Download as ppt, pdf, or txt
You might also like
- Blood Case Studies - Study CasesDocument6 pagesBlood Case Studies - Study CasesManuela Maria Venegas Escovar0% (1)
- 1.atlas Hematologi Diggs PDFDocument128 pages1.atlas Hematologi Diggs PDFPuspa YaNi100% (6)
- 10.21307 - Immunohematology 2022 048 PDFDocument6 pages10.21307 - Immunohematology 2022 048 PDFTanupreetNo ratings yet
- 2.membrane Physiology, Nerve and MuscleDocument6 pages2.membrane Physiology, Nerve and MuscleCLEMENT100% (1)
- Sideroblastic AnemiaDocument8 pagesSideroblastic AnemiaIslam Ahmady MohamedNo ratings yet
- Haematopoiesis: DR Rosline Hassan Hematology Department School of Medical Sciences Universiti Sains MalaysiaDocument46 pagesHaematopoiesis: DR Rosline Hassan Hematology Department School of Medical Sciences Universiti Sains Malaysialow_sernNo ratings yet
- 7 RespirationDocument15 pages7 RespirationCLEMENTNo ratings yet
- Patho Physiology Lecture13Document10 pagesPatho Physiology Lecture13Manar AlzobiNo ratings yet
- Blood 12-6-2018Document42 pagesBlood 12-6-2018Noor Fatima100% (1)
- White Blood CellsDocument35 pagesWhite Blood CellsYsa ZapantaNo ratings yet
- Haemoglobin: Higher The Partial Pressure, The Higher The AffinityDocument2 pagesHaemoglobin: Higher The Partial Pressure, The Higher The Affinitydebbie96No ratings yet
- Haem. Notes (MBCHB) ProperDocument162 pagesHaem. Notes (MBCHB) ProperKelvinTMaikanaNo ratings yet
- Anemia Its Laboratory DiagnosisDocument146 pagesAnemia Its Laboratory DiagnosisCh M MushahidNo ratings yet
- LeukemiaDocument1 pageLeukemiaGomathiRachakondaNo ratings yet
- 2 Medicine HematologyDocument78 pages2 Medicine HematologyAmitNo ratings yet
- Oncology Revision: Paul BaillieDocument299 pagesOncology Revision: Paul BaillieMourian AmanNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- HEMATOPOESISDocument71 pagesHEMATOPOESISHussenNo ratings yet
- 01 BMDocument132 pages01 BMBianca OcampoNo ratings yet
- Anemia BMLTDocument134 pagesAnemia BMLTRajkishor YadavNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- Hemoglobin Structure & SynthesisDocument24 pagesHemoglobin Structure & SynthesisIMDCBiochemNo ratings yet
- Bleeding Disorders: LCDR Art GeorgeDocument54 pagesBleeding Disorders: LCDR Art Georgesatya_mdsNo ratings yet
- Hemat.Q - 1Document27 pagesHemat.Q - 1aliaaNo ratings yet
- Animal Physiology LabDocument13 pagesAnimal Physiology LabAbi Nirmalan0% (1)
- RBC IndicesDocument13 pagesRBC IndicespremNo ratings yet
- RBCDocument3 pagesRBCMalkish RajkumarNo ratings yet
- Antibody Structure and Function PDFDocument8 pagesAntibody Structure and Function PDFJay JaswaniNo ratings yet
- Disorders of Iron MetabolismDocument42 pagesDisorders of Iron MetabolismFatima Zuhra100% (1)
- RBC MembraneDocument41 pagesRBC MembranemwambungupNo ratings yet
- Bio Inorganic ChemistryDocument49 pagesBio Inorganic ChemistryMONIRUZZAMAN MONIR100% (1)
- Case 1: 25 Yr Old Patient With History of FatigueDocument79 pagesCase 1: 25 Yr Old Patient With History of FatigueMira Wrycza100% (1)
- Lecture 1 - Introduction To HematologyDocument30 pagesLecture 1 - Introduction To Hematologyimam100% (1)
- Blood Cells MorphologyDocument20 pagesBlood Cells Morphologymoonfire2009No ratings yet
- Red Cell and White Cell Counting, BloodDocument89 pagesRed Cell and White Cell Counting, BloodJovel Gangcuangco100% (1)
- Classification of Anemia OkDocument60 pagesClassification of Anemia OkAnonymous 7CnBF0cjNo ratings yet
- Glomerular Filtration: Membrane, Which Consists of A Meshwork ofDocument3 pagesGlomerular Filtration: Membrane, Which Consists of A Meshwork ofPriscilia FooNo ratings yet
- Anemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9Document30 pagesAnemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9hercolaniumNo ratings yet
- Function of RBCDocument9 pagesFunction of RBCAthea MelosantosNo ratings yet
- ErythropoiesisDocument44 pagesErythropoiesisDr ratna kumariNo ratings yet
- Microcytic Hypochromic Anemia: - M QariDocument33 pagesMicrocytic Hypochromic Anemia: - M QarirohitNo ratings yet
- Body FluidsDocument44 pagesBody FluidsO'Brien Alfred100% (1)
- Red Blood Cell CountDocument4 pagesRed Blood Cell CountMohamed MokhtarNo ratings yet
- BloodDocument6 pagesBloodFadhil Hussam AhmedNo ratings yet
- Blood ComponentsDocument44 pagesBlood ComponentsKrisha VittoNo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- ERYTHROPOIESISDocument17 pagesERYTHROPOIESISsureshNo ratings yet
- RBCs Abnormal MorphologyDocument33 pagesRBCs Abnormal Morphologysigit100% (1)
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
- Lipoprotein Disorders 2Document33 pagesLipoprotein Disorders 2Bolabo BenivoNo ratings yet
- Renal PathologyDocument28 pagesRenal PathologyApril Deveras JudillaNo ratings yet
- Iron Metabolism: DR Mukhtiar BaigDocument58 pagesIron Metabolism: DR Mukhtiar BaigdrmukhtiarbaigNo ratings yet
- Blood - 6 (Anemia)Document9 pagesBlood - 6 (Anemia)drusmansaleemNo ratings yet
- Haematology - Blood Films.Document6 pagesHaematology - Blood Films.kkkssbb100% (1)
- Normal Haemopoiesis: Dr. Tariq M. Roshan Department of Hematology PPSPDocument29 pagesNormal Haemopoiesis: Dr. Tariq M. Roshan Department of Hematology PPSPyamanassafNo ratings yet
- Von Willibrand DiseasesDocument34 pagesVon Willibrand DiseasesZulfadli Hussein100% (1)
- Sickle Cell TestDocument14 pagesSickle Cell TestkayNo ratings yet
- Cytochemical Stains in Haematology PDFDocument3 pagesCytochemical Stains in Haematology PDFABHINABA GUPTANo ratings yet
- Hemoglobin & Derivatives: DR. S. Irfan RazaDocument30 pagesHemoglobin & Derivatives: DR. S. Irfan RazaSyed Irfan Raza100% (1)
- Blood Cells, Immunity and Blood ClottingDocument65 pagesBlood Cells, Immunity and Blood Clottingmunaamuummee100% (1)
- Chapter 9&10: Microscopic Examination of Urinary Sediment: CastsDocument48 pagesChapter 9&10: Microscopic Examination of Urinary Sediment: CastsAllexandra CameliaNo ratings yet
- Anemia 101-Case StudiesDocument20 pagesAnemia 101-Case StudiesZamharira MuslimNo ratings yet
- History Taking and Physical Examination, Level 5Document48 pagesHistory Taking and Physical Examination, Level 5CLEMENT100% (1)
- Development of A Research ProposalDocument25 pagesDevelopment of A Research ProposalCLEMENTNo ratings yet
- Sports PhysiologyDocument3 pagesSports PhysiologyCLEMENTNo ratings yet
- 8.aviation, Space and Deep Sea Diving PhysiologyDocument5 pages8.aviation, Space and Deep Sea Diving PhysiologyCLEMENTNo ratings yet
- The HeartDocument15 pagesThe HeartCLEMENTNo ratings yet
- Synthesis of Eicosanoids and SignalingDocument10 pagesSynthesis of Eicosanoids and SignalingCLEMENTNo ratings yet
- Genetics: Definition: Branch of Biologic Science That Deals With Transmission of Characters From Parents To OffspringsDocument22 pagesGenetics: Definition: Branch of Biologic Science That Deals With Transmission of Characters From Parents To OffspringsCLEMENTNo ratings yet
- 1.introduction To Physiology, The Cell and General PhysiologDocument3 pages1.introduction To Physiology, The Cell and General PhysiologCLEMENT100% (1)
- Pathological Response To Infectious and Parasitic DiseasesDocument36 pagesPathological Response To Infectious and Parasitic DiseasesCLEMENTNo ratings yet
- Pathogenesis and Classification of NeoplasiaDocument36 pagesPathogenesis and Classification of NeoplasiaCLEMENT0% (1)
- Growth and Development in Children by Dr. Rafia. IqbalDocument34 pagesGrowth and Development in Children by Dr. Rafia. IqbalCLEMENTNo ratings yet
- DicDocument17 pagesDicCLEMENT0% (1)
- Nutritional and Nutritional RequirementsDocument25 pagesNutritional and Nutritional RequirementsCLEMENTNo ratings yet
- Cellular Growth, Injury and Adaptation: DR Kasonda Pediatrician 17/5/2017Document3 pagesCellular Growth, Injury and Adaptation: DR Kasonda Pediatrician 17/5/2017CLEMENTNo ratings yet
- Malaria: Definition: Infection Due To PlasmodiumDocument17 pagesMalaria: Definition: Infection Due To PlasmodiumCLEMENTNo ratings yet
- Clinical Use of Antimicrobial AgentsDocument24 pagesClinical Use of Antimicrobial AgentsCLEMENTNo ratings yet
- Clinical Epidemiology of The Leading Causes of MorbidityDocument22 pagesClinical Epidemiology of The Leading Causes of MorbidityCLEMENTNo ratings yet
- Disorders of Skeletal, Cardiac and Smooth Muscle Cells-Myasthenia Gravis, Muscular Dystrophy and MyotoniaDocument51 pagesDisorders of Skeletal, Cardiac and Smooth Muscle Cells-Myasthenia Gravis, Muscular Dystrophy and MyotoniaCLEMENTNo ratings yet
- Protein Energy Malnutrition (PEM)Document39 pagesProtein Energy Malnutrition (PEM)CLEMENT100% (3)
- Basic PathologyDocument37 pagesBasic PathologyCLEMENTNo ratings yet
- Genital UlcersDocument17 pagesGenital UlcersCLEMENTNo ratings yet
- Antigens, Hapteins, Immunogens Lectures 10.1.06Document32 pagesAntigens, Hapteins, Immunogens Lectures 10.1.06CLEMENTNo ratings yet
- Gas Transport in Blood PPT 1Document34 pagesGas Transport in Blood PPT 1CLEMENTNo ratings yet
- Pain Sensation and Pathophysiology of Headache: Presenter: DR William Ramadhan.A FACILITATOR: DR M A. NjelekelaDocument34 pagesPain Sensation and Pathophysiology of Headache: Presenter: DR William Ramadhan.A FACILITATOR: DR M A. NjelekelaCLEMENTNo ratings yet
- Hypertension: Definition: BP 95% Percentile Incidence: 1% of All AdolescentsDocument15 pagesHypertension: Definition: BP 95% Percentile Incidence: 1% of All AdolescentsCLEMENTNo ratings yet
- Laboratory Flow Sheet: Hematology Blood ChemistryDocument2 pagesLaboratory Flow Sheet: Hematology Blood ChemistrytrialqwNo ratings yet
- Kontraksi Dan Eksitasi Otot Polos Sistem Muskuloskletal FREEDocument35 pagesKontraksi Dan Eksitasi Otot Polos Sistem Muskuloskletal FREENovita DamaiyantiNo ratings yet
- Mass Blood Donation (MBD) GuidelinesDocument4 pagesMass Blood Donation (MBD) GuidelinesRenz Dominic GonzalesNo ratings yet
- Plant TissuesDocument3 pagesPlant TissuesHolofa Andrea LemanaNo ratings yet
- Hematopoietic System PDFDocument275 pagesHematopoietic System PDFXochitl ZambranoNo ratings yet
- Blood Groups Practical NewDocument19 pagesBlood Groups Practical NewSreedeep TejaNo ratings yet
- Case Study On Wound HealingDocument5 pagesCase Study On Wound HealingINSANE LEO GAMINGNo ratings yet
- Plant Tissues - Practice QuestionsDocument4 pagesPlant Tissues - Practice QuestionsAruna PatilNo ratings yet
- Ananya Mishra Biology PaperDocument5 pagesAnanya Mishra Biology PaperA-Z Channel miahrajiNo ratings yet
- HistologyDocument109 pagesHistologyMEHMET ALİ KIRBIYIKNo ratings yet
- Animal Tissues: Lab ReviewDocument5 pagesAnimal Tissues: Lab ReviewTAHA GABRNo ratings yet
- Daftar Harga Pt. Raja Tiara Alkesindo - 2022Document3 pagesDaftar Harga Pt. Raja Tiara Alkesindo - 2022PT RAJA TIARA ALKESINDONo ratings yet
- Anemia in PregnancyDocument65 pagesAnemia in Pregnancyholly girlchy JastinNo ratings yet
- Revised Hema Outline Aug 2, 2020Document9 pagesRevised Hema Outline Aug 2, 2020Edna Uneta RoblesNo ratings yet
- Approach To Antibody IdentificationDocument4 pagesApproach To Antibody IdentificationMohamed ElmasryNo ratings yet
- 6 - HemoglobinopathiesDocument55 pages6 - HemoglobinopathiesSara BakerNo ratings yet
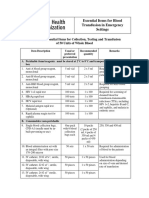
- Checklist of Essential Items For Collection, Testing and Transfusion of 50 Units of Whole BloodDocument4 pagesChecklist of Essential Items For Collection, Testing and Transfusion of 50 Units of Whole BloodGilbertmichyNo ratings yet
- Patomorfologia Prezentacja - KopiaDocument14 pagesPatomorfologia Prezentacja - KopiaOlgaNo ratings yet
- Lec - Activity11 and 13 - Blood - Blood - Vessel1Document3 pagesLec - Activity11 and 13 - Blood - Blood - Vessel1apple BananaNo ratings yet
- Transfusion-Related Acute Lung Injury (TRALI) - UpToDateDocument34 pagesTransfusion-Related Acute Lung Injury (TRALI) - UpToDateHartanto LieNo ratings yet
- HEMOPHILA ProjectDocument4 pagesHEMOPHILA ProjectShin SimNo ratings yet
- Types of Neurons PDFDocument2 pagesTypes of Neurons PDFPerry Sin100% (2)
- HM 09 20155v2 Ruby Casebook 122010 PDFDocument91 pagesHM 09 20155v2 Ruby Casebook 122010 PDFFrankie LamNo ratings yet
- Blood Donation 1Document10 pagesBlood Donation 1chhayaraviNo ratings yet
- BT ReactionDocument8 pagesBT ReactionMary Elijah Jane PopesNo ratings yet
- 1 Coagulation Disorderin PregnancyDocument21 pages1 Coagulation Disorderin PregnancyIntan Nursiani AgnurNo ratings yet
- DIC Case StudyDocument3 pagesDIC Case StudyJuliaNo ratings yet
- BCM 20 Ultra NewDocument11 pagesBCM 20 Ultra NewWessamNo ratings yet