Download as pptx, pdf, or txt
You might also like
- Salso Manual 2018Document124 pagesSalso Manual 2018Sana Anam Jahan100% (1)
- Example of A Personal Leadership SWOTDocument1 pageExample of A Personal Leadership SWOTVishwanath Usha100% (1)
- Chapter 2 - OHSA Scavenger Hunt - Dropbox #1Document3 pagesChapter 2 - OHSA Scavenger Hunt - Dropbox #1Joshua AbrahamNo ratings yet
- AP Medical Council Renewal ApplicationDocument2 pagesAP Medical Council Renewal Applicationdrvaas73% (11)
- Diabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDocument18 pagesDiabetic Ketoacidosis Hypoglycemia: DR MD Mamunul Abedin ShimulDr. Mamunul AbedinNo ratings yet
- Case Write Up MedicineDocument16 pagesCase Write Up MedicineSana Anam JahanNo ratings yet
- Sinha's Comprehensive Anxiety Test (SCAT)Document9 pagesSinha's Comprehensive Anxiety Test (SCAT)Pragya100% (13)
- Holistic Health and The Critique of Western Medicine - Janet McKeeDocument3 pagesHolistic Health and The Critique of Western Medicine - Janet McKeeAlex CosiNo ratings yet
- Diabetic KetoacidosisDocument27 pagesDiabetic Ketoacidosisjun sianNo ratings yet
- Diabetic Ketoacidosis (DKA) - Presentation Slide EditedDocument22 pagesDiabetic Ketoacidosis (DKA) - Presentation Slide EditedTerence Chin0% (1)
- Diabetes KetoacidosisDocument23 pagesDiabetes KetoacidosisSalman MajidNo ratings yet
- DKA Canadian ProtocolDocument2 pagesDKA Canadian Protocolplay_wright2084No ratings yet
- Nursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Document9 pagesNursing Care Plan: Fluid Volume Deficit R/T Active Fluid Loss (Increased Urine Output)Gayu Patel0% (1)
- Diabetic Ketoacidosis:: Evidence Based ReviewDocument4 pagesDiabetic Ketoacidosis:: Evidence Based ReviewgracedumaNo ratings yet
- DkaDocument38 pagesDkaHam SotheaNo ratings yet
- Case Presentation: Andreas Crede EM RegistrarDocument15 pagesCase Presentation: Andreas Crede EM RegistrarHeru WahyudiNo ratings yet
- Diabetic Ketoacidosis (DKA) & Hyperglycemic Hyperosmolar State (HHS)Document36 pagesDiabetic Ketoacidosis (DKA) & Hyperglycemic Hyperosmolar State (HHS)Ismail GunawanNo ratings yet
- Dka & HHS: Ketoasidosis Diabetikum & Hiperosmolaritas Hyperglikemik StageDocument17 pagesDka & HHS: Ketoasidosis Diabetikum & Hiperosmolaritas Hyperglikemik StageAmeel BubbleeNo ratings yet
- 3a Emergency Care DKA (UK) FINALDocument40 pages3a Emergency Care DKA (UK) FINALDrsarfaraz SiddiquiNo ratings yet
- Diabetic Ketoacidosis in Pregnancy: Diagnosis of DKADocument7 pagesDiabetic Ketoacidosis in Pregnancy: Diagnosis of DKA123someone123No ratings yet
- Guidelines For Management of Diabetes MellitusDocument1 pageGuidelines For Management of Diabetes MellitusthapanNo ratings yet
- Diabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: DiagnosisDocument1 pageDiabetic Ketoacidosis (D.K.A) Beaumont Hospital Protocol: Diagnosislouglee9174100% (1)
- สำเนา draft1 - DKA 1Document42 pagesสำเนา draft1 - DKA 1teddypor100% (1)
- Diabetic KetoacidosisDocument13 pagesDiabetic KetoacidosisMabelle Blancada ConsultaNo ratings yet
- Dka Guidelines - 2012Document4 pagesDka Guidelines - 2012djizhieeNo ratings yet
- Endocrine Emergencies in The ICUDocument47 pagesEndocrine Emergencies in The ICUchadchimaNo ratings yet
- Diabetic KetoacidosisDocument5 pagesDiabetic Ketoacidosislpickering33No ratings yet
- Hyperglycemia Crisis: Dr. Netty NurnaningtyasDocument34 pagesHyperglycemia Crisis: Dr. Netty Nurnaningtyasnetty nurnaningtyas100% (1)
- DKA and HHSDocument16 pagesDKA and HHSGepengCungkringNo ratings yet
- Emergency Diabetes 2023 - Septian Mixrova SebayangDocument30 pagesEmergency Diabetes 2023 - Septian Mixrova SebayangFiqri DzulfaqqorNo ratings yet
- Hyponatremia: Michael TobinDocument24 pagesHyponatremia: Michael Tobinmtob3516No ratings yet
- Diabetic KetoacidosisDocument22 pagesDiabetic KetoacidosispoktaviantiNo ratings yet
- Adrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal MedicineDocument24 pagesAdrenal Insufficiency: DR - Abbas Mansour Senior Consultant Internal Medicineraed faisalNo ratings yet
- Hyponatremia in Children 03.19.2010Document23 pagesHyponatremia in Children 03.19.2010Emily EresumaNo ratings yet
- DKA Simlab FinalDocument3 pagesDKA Simlab FinalTee WoodNo ratings yet
- Acute Complications of Diabetes MellitusDocument43 pagesAcute Complications of Diabetes MellitusalphaphoenixNo ratings yet
- Approach To The Child With Metabolic Acidosis - UDocument3 pagesApproach To The Child With Metabolic Acidosis - URishi Shrestha100% (1)
- DKA NICE GuidlineDocument13 pagesDKA NICE GuidlineSachin DangiNo ratings yet
- Diabetic KetoasidosisDocument33 pagesDiabetic KetoasidosisGrace UlyNo ratings yet
- Pediatric DKA: Section I: Scenario DemographicsDocument7 pagesPediatric DKA: Section I: Scenario DemographicsSugi DenyNo ratings yet
- Assessment of Metabolic AcidosisDocument34 pagesAssessment of Metabolic Acidosisfatha100% (1)
- Disorders of The Parathyroid GlandsDocument30 pagesDisorders of The Parathyroid Glandsikram ullah khan100% (1)
- Acid-Base Homeostasis: Dr. Abeer KhurshidDocument42 pagesAcid-Base Homeostasis: Dr. Abeer Khurshidسلة فواكة100% (2)
- Cushing SyndromeDocument19 pagesCushing SyndromerituNo ratings yet
- Ketone Bodies 2012Document15 pagesKetone Bodies 2012Adhya MurugesanNo ratings yet
- Alzheimer's Disease: Causes, Effects, and TreatmentsDocument21 pagesAlzheimer's Disease: Causes, Effects, and TreatmentsJesshica Navarro AlejandrinoNo ratings yet
- Type 1 Diabetes: Diabetic Ketoacidos ISDocument16 pagesType 1 Diabetes: Diabetic Ketoacidos ISapi-551073862No ratings yet
- Pathophysiology of ShockDocument56 pagesPathophysiology of ShockDr. Haricharan ANo ratings yet
- Pediatric DKA: Section I: Scenario DemographicsDocument8 pagesPediatric DKA: Section I: Scenario DemographicsSherein ShalabyNo ratings yet
- Clinical Order Set DKA AdultDocument2 pagesClinical Order Set DKA AdultBashar Al-HamaidehNo ratings yet
- Management of DKA PresentationDocument46 pagesManagement of DKA PresentationMuhammed YesufNo ratings yet
- HyponatremiaDocument19 pagesHyponatremiaapi-260357356No ratings yet
- GTTDocument4 pagesGTTdr hinaNo ratings yet
- RhabdomyolysisDocument2 pagesRhabdomyolysisintrovoyz041No ratings yet
- Metabolism and NutritionDocument52 pagesMetabolism and NutritionAlex SaljayNo ratings yet
- Type2dm PDFDocument3 pagesType2dm PDFapi-303065684No ratings yet
- Diabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManDocument66 pagesDiabetes Mellitus: Ma. Tosca Cybil A. Torres, RN, ManElvis J. DavisNo ratings yet
- Case StudyDocument6 pagesCase Studyapi-276551783No ratings yet
- Adrenal Insufficiency and Cushing's Disease-1Document34 pagesAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesNo ratings yet
- Paediatric Diabetic KetoacidosisDocument7 pagesPaediatric Diabetic KetoacidosisJuan Carlos BayonaNo ratings yet
- Pituitary Gland DisordersDocument3 pagesPituitary Gland DisordersPAPIYA BHATTACHARYANo ratings yet
- DM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Document1 pageDM Diabetic Ketoacidosis DKA Management Algorithm Adult Patients 2019Hendra AfrilaNo ratings yet
- Acid Base BalanceDocument60 pagesAcid Base BalanceMariamNo ratings yet
- Postmortem Biochemistry of Vitreous Humor and Glucose MetabolismDocument7 pagesPostmortem Biochemistry of Vitreous Humor and Glucose MetabolismsbeyeforhireNo ratings yet
- The Complications of DiabetesDocument1 pageThe Complications of DiabetesMiguel Cuevas DolotNo ratings yet
- Electrolyte AbnormalitiesDocument74 pagesElectrolyte Abnormalitiesbluecrush1No ratings yet
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDocument23 pagesDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- CWU OrthopedicsDocument6 pagesCWU OrthopedicsSana Anam JahanNo ratings yet
- Case 2-Chest Pain: Alifah & LiyanaDocument18 pagesCase 2-Chest Pain: Alifah & LiyanaSana Anam JahanNo ratings yet
- Lesson Plan in Tle SubjectDocument11 pagesLesson Plan in Tle SubjectJonaiza PangandianNo ratings yet
- Secondary Victimization - Domestic Violence Survivors Navigating The Family Law SystemDocument22 pagesSecondary Victimization - Domestic Violence Survivors Navigating The Family Law SystemJihan Savira LamengNo ratings yet
- Juan Carlos I. Iquiña, PTRP: Personal InformationDocument2 pagesJuan Carlos I. Iquiña, PTRP: Personal InformationEunice IquinaNo ratings yet
- Ap06-Aa7-Ev06 Inglés Taller Reconociendo El Lugar de TrabajoDocument11 pagesAp06-Aa7-Ev06 Inglés Taller Reconociendo El Lugar de TrabajoAlejandro RománNo ratings yet
- Desain Penugasan KMB III Tranfer Ko EniDocument7 pagesDesain Penugasan KMB III Tranfer Ko EniAhmad NajibNo ratings yet
- Microbiology (HBM 531)Document5 pagesMicrobiology (HBM 531)panther795No ratings yet
- Spanish For Medical ProfessionalsDocument372 pagesSpanish For Medical ProfessionalsJean MallipudiNo ratings yet
- Adapted From The CDC/NIH 3rd Edition Of: Biosafety in Microbiological and Biomedical LaboratoriesDocument8 pagesAdapted From The CDC/NIH 3rd Edition Of: Biosafety in Microbiological and Biomedical Laboratoriesdipys41No ratings yet
- Reading Comprehension - The Ten Happiest Countries in The WorldDocument2 pagesReading Comprehension - The Ten Happiest Countries in The WorldDayse LopesNo ratings yet
- Envirotrends Regulatory Update#105 of 2020 - PESOs Circular Regarding Safety Precautions Under Petroleum Rules 2002Document2 pagesEnvirotrends Regulatory Update#105 of 2020 - PESOs Circular Regarding Safety Precautions Under Petroleum Rules 2002Rohit ShuklaNo ratings yet
- Comm Med AIIMS Nov 2019 v2Document17 pagesComm Med AIIMS Nov 2019 v2NokiaNo ratings yet
- A Study of Snail Behavior: Directions For StudentsDocument28 pagesA Study of Snail Behavior: Directions For StudentsHyacinth Jade SantosNo ratings yet
- Toothpaste IngredientsDocument10 pagesToothpaste Ingredientsjaxine labialNo ratings yet
- Surgical GuideDocument29 pagesSurgical GuideVăn Trọng MinhNo ratings yet
- A12 Prevmed Flashcards Oct 2022Document5 pagesA12 Prevmed Flashcards Oct 2022edgarciaNo ratings yet
- Jurnal Pentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup WargaDocument1 pageJurnal Pentingnya Memelihara Kebersihan Dan Keamanan Lingkungan Secarapartisipatif Demi Meningkatkan Gotong Royong Dan Kualitas Hidup Wargaeko sutarkoNo ratings yet
- Unit 5.1 Student JLBDocument26 pagesUnit 5.1 Student JLBkendrabooboooNo ratings yet
- Cerebrospinal Fluid and Blood Biomarkers For Neurodegenerative Dementias An Update of The Consensus of The Task Force On BioDocument87 pagesCerebrospinal Fluid and Blood Biomarkers For Neurodegenerative Dementias An Update of The Consensus of The Task Force On BioPer SabNo ratings yet
- Original Contribution: The SHEZ StudyDocument9 pagesOriginal Contribution: The SHEZ StudyRaúl AñariNo ratings yet
- Productlist 20221121Document3 pagesProductlist 20221121idboggNo ratings yet
- Memo-1 HRDocument2 pagesMemo-1 HRMukhammadbobur ShamirbaevNo ratings yet
- 18 Affidavit of Experience (Form A)Document2 pages18 Affidavit of Experience (Form A)playbowensNo ratings yet
- Book 2 Mock 1 2018 FebDocument16 pagesBook 2 Mock 1 2018 FebMonaNo ratings yet
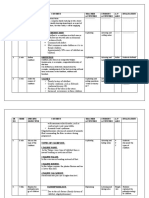
- SR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationDocument16 pagesSR NO Time Specific Objective Content Teacher Activities Student Activities A.V Aids EvaluationJuhi Johnson JadhavNo ratings yet
- Inserto Fibrinogeno SIEMENSDocument5 pagesInserto Fibrinogeno SIEMENSedson floresNo ratings yet