
Use of Antibiotics in Periodontal Therapy
Use of Antibiotics in Periodontal Therapy
You might also like
- SCID - Full InterviewDocument141 pagesSCID - Full InterviewCirtiu Dana92% (13)
- Vanders Human Physiology The Mechanisms of Body Function 15th Edition Widmaier Test BankDocument29 pagesVanders Human Physiology The Mechanisms of Body Function 15th Edition Widmaier Test BankDavidWardrcobi100% (15)
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Introduction To BiochemistryDocument122 pagesIntroduction To Biochemistryqwerty123100% (1)
- Antimicrobial DrugsDocument64 pagesAntimicrobial Drugsdr. khushboo singh100% (1)
- Chapter 7 RH Blood Group SystemDocument28 pagesChapter 7 RH Blood Group Systemschemology100% (2)
- Biology Notes For Unit 5Document84 pagesBiology Notes For Unit 5nhmerali7860% (1)
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)
- Principles of Antimicrobial TherapyDocument19 pagesPrinciples of Antimicrobial TherapyMERVENo ratings yet
- ChemotherapyDocument11 pagesChemotherapyJennifer DixonNo ratings yet
- Anti-Infectives and AntibioticsDocument38 pagesAnti-Infectives and AntibioticsKarel Lu0% (1)
- Antibiotic 1Document13 pagesAntibiotic 1ريدان عياشNo ratings yet
- AntibioticDocument84 pagesAntibioticDr. Kalavati PrajapatiNo ratings yet
- Pharma URO AminoglycosidesDocument8 pagesPharma URO AminoglycosidesHussein AlhaddadNo ratings yet
- AMINOGLYCOSIDESDocument45 pagesAMINOGLYCOSIDESAbdullah EmadNo ratings yet
- Buy The Book PDA DownloadDocument9 pagesBuy The Book PDA Downloadneilbert_jayNo ratings yet
- L16 Antibiotics - in - Oral - Maxillofacial - SurgeryDocument75 pagesL16 Antibiotics - in - Oral - Maxillofacial - SurgeryJu JuNo ratings yet
- ChemotherapyDocument58 pagesChemotherapyRakesh MahindraNo ratings yet
- Cirilo Albert Hicban RN, RM LecturerDocument50 pagesCirilo Albert Hicban RN, RM Lecturerrongan008No ratings yet
- AntibioticsDocument56 pagesAntibioticstintinNo ratings yet
- Antibiotics in Periodontics PerioDocument51 pagesAntibiotics in Periodontics PerioSiddhartha BanerjeeNo ratings yet
- AntibioticsDocument90 pagesAntibioticsArun MamachanNo ratings yet
- AminoglycosidesDocument36 pagesAminoglycosidesIqbal V MohammadNo ratings yet
- Antibiotics Used in Oral and Maxillofacial Surgery1Document38 pagesAntibiotics Used in Oral and Maxillofacial Surgery1mcshah19100% (1)
- AMINOGLYCOSIDEDocument18 pagesAMINOGLYCOSIDEVinayKumarNo ratings yet
- Antibacterials and AntibioticsDocument44 pagesAntibacterials and AntibioticsVallejo Taberna HannalieNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Aminoglycosides: Official Reprint From Uptodate ©2021 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument17 pagesAminoglycosides: Official Reprint From Uptodate ©2021 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedVanessa GomesNo ratings yet
- Nursing 3703 Pharmacology: Antimicrobials by Linda SelfDocument78 pagesNursing 3703 Pharmacology: Antimicrobials by Linda Selfdon yenNo ratings yet
- Antibiotics Resistance - 20WDocument24 pagesAntibiotics Resistance - 20WflubbybananaNo ratings yet
- PharmaDocument16 pagesPharmaPaula Grace MorfeNo ratings yet
- DR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtDocument45 pagesDR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtalyaNo ratings yet
- Antibacterial Drugs: B.K. SatriyasaDocument56 pagesAntibacterial Drugs: B.K. SatriyasaVicNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- Microbiology Assignmentt TradeDocument14 pagesMicrobiology Assignmentt TradeADITYAROOP PATHAKNo ratings yet
- DP On AglDocument12 pagesDP On AglDeepikaNo ratings yet
- AntibioticsDocument30 pagesAntibioticsRoza RahbeniNo ratings yet
- NotesDocument9 pagesNotesVivianNo ratings yet
- Antibiotics & Antibiotic ResistanceDocument53 pagesAntibiotics & Antibiotic ResistanceLeenoos RayapanNo ratings yet
- Microbiology Assignmentt xxx123Document16 pagesMicrobiology Assignmentt xxx123ADITYAROOP PATHAKNo ratings yet
- Pharmacology: Fast and Dirty Board ReviewDocument7 pagesPharmacology: Fast and Dirty Board ReviewRochelleth7278No ratings yet
- Title: meropenem: Student Name: طباس ميرك ليلخDocument6 pagesTitle: meropenem: Student Name: طباس ميرك ليلخKha KinNo ratings yet
- Antibiotik Imipenem Golongan CarbapenemDocument5 pagesAntibiotik Imipenem Golongan Carbapenemabam_abamNo ratings yet
- Antimicrobial DrugsDocument63 pagesAntimicrobial DrugsRonalyn UgatNo ratings yet
- 2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Document28 pages2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Leena AlateeqNo ratings yet
- Chemotherapeutic DrugsDocument122 pagesChemotherapeutic Drugsdex7reme100% (1)
- Aminoglycosides 23099Document27 pagesAminoglycosides 23099TES SENNo ratings yet
- 5 AminoglycosidesDocument7 pages5 AminoglycosidesNashat SaadiNo ratings yet
- Antibiotics 3: (Year 1 Term 2) (Session 2014-2015) by Professor Dr. Naeem Hasan Khan 17.04.2015Document35 pagesAntibiotics 3: (Year 1 Term 2) (Session 2014-2015) by Professor Dr. Naeem Hasan Khan 17.04.2015ArunaNo ratings yet
- Pharmacology AntibioticsDocument70 pagesPharmacology Antibioticsmaggie100% (1)
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Monobactams & CarbapenemsDocument41 pagesMonobactams & CarbapenemsHussein AlhaddadNo ratings yet
- Antibiotic's Interactions in GynecologyDocument26 pagesAntibiotic's Interactions in Gynecologyمحمد قاسمNo ratings yet
- Pharmacology-Antibiotic 2021Document52 pagesPharmacology-Antibiotic 2021Ngọc VânNo ratings yet
- Drug Resistance Pharmacology Lecture Lecture Series 2019Document23 pagesDrug Resistance Pharmacology Lecture Lecture Series 2019temitopeNo ratings yet
- Microbiology AssignmentDocument18 pagesMicrobiology AssignmentADITYAROOP PATHAKNo ratings yet
- ChemotherapyDocument66 pagesChemotherapyElias HaimanotNo ratings yet
- Antimicrobials Complete by DR - Mayur Sayta M 91 PDFDocument86 pagesAntimicrobials Complete by DR - Mayur Sayta M 91 PDFRuthvi Jain100% (1)
- Chapter 9 Surgical Infections and Antibiotic SelectionDocument42 pagesChapter 9 Surgical Infections and Antibiotic SelectionSteven Mark MananguNo ratings yet
- 13 - Antibiotic III Nalidixic AcidDocument7 pages13 - Antibiotic III Nalidixic AcidMoataz TrabehNo ratings yet
- AntibioticsDocument63 pagesAntibioticsSahin mollickNo ratings yet
- Antimicrobial TherapyDocument18 pagesAntimicrobial TherapysaifNo ratings yet
- Pharmacology Powerpoint - AntibioticsDocument90 pagesPharmacology Powerpoint - AntibioticsAdminNo ratings yet
- Anti - TB DrugsupdatedDocument35 pagesAnti - TB DrugsupdatedgNo ratings yet
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
- Dental Anxiety Form 4 PDFDocument2 pagesDental Anxiety Form 4 PDFBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
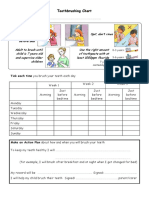
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
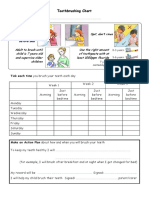
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
- Gastro highlightCHAPTER1Document12 pagesGastro highlightCHAPTER1Lovely CruzxNo ratings yet
- 7JC - Early TreatmentDocument18 pages7JC - Early Treatmentanon_137544084No ratings yet
- Orbans Oral Histology Embryology 15Th Edition G S Kumar Full ChapterDocument67 pagesOrbans Oral Histology Embryology 15Th Edition G S Kumar Full Chaptersimon.sheneman371100% (5)
- 3rd YrMedical Surgical NursingDocument24 pages3rd YrMedical Surgical Nursingpunam todkarNo ratings yet
- Paracetamol Poisoning: G. Rajapandi 521625111 Final MbbsDocument18 pagesParacetamol Poisoning: G. Rajapandi 521625111 Final MbbsAntony PrakashNo ratings yet
- Diuretic Activity of S.officinarumDocument42 pagesDiuretic Activity of S.officinarumPalaksha M.N.No ratings yet
- A Short History of VaccinationDocument16 pagesA Short History of VaccinationAlejandro MotoliníaNo ratings yet
- SRS Kidney - 2016BDocument3 pagesSRS Kidney - 2016ByayayanizaNo ratings yet
- Hematological Emergencies in Dental Office by DR Khalid Hassan AlhazmiDocument13 pagesHematological Emergencies in Dental Office by DR Khalid Hassan Alhazmiamoon almNo ratings yet
- CHN ExamDocument30 pagesCHN ExamKhei Laqui SN100% (3)
- A Thing of Nothing. The Catastrophic Body in HamletDocument19 pagesA Thing of Nothing. The Catastrophic Body in HamletMarialena MarialenakiNo ratings yet
- Difficult Airway Management: 2009 Adrian SieberhagenDocument26 pagesDifficult Airway Management: 2009 Adrian Sieberhagendpeka dpekaNo ratings yet
- Piggery InvestmentDocument9 pagesPiggery InvestmentAndile Ntuli100% (1)
- Renal Fabs Post TestDocument3 pagesRenal Fabs Post Testlorelyn corpuzNo ratings yet
- CH 26 - The FungiDocument29 pagesCH 26 - The FungiBronwyn JuliusNo ratings yet
- Learning Continuity Plan For The Limited Face To Face ClassesDocument41 pagesLearning Continuity Plan For The Limited Face To Face ClassesHaimen BuisanNo ratings yet
- English: Learning Activity Sheets Module 1: What Composes MeDocument12 pagesEnglish: Learning Activity Sheets Module 1: What Composes MeGe PebresNo ratings yet
- chn-1 InfosheetDocument71 pageschn-1 InfosheetAMIR LADJANo ratings yet
- Clinical Report FinalDocument45 pagesClinical Report FinalBENJAMIN MAWUENYEGAHNo ratings yet
- 132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SDocument4 pages132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SUsman AR VainceNo ratings yet
- PDF Copy Haematology Laboratory Manual Cls 241 PDFDocument70 pagesPDF Copy Haematology Laboratory Manual Cls 241 PDFKahina Ould TalebNo ratings yet
- Unit Test 8B: Are Girls Better at Cooking?Document5 pagesUnit Test 8B: Are Girls Better at Cooking?Ana TodorovićNo ratings yet
- Anavar (Oxandrolone)Document26 pagesAnavar (Oxandrolone)illicitdrugsNo ratings yet
- MemoryDocument11 pagesMemorydkrms DNo ratings yet
- New York Health Welcomes Jay B. Adlersberg, M.D.Document2 pagesNew York Health Welcomes Jay B. Adlersberg, M.D.PR.comNo ratings yet
















































































































Download as pptx, pdf, or txt
You might also like
- SCID - Full InterviewDocument141 pagesSCID - Full InterviewCirtiu Dana92% (13)
- Vanders Human Physiology The Mechanisms of Body Function 15th Edition Widmaier Test BankDocument29 pagesVanders Human Physiology The Mechanisms of Body Function 15th Edition Widmaier Test BankDavidWardrcobi100% (15)
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Introduction To BiochemistryDocument122 pagesIntroduction To Biochemistryqwerty123100% (1)
- Antimicrobial DrugsDocument64 pagesAntimicrobial Drugsdr. khushboo singh100% (1)
- Chapter 7 RH Blood Group SystemDocument28 pagesChapter 7 RH Blood Group Systemschemology100% (2)
- Biology Notes For Unit 5Document84 pagesBiology Notes For Unit 5nhmerali7860% (1)
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)
- Principles of Antimicrobial TherapyDocument19 pagesPrinciples of Antimicrobial TherapyMERVENo ratings yet
- ChemotherapyDocument11 pagesChemotherapyJennifer DixonNo ratings yet
- Anti-Infectives and AntibioticsDocument38 pagesAnti-Infectives and AntibioticsKarel Lu0% (1)
- Antibiotic 1Document13 pagesAntibiotic 1ريدان عياشNo ratings yet
- AntibioticDocument84 pagesAntibioticDr. Kalavati PrajapatiNo ratings yet
- Pharma URO AminoglycosidesDocument8 pagesPharma URO AminoglycosidesHussein AlhaddadNo ratings yet
- AMINOGLYCOSIDESDocument45 pagesAMINOGLYCOSIDESAbdullah EmadNo ratings yet
- Buy The Book PDA DownloadDocument9 pagesBuy The Book PDA Downloadneilbert_jayNo ratings yet
- L16 Antibiotics - in - Oral - Maxillofacial - SurgeryDocument75 pagesL16 Antibiotics - in - Oral - Maxillofacial - SurgeryJu JuNo ratings yet
- ChemotherapyDocument58 pagesChemotherapyRakesh MahindraNo ratings yet
- Cirilo Albert Hicban RN, RM LecturerDocument50 pagesCirilo Albert Hicban RN, RM Lecturerrongan008No ratings yet
- AntibioticsDocument56 pagesAntibioticstintinNo ratings yet
- Antibiotics in Periodontics PerioDocument51 pagesAntibiotics in Periodontics PerioSiddhartha BanerjeeNo ratings yet
- AntibioticsDocument90 pagesAntibioticsArun MamachanNo ratings yet
- AminoglycosidesDocument36 pagesAminoglycosidesIqbal V MohammadNo ratings yet
- Antibiotics Used in Oral and Maxillofacial Surgery1Document38 pagesAntibiotics Used in Oral and Maxillofacial Surgery1mcshah19100% (1)
- AMINOGLYCOSIDEDocument18 pagesAMINOGLYCOSIDEVinayKumarNo ratings yet
- Antibacterials and AntibioticsDocument44 pagesAntibacterials and AntibioticsVallejo Taberna HannalieNo ratings yet
- Week 3 & 4 AntimicrobialsDocument120 pagesWeek 3 & 4 AntimicrobialsQuerubin DandoyNo ratings yet
- Aminoglycosides: Official Reprint From Uptodate ©2021 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedDocument17 pagesAminoglycosides: Official Reprint From Uptodate ©2021 Uptodate, Inc. And/Or Its Affiliates. All Rights ReservedVanessa GomesNo ratings yet
- Nursing 3703 Pharmacology: Antimicrobials by Linda SelfDocument78 pagesNursing 3703 Pharmacology: Antimicrobials by Linda Selfdon yenNo ratings yet
- Antibiotics Resistance - 20WDocument24 pagesAntibiotics Resistance - 20WflubbybananaNo ratings yet
- PharmaDocument16 pagesPharmaPaula Grace MorfeNo ratings yet
- DR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtDocument45 pagesDR Retno Budiarti, DR., M.Kes Microbiology Department FK UhtalyaNo ratings yet
- Antibacterial Drugs: B.K. SatriyasaDocument56 pagesAntibacterial Drugs: B.K. SatriyasaVicNo ratings yet
- Lac 10&11 PPTDocument16 pagesLac 10&11 PPTRaghdaNo ratings yet
- Microbiology Assignmentt TradeDocument14 pagesMicrobiology Assignmentt TradeADITYAROOP PATHAKNo ratings yet
- DP On AglDocument12 pagesDP On AglDeepikaNo ratings yet
- AntibioticsDocument30 pagesAntibioticsRoza RahbeniNo ratings yet
- NotesDocument9 pagesNotesVivianNo ratings yet
- Antibiotics & Antibiotic ResistanceDocument53 pagesAntibiotics & Antibiotic ResistanceLeenoos RayapanNo ratings yet
- Microbiology Assignmentt xxx123Document16 pagesMicrobiology Assignmentt xxx123ADITYAROOP PATHAKNo ratings yet
- Pharmacology: Fast and Dirty Board ReviewDocument7 pagesPharmacology: Fast and Dirty Board ReviewRochelleth7278No ratings yet
- Title: meropenem: Student Name: طباس ميرك ليلخDocument6 pagesTitle: meropenem: Student Name: طباس ميرك ليلخKha KinNo ratings yet
- Antibiotik Imipenem Golongan CarbapenemDocument5 pagesAntibiotik Imipenem Golongan Carbapenemabam_abamNo ratings yet
- Antimicrobial DrugsDocument63 pagesAntimicrobial DrugsRonalyn UgatNo ratings yet
- 2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Document28 pages2-Cell Wall Inhibitor Antibitics-I Oct 15th 2018Leena AlateeqNo ratings yet
- Chemotherapeutic DrugsDocument122 pagesChemotherapeutic Drugsdex7reme100% (1)
- Aminoglycosides 23099Document27 pagesAminoglycosides 23099TES SENNo ratings yet
- 5 AminoglycosidesDocument7 pages5 AminoglycosidesNashat SaadiNo ratings yet
- Antibiotics 3: (Year 1 Term 2) (Session 2014-2015) by Professor Dr. Naeem Hasan Khan 17.04.2015Document35 pagesAntibiotics 3: (Year 1 Term 2) (Session 2014-2015) by Professor Dr. Naeem Hasan Khan 17.04.2015ArunaNo ratings yet
- Pharmacology AntibioticsDocument70 pagesPharmacology Antibioticsmaggie100% (1)
- FTX Infeksi JamurDocument64 pagesFTX Infeksi JamurNafisah SofiaNo ratings yet
- Monobactams & CarbapenemsDocument41 pagesMonobactams & CarbapenemsHussein AlhaddadNo ratings yet
- Antibiotic's Interactions in GynecologyDocument26 pagesAntibiotic's Interactions in Gynecologyمحمد قاسمNo ratings yet
- Pharmacology-Antibiotic 2021Document52 pagesPharmacology-Antibiotic 2021Ngọc VânNo ratings yet
- Drug Resistance Pharmacology Lecture Lecture Series 2019Document23 pagesDrug Resistance Pharmacology Lecture Lecture Series 2019temitopeNo ratings yet
- Microbiology AssignmentDocument18 pagesMicrobiology AssignmentADITYAROOP PATHAKNo ratings yet
- ChemotherapyDocument66 pagesChemotherapyElias HaimanotNo ratings yet
- Antimicrobials Complete by DR - Mayur Sayta M 91 PDFDocument86 pagesAntimicrobials Complete by DR - Mayur Sayta M 91 PDFRuthvi Jain100% (1)
- Chapter 9 Surgical Infections and Antibiotic SelectionDocument42 pagesChapter 9 Surgical Infections and Antibiotic SelectionSteven Mark MananguNo ratings yet
- 13 - Antibiotic III Nalidixic AcidDocument7 pages13 - Antibiotic III Nalidixic AcidMoataz TrabehNo ratings yet
- AntibioticsDocument63 pagesAntibioticsSahin mollickNo ratings yet
- Antimicrobial TherapyDocument18 pagesAntimicrobial TherapysaifNo ratings yet
- Pharmacology Powerpoint - AntibioticsDocument90 pagesPharmacology Powerpoint - AntibioticsAdminNo ratings yet
- Anti - TB DrugsupdatedDocument35 pagesAnti - TB DrugsupdatedgNo ratings yet
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
- Dental Anxiety Form 4 PDFDocument2 pagesDental Anxiety Form 4 PDFBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
- Gastro highlightCHAPTER1Document12 pagesGastro highlightCHAPTER1Lovely CruzxNo ratings yet
- 7JC - Early TreatmentDocument18 pages7JC - Early Treatmentanon_137544084No ratings yet
- Orbans Oral Histology Embryology 15Th Edition G S Kumar Full ChapterDocument67 pagesOrbans Oral Histology Embryology 15Th Edition G S Kumar Full Chaptersimon.sheneman371100% (5)
- 3rd YrMedical Surgical NursingDocument24 pages3rd YrMedical Surgical Nursingpunam todkarNo ratings yet
- Paracetamol Poisoning: G. Rajapandi 521625111 Final MbbsDocument18 pagesParacetamol Poisoning: G. Rajapandi 521625111 Final MbbsAntony PrakashNo ratings yet
- Diuretic Activity of S.officinarumDocument42 pagesDiuretic Activity of S.officinarumPalaksha M.N.No ratings yet
- A Short History of VaccinationDocument16 pagesA Short History of VaccinationAlejandro MotoliníaNo ratings yet
- SRS Kidney - 2016BDocument3 pagesSRS Kidney - 2016ByayayanizaNo ratings yet
- Hematological Emergencies in Dental Office by DR Khalid Hassan AlhazmiDocument13 pagesHematological Emergencies in Dental Office by DR Khalid Hassan Alhazmiamoon almNo ratings yet
- CHN ExamDocument30 pagesCHN ExamKhei Laqui SN100% (3)
- A Thing of Nothing. The Catastrophic Body in HamletDocument19 pagesA Thing of Nothing. The Catastrophic Body in HamletMarialena MarialenakiNo ratings yet
- Difficult Airway Management: 2009 Adrian SieberhagenDocument26 pagesDifficult Airway Management: 2009 Adrian Sieberhagendpeka dpekaNo ratings yet
- Piggery InvestmentDocument9 pagesPiggery InvestmentAndile Ntuli100% (1)
- Renal Fabs Post TestDocument3 pagesRenal Fabs Post Testlorelyn corpuzNo ratings yet
- CH 26 - The FungiDocument29 pagesCH 26 - The FungiBronwyn JuliusNo ratings yet
- Learning Continuity Plan For The Limited Face To Face ClassesDocument41 pagesLearning Continuity Plan For The Limited Face To Face ClassesHaimen BuisanNo ratings yet
- English: Learning Activity Sheets Module 1: What Composes MeDocument12 pagesEnglish: Learning Activity Sheets Module 1: What Composes MeGe PebresNo ratings yet
- chn-1 InfosheetDocument71 pageschn-1 InfosheetAMIR LADJANo ratings yet
- Clinical Report FinalDocument45 pagesClinical Report FinalBENJAMIN MAWUENYEGAHNo ratings yet
- 132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SDocument4 pages132 - Neurology Pathology - Stroke Syndromes - MCA, ACA, ICA, PCA, Vertebrobasilar Artery SUsman AR VainceNo ratings yet
- PDF Copy Haematology Laboratory Manual Cls 241 PDFDocument70 pagesPDF Copy Haematology Laboratory Manual Cls 241 PDFKahina Ould TalebNo ratings yet
- Unit Test 8B: Are Girls Better at Cooking?Document5 pagesUnit Test 8B: Are Girls Better at Cooking?Ana TodorovićNo ratings yet
- Anavar (Oxandrolone)Document26 pagesAnavar (Oxandrolone)illicitdrugsNo ratings yet
- MemoryDocument11 pagesMemorydkrms DNo ratings yet
- New York Health Welcomes Jay B. Adlersberg, M.D.Document2 pagesNew York Health Welcomes Jay B. Adlersberg, M.D.PR.comNo ratings yet