014-Ch 27Document63 pagesUnit II CVD Spring 2014-Ch 27Glory MimiNo ratings yet
- KP 2.5.5.1 Gagal Jantung KronikDocument39 pagesKP 2.5.5.1 Gagal Jantung Kronikayam kecapNo ratings yet
- CHFDocument35 pagesCHFireneNo ratings yet
- Heart FailureDocument4 pagesHeart FailureFaizan AbbasiNo ratings yet
- Essential Heart FailureDocument24 pagesEssential Heart FailuredeffyNo ratings yet
- Cardiac Care and COVID-19: Perspectives in Medical PracticeFrom EverandCardiac Care and COVID-19: Perspectives in Medical PracticeNo ratings yet
- SP 16 Week 5 Class 7 Bleeding in Late PregnancyDocument33 pagesSP 16 Week 5 Class 7 Bleeding in Late PregnancyGlory MimiNo ratings yet
- Addictive DisordersDocument117 pagesAddictive DisordersGlory MimiNo ratings yet
- SP 16 Week 5 Class 7 Bleeding in Late PregnancyDocument33 pagesSP 16 Week 5 Class 7 Bleeding in Late PregnancyGlory MimiNo ratings yet
- Treatment Modalities For Mood DisordersDocument55 pagesTreatment Modalities For Mood DisordersGlory MimiNo ratings yet
- Schizophrenia Other Psychotic DisorderDocument57 pagesSchizophrenia Other Psychotic DisorderGlory MimiNo ratings yet
- AntipsychoticsDocument36 pagesAntipsychoticsGlory MimiNo ratings yet
- Week 10 Class 15 Preterm Labor With AnswersDocument29 pagesWeek 10 Class 15 Preterm Labor With AnswersGlory MimiNo ratings yet
- Chapter 52 Endocrine Disorders Unit 1Document55 pagesChapter 52 Endocrine Disorders Unit 1Glory Mimi100% (1)
- Week 10 Class 15 Intrapartum Complications With AnswersDocument55 pagesWeek 10 Class 15 Intrapartum Complications With AnswersGlory MimiNo ratings yet
- Chapter 51 Unit I Diabetes Mellitus-1Document70 pagesChapter 51 Unit I Diabetes Mellitus-1Glory MimiNo ratings yet
- Milieu MGT & Group TherapyDocument28 pagesMilieu MGT & Group TherapyGlory MimiNo ratings yet
- AtireviewDocument163 pagesAtireviewGlory Mimi0% (1)
- Unit I Scope and Standards of Med-Surg Nursing PracticeDocument9 pagesUnit I Scope and Standards of Med-Surg Nursing PracticeGlory Mimi100% (1)
- Chapter 17 Unit IDocument23 pagesChapter 17 Unit IGlory MimiNo ratings yet
- Chapter 13 Unit 1 Fluid and ElectrolytesDocument59 pagesChapter 13 Unit 1 Fluid and ElectrolytesGlory MimiNo ratings yet
- Cannibalism British English Teacher BWDocument11 pagesCannibalism British English Teacher BWDIONELIO MORENONo ratings yet
- Comparing Homatropine and Atropine in Pediatric Cycloplegic RefractionsDocument6 pagesComparing Homatropine and Atropine in Pediatric Cycloplegic RefractionsDwi Yuli YantoNo ratings yet
- UNAS B.inggrisDocument6 pagesUNAS B.inggrisintan kartikaNo ratings yet
- CHAPTER 6 Workplace Environment and ErgonomicsDocument30 pagesCHAPTER 6 Workplace Environment and Ergonomicsadlirazin24No ratings yet
- NHAI Recruitment 2022 Notification and FormDocument30 pagesNHAI Recruitment 2022 Notification and FormVikas SharmaNo ratings yet
- Philippine Science High School Pilot Implementation of In-Person ClassesDocument5 pagesPhilippine Science High School Pilot Implementation of In-Person ClassesJonathan AladinNo ratings yet
- 205 Câu Hỏi Ngữ Pháp Trọng Điểm Trước Kì Thi Tốt Nghiệp THPT 2023Document12 pages205 Câu Hỏi Ngữ Pháp Trọng Điểm Trước Kì Thi Tốt Nghiệp THPT 2023leeyangmin28No ratings yet
- Advanced Trauma Life Support (Atls) : DR Eko Setiawan, SpotDocument67 pagesAdvanced Trauma Life Support (Atls) : DR Eko Setiawan, Spotyuliana khairiNo ratings yet
- q4sgc Medical Laboratory Science Review 4th EditionDocument632 pagesq4sgc Medical Laboratory Science Review 4th EditionAlexandr Trotsky0% (1)
- Clinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDateDocument16 pagesClinical Manifestations, Pathologic Features, and Diagnosis of Peripheral T Cell Lymphoma, Not Otherwise Specified - UpToDatePablo ZeregaNo ratings yet
- Rechamp Gold Tablet Is A Unique Combination of Benfothiamine With MethylcobalaminDocument20 pagesRechamp Gold Tablet Is A Unique Combination of Benfothiamine With MethylcobalaminRoking KumarNo ratings yet
- Thesis Topics in EndodonticsDocument7 pagesThesis Topics in EndodonticsPapersHelpCanada100% (2)
- Surgery III MCQS 2023Document4 pagesSurgery III MCQS 2023mariam100% (1)
- (Code No. 044) : Term - IDocument6 pages(Code No. 044) : Term - IA KumarNo ratings yet
- Banana Nutrition Health BenefitsDocument9 pagesBanana Nutrition Health BenefitsUmar PervezNo ratings yet
- Drugs Affecting The Body SystemDocument3 pagesDrugs Affecting The Body SystemKhzNo ratings yet
- Lecture 2 PH & BUFFERSDocument56 pagesLecture 2 PH & BUFFERSJosephNo ratings yet
- CL 9 Nstse 2022 Paper 478 KeyDocument7 pagesCL 9 Nstse 2022 Paper 478 KeyVilas DewadeNo ratings yet
- Shinrin-Yoku Forest Bathing and Nature Therapy A S PDFDocument37 pagesShinrin-Yoku Forest Bathing and Nature Therapy A S PDFLaimis MotuzaNo ratings yet
- Nervous System WorksheetDocument3 pagesNervous System WorksheetaNo ratings yet
- Blood Transfusion ProblemsDocument52 pagesBlood Transfusion ProblemsAulia RahmanNo ratings yet
- Gfad 118Document10 pagesGfad 118pepegiovannyNo ratings yet
- Siddhis PowweerDocument16 pagesSiddhis PowweerWilliam NormanNo ratings yet
- 9.3B The Baltimore Virus Classification - Biology LibreTextsDocument2 pages9.3B The Baltimore Virus Classification - Biology LibreTextsr60852009No ratings yet
- RyaltrisDocument6 pagesRyaltrisNaveen RaghavanNo ratings yet
- Programmable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7Document28 pagesProgrammable Protein Delivery With A Bacterial Contractile Injection System - s41586-023-05870-7vin.vinylNo ratings yet