Download as pptx, pdf, or txt
You might also like
- Free Worksheets From CBT Toolbox For Children and AdolescentsDocument4 pagesFree Worksheets From CBT Toolbox For Children and AdolescentsFernanda Keren de Paula40% (20)
- Blood Gas Analysis Ppt-3Document32 pagesBlood Gas Analysis Ppt-3Kresna Dharma SuryanaNo ratings yet
- OBG-GYN Practice QuestionsDocument222 pagesOBG-GYN Practice QuestionsRizwanNo ratings yet
- Fundamentals of NursingDocument31 pagesFundamentals of NursingAngelica Soriano93% (14)
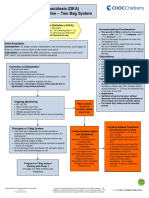
- Diabetic Ketoacidosis Care GuidelineDocument5 pagesDiabetic Ketoacidosis Care GuidelineRahma DhNo ratings yet
- AdenoidsDocument6 pagesAdenoidsIfeanyichukwu OgbonnayaNo ratings yet
- Exudative Pleural Effusions - UpToDateDocument2 pagesExudative Pleural Effusions - UpToDateAsif IqbalNo ratings yet
- ChickenpoxDocument3 pagesChickenpoxEdward McSweegan, PhDNo ratings yet
- Polycythemia Vera: What Are The Symptoms of Polycythemia?Document10 pagesPolycythemia Vera: What Are The Symptoms of Polycythemia?Dimpal ChoudharyNo ratings yet
- Asthma: Dr.M.Mehtab TehseenDocument14 pagesAsthma: Dr.M.Mehtab TehseenAsad AhmadNo ratings yet
- Management of Hypoxia During AnaesthesiaDocument5 pagesManagement of Hypoxia During AnaesthesiaNurhafizahImfista100% (1)
- Diabetic KetoacidosisDocument7 pagesDiabetic KetoacidosisetengNo ratings yet
- Lower Respiratory Tract InfectionDocument9 pagesLower Respiratory Tract InfectionNamrah AfzalNo ratings yet
- Questions For OSCE Exam - Model AnswersDocument9 pagesQuestions For OSCE Exam - Model AnswersFarah FarahNo ratings yet
- NIV Fs 9108147 e 1911 1 PDFDocument4 pagesNIV Fs 9108147 e 1911 1 PDFliuchenshitaoNo ratings yet
- DVT Case StudyDocument2 pagesDVT Case StudyCrystal B Costa78No ratings yet
- Case History of Focal PneumoniaDocument6 pagesCase History of Focal PneumoniaEmmanuel Akhadelor0% (2)
- Pulmonary EdemaDocument2 pagesPulmonary EdemaMuhammad Bayu Zohari HutagalungNo ratings yet
- Asthma2 Case StudyDocument8 pagesAsthma2 Case StudyGlenn Asuncion PagaduanNo ratings yet
- Running Head: A Patient Who Has Glaucoma 1Document10 pagesRunning Head: A Patient Who Has Glaucoma 1Alonso LugoNo ratings yet
- Tonsillectomy - ORDocument3 pagesTonsillectomy - ORRich John Mercene-NewNo ratings yet
- Pathophysiology of AsthmaDocument71 pagesPathophysiology of AsthmaChin ChanNo ratings yet
- K.6 PicoDocument9 pagesK.6 PicoSteven FongNo ratings yet
- Bullous PemphigoidDocument21 pagesBullous PemphigoidChe Ainil ZainodinNo ratings yet
- Intensive V (Complications)Document117 pagesIntensive V (Complications)darren55No ratings yet
- Cheiloplasty and PalatoplastyDocument41 pagesCheiloplasty and Palatoplastyapi-325029251No ratings yet
- Visual Acuity Test: Presented by Sushma Shrestha Roll No 38Document20 pagesVisual Acuity Test: Presented by Sushma Shrestha Roll No 38sushma shresthaNo ratings yet
- Chronic Suppurative Otitis MediaDocument11 pagesChronic Suppurative Otitis MediaaditiarrtuguNo ratings yet
- Dr. Kristia Hermawan, MSC, Sp.A: Pediatric Nephrology Sub-DivisionDocument47 pagesDr. Kristia Hermawan, MSC, Sp.A: Pediatric Nephrology Sub-DivisionWindy MentariNo ratings yet
- GP Reg - Asthma and Spirometry 2011Document114 pagesGP Reg - Asthma and Spirometry 2011minerva_stanciuNo ratings yet
- Acute Cholecystitis SeminarDocument42 pagesAcute Cholecystitis SeminarNatnaelNo ratings yet
- Medical Surgical Nursing Suretech College of NursingDocument18 pagesMedical Surgical Nursing Suretech College of NursingSanket TelangNo ratings yet
- Pulmonary EmbolismDocument47 pagesPulmonary EmbolismmalathiNo ratings yet
- HyperopiaDocument6 pagesHyperopiageeneevzzNo ratings yet
- DR As TuberculosisDocument59 pagesDR As TuberculosisAchhar SinghNo ratings yet
- Lower Respiratory Tract InfectionDocument6 pagesLower Respiratory Tract InfectionFlorence De ChavezNo ratings yet
- (Pelvic Inflammatory Disease) Samiya AhmedDocument31 pages(Pelvic Inflammatory Disease) Samiya AhmedSaamiya AhmedNo ratings yet
- Chronic Otitis MediaDocument24 pagesChronic Otitis Mediaingidzai100% (1)
- CholecystectomyDocument6 pagesCholecystectomyTom Bayubs-tucsNo ratings yet
- CHPT 70 Respiratory Part 2Document56 pagesCHPT 70 Respiratory Part 2helen brockNo ratings yet
- Case Study CLD 3Document18 pagesCase Study CLD 3MoonNo ratings yet
- NIH Aids Info HIV Treatment Guidelines AdultandadolescentglDocument267 pagesNIH Aids Info HIV Treatment Guidelines Adultandadolescentglbmartindoyle6396No ratings yet
- Airway Emergencies: ORL PostingDocument58 pagesAirway Emergencies: ORL PostingKimberlyLaw95No ratings yet
- Biliary Tract DiseasesDocument35 pagesBiliary Tract DiseasesSoumya Ranjan PandaNo ratings yet
- Premature BabyDocument5 pagesPremature Babypaulinagigantone100% (1)
- DIC Case StudyDocument7 pagesDIC Case StudyRobertNo ratings yet
- Acute Rheumatic Fever: Prof - Univ.Dr. Corina ZorilăDocument40 pagesAcute Rheumatic Fever: Prof - Univ.Dr. Corina ZorilăGermanyNo ratings yet
- Menigitis EncephalitisDocument63 pagesMenigitis EncephalitisHussain Azhar100% (1)
- Pa Tho PhysiologyDocument4 pagesPa Tho Physiologyimagine28No ratings yet
- PancreatitisDocument59 pagesPancreatitisAarif RanaNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument2 pagesIdiopathic Thrombocytopenic PurpuraMitch Hellgirl AlmonteNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument8 pagesIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaNo ratings yet
- Brain AbscessDocument25 pagesBrain AbscessprembarnabasNo ratings yet
- AKI CASE NishaDocument64 pagesAKI CASE NishaSurkhali Bipana100% (1)
- MeaslesDocument23 pagesMeaslesadwait marhattaNo ratings yet
- Cirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDocument21 pagesCirrhosis in Adults: Overview of Complications, General Management, and Prognosis - UpToDateDan ChicinasNo ratings yet
- Hiatal Hernia: BY MR, Vinay KumarDocument27 pagesHiatal Hernia: BY MR, Vinay KumarVinay KumarNo ratings yet
- Urinary Retention PostpartumDocument5 pagesUrinary Retention PostpartumpaswordnyalupaNo ratings yet
- Ebstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEbstein Anomaly, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- HemorrhoidsDocument25 pagesHemorrhoidsAdoma SportsNo ratings yet
- HEMOROIDDocument29 pagesHEMOROIDDanang Aryo PinujiNo ratings yet
- Jurnal 3 Diagnosis and Management of Internal Hemorrhoids - A Brief ReviewDocument16 pagesJurnal 3 Diagnosis and Management of Internal Hemorrhoids - A Brief ReviewRosfi Firdha HuzaimaNo ratings yet
- Hemorrhoid Externa: Qara Syifa Fachrani 1610211039Document25 pagesHemorrhoid Externa: Qara Syifa Fachrani 1610211039Qara Syifa FNo ratings yet
- Psychology A Student Friendly ApproachDocument344 pagesPsychology A Student Friendly ApproachcacharretaNo ratings yet
- Placental Abruption - Management - UpToDateDocument14 pagesPlacental Abruption - Management - UpToDateCarlos Jeiner Díaz SilvaNo ratings yet
- Irrigation of RCTDocument30 pagesIrrigation of RCTRafiur RahmanNo ratings yet
- Osteopathie FoundationDocument4 pagesOsteopathie FoundationAnonymous VghTGARciNo ratings yet
- Card 1Document2 pagesCard 1nalessNo ratings yet
- Molecular Basis of The Anti-Aging' Effect of Spermidine and Other Natural Polyamines - A Mini-ReviewDocument8 pagesMolecular Basis of The Anti-Aging' Effect of Spermidine and Other Natural Polyamines - A Mini-ReviewAntares1973No ratings yet
- Assessment of The Level of Adherance of Private Medical Clinics in Kampala To The Standards of Good Pharmacy PracticeDocument70 pagesAssessment of The Level of Adherance of Private Medical Clinics in Kampala To The Standards of Good Pharmacy PracticeCaroleKKagandaNo ratings yet
- Enbrel Side EffectsDocument5 pagesEnbrel Side EffectsDionisis MentzeniotisNo ratings yet
- Dandy Walker SyndromeDocument9 pagesDandy Walker SyndromeDarshika Vyas MohanNo ratings yet
- Movie Review - The NOTEBOOKDocument8 pagesMovie Review - The NOTEBOOKekhai47100% (3)
- Sarcoidosis Review. JAMADocument9 pagesSarcoidosis Review. JAMARafael ReañoNo ratings yet
- Nurs 5002 - Case Study 4Document17 pagesNurs 5002 - Case Study 4api-308904543100% (2)
- CT Scan Request 2ND PageDocument1 pageCT Scan Request 2ND PageAina Haravata100% (1)
- RECELL Repigmentation Underwhelms: Avita Medical (AVH)Document2 pagesRECELL Repigmentation Underwhelms: Avita Medical (AVH)Muhammad ImranNo ratings yet
- The Therapeutic Relationship - Leslie MelisaDocument47 pagesThe Therapeutic Relationship - Leslie MelisaLeslie Melisa100% (1)
- Asphalt PG 58-28: Material Safety Data SheetDocument3 pagesAsphalt PG 58-28: Material Safety Data SheetSen HuNo ratings yet
- PNS - Bafs 267.2022 - PNS Swine - Good Animal Husbandry Practices (GAHP)Document25 pagesPNS - Bafs 267.2022 - PNS Swine - Good Animal Husbandry Practices (GAHP)Johana Pinagayao AngkadNo ratings yet
- 5th SeminarDocument104 pages5th SeminarVeena GoudNo ratings yet
- Analgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiDocument31 pagesAnalgezia Si Anestezia in Obstetrica. Analgezia IN Travaliu: IndicatiiAlex GrigoreNo ratings yet
- BooksDocument12 pagesBookschakriy9No ratings yet
- Dr. Marwah'S Test Series Whatsapp Number: 9873835363, 8447982490,9717143789Document15 pagesDr. Marwah'S Test Series Whatsapp Number: 9873835363, 8447982490,97171437891S@M1No ratings yet
- Gonadil F Caps Leaflet Pakistan 1Document2 pagesGonadil F Caps Leaflet Pakistan 1carefulgurl42No ratings yet
- Jurnal Reading OtomikosisDocument4 pagesJurnal Reading OtomikosisTria JuwitaNo ratings yet
- TCM PorkDocument4 pagesTCM PorkVivekanandanvrNo ratings yet
- 10 Day ChallengeDocument5 pages10 Day Challengegidum2006No ratings yet
- Cytochrome P450 / PolymorphismDocument15 pagesCytochrome P450 / PolymorphismFULL NAMENo ratings yet
- Movie Review Shutter Island'Document16 pagesMovie Review Shutter Island'DishaSareenNo ratings yet