Download as ppt, pdf, or txt
You might also like
- Snake Bite Ppt-1Document53 pagesSnake Bite Ppt-1Arjit Bhushan100% (2)
- Snake Bits: Introduced by D. Abdallah Abd El Rahman Ali MohammediaDocument17 pagesSnake Bits: Introduced by D. Abdallah Abd El Rahman Ali MohammediaSalah Elbadawy100% (1)
- Common Toxic Bites: Olowookere O.ODocument62 pagesCommon Toxic Bites: Olowookere O.OTheop AyodeleNo ratings yet
- Snakebite Poisoning Viva2019Document6 pagesSnakebite Poisoning Viva2019Meer HomerNo ratings yet
- Snake Bite ManagementDocument49 pagesSnake Bite ManagementChhabilal Bastola100% (1)
- Sarpa All BasicsDocument11 pagesSarpa All BasicsRavichandra MentheNo ratings yet
- MAKALAH Snake BiteDocument6 pagesMAKALAH Snake BiteMutiara YuliantikaNo ratings yet
- Snake Bite Management in Bangladesh 2Document66 pagesSnake Bite Management in Bangladesh 2taosifNo ratings yet
- Management of Snake Bite National Guideline 2014Document66 pagesManagement of Snake Bite National Guideline 2014jonmax86No ratings yet
- Snake Bite - Indian Guidelines and ProtocolDocument3 pagesSnake Bite - Indian Guidelines and ProtocolSushobhanSarkarNo ratings yet
- SNAKE BITE FOR GP DOKTER POST DR IsyaDocument50 pagesSNAKE BITE FOR GP DOKTER POST DR IsyaMuhammad Agung HidayatNo ratings yet
- Snake BiteDocument38 pagesSnake Biteehabahmad12365No ratings yet
- First Aid & Management of Snake BitesDocument38 pagesFirst Aid & Management of Snake BitesDeepak BenjaminNo ratings yet
- Snake Bites MainDocument6 pagesSnake Bites MainElvisNo ratings yet
- Snakebite Medan DR DickyDocument37 pagesSnakebite Medan DR Dickypuskesmas paparNo ratings yet
- Tatalaksana Gigitan Hewan BerbisaDocument73 pagesTatalaksana Gigitan Hewan BerbisaDenny Eka Putri PurwantoNo ratings yet
- Redback Spider FactsDocument3 pagesRedback Spider FactsPradeep WalaweNo ratings yet
- Animal Envenomation: Scorpion Sting and Snake BitesDocument49 pagesAnimal Envenomation: Scorpion Sting and Snake BitesRaymond ManjengwaNo ratings yet
- Snake Bite: Families of Venomous SnakesDocument4 pagesSnake Bite: Families of Venomous SnakesPeter AbikoyeNo ratings yet
- Community Health Nursing - 1 MahirDocument37 pagesCommunity Health Nursing - 1 MahirvhoramahirNo ratings yet
- Venomous Bites Stings and PoisoningDocument17 pagesVenomous Bites Stings and Poisoningdrheay100% (1)
- Snake Bite: DR - Vemuri ChaitanyaDocument54 pagesSnake Bite: DR - Vemuri ChaitanyaMutiara YuliantikaNo ratings yet
- Materi Dr. Tri Maharani PDFDocument53 pagesMateri Dr. Tri Maharani PDFgalon akuaNo ratings yet
- War Rell 2019Document22 pagesWar Rell 2019Yesid MedinaNo ratings yet
- 2010148newton 2Document2 pages2010148newton 2Fenty SuwidakNo ratings yet
- Snake BiteDocument46 pagesSnake Bitejerly lNo ratings yet
- Management of Snake Bite in India: Shibendu Ghosh, Prabuddha MukhopadhyayDocument6 pagesManagement of Snake Bite in India: Shibendu Ghosh, Prabuddha MukhopadhyaychandanNo ratings yet
- Ebola Haemorrhagic FeverDocument42 pagesEbola Haemorrhagic FeverDebraj BhattacharjeeNo ratings yet
- Tropmed - Lecture 4Document78 pagesTropmed - Lecture 4VerarisnaNo ratings yet
- Rabies 151018135758 Lva1 App6892 PDFDocument44 pagesRabies 151018135758 Lva1 App6892 PDFAna SismanNo ratings yet
- HIV InfectionDocument13 pagesHIV Infectionsun shineNo ratings yet
- Snake Bite: ManagementDocument77 pagesSnake Bite: ManagementSunnyEesuNo ratings yet
- 1 Snake BiteDocument8 pages1 Snake BiteMatthew Wei Hua CaiNo ratings yet
- Snake BiteDocument66 pagesSnake BiteedfZSEADFsfsafafNo ratings yet
- Update Manajemen Snakebite: Biodiversity of Indonesian SnakeDocument18 pagesUpdate Manajemen Snakebite: Biodiversity of Indonesian SnakeAndrianto AliongNo ratings yet
- Envenomation Snake BiteDocument39 pagesEnvenomation Snake BiteMeliani FranzNo ratings yet
- Snake Bite - Native British Species - 200123062646Document5 pagesSnake Bite - Native British Species - 200123062646Belal HasanNo ratings yet
- Animal Related Injury: Snake BiteDocument12 pagesAnimal Related Injury: Snake Bitemsah820No ratings yet
- FM Snake - Bite 16 12 14Document54 pagesFM Snake - Bite 16 12 14Endah Duii Utamee100% (1)
- Anjali Triathi BSC (H) Microbiology Department of Industrial Microbiology 16BSMBH012Document31 pagesAnjali Triathi BSC (H) Microbiology Department of Industrial Microbiology 16BSMBH012shravaniNo ratings yet
- Snake Bites: and Their TreatmentDocument15 pagesSnake Bites: and Their TreatmentRamakrishna JakkulaNo ratings yet
- Unit-3: Arthropods and StingsDocument18 pagesUnit-3: Arthropods and StingsDivithNo ratings yet
- Training CasesDocument8 pagesTraining CasesManisanthosh KumarNo ratings yet
- Snake BiteDocument82 pagesSnake Biteokeherawati21No ratings yet
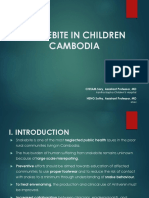
- Snakebite in Cambodia - 2021Document47 pagesSnakebite in Cambodia - 2021bo kongNo ratings yet
- Intrevenous TherapyDocument5 pagesIntrevenous TherapyCharles DoradoNo ratings yet
- Tetanus: Dr.I.SelvarajDocument47 pagesTetanus: Dr.I.SelvarajimyoongsNo ratings yet
- VaxiRab CME Slides - EnglishDocument40 pagesVaxiRab CME Slides - EnglishAnand VinayNo ratings yet
- Rabies: Clinical FeaturesDocument3 pagesRabies: Clinical FeaturessivaNo ratings yet
- API Snakebite ManagementDocument3 pagesAPI Snakebite Managementsyed aquibNo ratings yet
- RabiesDocument28 pagesRabiesrouhanbinrashidNo ratings yet
- Case Histories in PoisoningDocument28 pagesCase Histories in Poisoningzonia kilashNo ratings yet
- Foot and Mouth DiseaseDocument5 pagesFoot and Mouth Diseaseelvhynd beiNo ratings yet
- Aims of Anthrax LectureDocument25 pagesAims of Anthrax LectureSecret ManNo ratings yet
- Post Mortem Examination PDFDocument23 pagesPost Mortem Examination PDFFaizan AhmadNo ratings yet
- Rabies by DR Najeeb Memon PakistanDocument23 pagesRabies by DR Najeeb Memon Pakistanmnajeeb807196No ratings yet
- Bsn4a Group 4 Red Dog BitesDocument34 pagesBsn4a Group 4 Red Dog BitesNovie GarillosNo ratings yet
- Lap Kasus Listiana - Rev1Document6 pagesLap Kasus Listiana - Rev1Gunawan pnsNo ratings yet
- Snake Bite: Dr. Eman Alaa EldinDocument7 pagesSnake Bite: Dr. Eman Alaa EldinAbdelrhman AboodaNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
- Dental Anxiety Form 4 PDFDocument2 pagesDental Anxiety Form 4 PDFBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
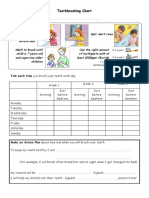
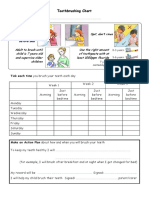
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
- Marine Refrigeration AND Air ConditioningDocument73 pagesMarine Refrigeration AND Air ConditioningBruno Manestar100% (2)
- HIRA of Batching Plant Erection.Document3 pagesHIRA of Batching Plant Erection.Gyanendra SrivastavaNo ratings yet
- Watts Zone Controls and Valves - 2Document16 pagesWatts Zone Controls and Valves - 2Sid KherNo ratings yet
- Molecular Orbital TheoryDocument17 pagesMolecular Orbital TheoryOmSilence2651No ratings yet
- Model ESFR-17 16.8 K-Factor Pendent Sprinkler Early Suppression, Fast Response General DescriptionDocument4 pagesModel ESFR-17 16.8 K-Factor Pendent Sprinkler Early Suppression, Fast Response General DescriptionJUANA MONSERRATE PARRALES PILAYNo ratings yet
- MTO MATERIAL OHL 20 KVDocument4 pagesMTO MATERIAL OHL 20 KVDacid ChalinkNo ratings yet
- 871 BookDocument4 pages871 Bookmurty99No ratings yet
- D5462 PDFDocument6 pagesD5462 PDFZamir Danilo Morera ForeroNo ratings yet
- First Floor: No. Location Area (M ) Cooling (Btu/h) Model (Daikin) Cap. (Btu/h) Type OtherDocument3 pagesFirst Floor: No. Location Area (M ) Cooling (Btu/h) Model (Daikin) Cap. (Btu/h) Type OtherIm ChinithNo ratings yet
- Sample Application For NCH Nomination On Province Reserved Seats 2017Document2 pagesSample Application For NCH Nomination On Province Reserved Seats 2017Tabib Afzaal Ahmad Virk100% (1)
- Aadhaar Enabled Public Distribution System - Aepds: Food and Consumer Protection Department Government of BiharDocument1 pageAadhaar Enabled Public Distribution System - Aepds: Food and Consumer Protection Department Government of BiharAnil SharmaNo ratings yet
- Safety Data Sheet: Armohib 31Document12 pagesSafety Data Sheet: Armohib 31Dr. Pushkar ShuklaNo ratings yet
- Functional Safety Embedded Systems: Integration of in The Development Process ofDocument34 pagesFunctional Safety Embedded Systems: Integration of in The Development Process ofAleksandar MilinkovicNo ratings yet
- Risk Assessment OF IODINE AND PROPANONE REACTIONDocument3 pagesRisk Assessment OF IODINE AND PROPANONE REACTIONelizabeth sonubiNo ratings yet
- Proposed Rule: Medicare: Electronic Prescription Drug Program E-PrescribingDocument20 pagesProposed Rule: Medicare: Electronic Prescription Drug Program E-PrescribingJustia.comNo ratings yet
- Divya Kit Online All ProductsDocument6 pagesDivya Kit Online All ProductsDivya KitNo ratings yet
- CA1 Online Class 2Document13 pagesCA1 Online Class 2kemerutNo ratings yet
- Grade 10 Relative ClauseDocument1 pageGrade 10 Relative ClauseMjoy PadayaoNo ratings yet
- Gea Fes, Inc.: 4 Models 50 - 300 HPDocument2 pagesGea Fes, Inc.: 4 Models 50 - 300 HPVadimNo ratings yet
- Letter Responding To Cosmopolis Fire Department Volunteer ResignationDocument2 pagesLetter Responding To Cosmopolis Fire Department Volunteer ResignationKING 5 NewsNo ratings yet
- Fall Arrest SystemDocument16 pagesFall Arrest SystemDragos VerdesNo ratings yet
- Domains Kingdoms and Hierarchy PDFDocument5 pagesDomains Kingdoms and Hierarchy PDFEj FerrerNo ratings yet
- Easy Go System by StorzDocument16 pagesEasy Go System by StorzKaustubh KeskarNo ratings yet
- BiologyDocument23 pagesBiologyDevendra AryaNo ratings yet
- Eaton - Internormen Wind Power SolutionsDocument12 pagesEaton - Internormen Wind Power SolutionsEaton FiltrationNo ratings yet
- Rojek Advance Solutions Employee HandbookDocument32 pagesRojek Advance Solutions Employee HandbookJämes ScarlétteNo ratings yet
- Compressed Air System Design, Operating and MaintenanceDocument29 pagesCompressed Air System Design, Operating and Maintenanceibrahim1961No ratings yet
- 718Document19 pages718shankerahulNo ratings yet
- Ecpg OrlapDocument258 pagesEcpg OrlapNoha Ibraheem HelmyNo ratings yet
- Warrenton Horse Show Program 2016Document36 pagesWarrenton Horse Show Program 2016Fauquier NowNo ratings yet