Download as ppt, pdf, or txt
You might also like
- TestBank Norris Porths Essentials Pathophysiology 5e 2019Document505 pagesTestBank Norris Porths Essentials Pathophysiology 5e 2019Cindy Perez50% (2)
- HLT Health Training Package Implementation Guide Release 7.0 - December 2021 FinalDocument103 pagesHLT Health Training Package Implementation Guide Release 7.0 - December 2021 FinalElaine CruzNo ratings yet
- Post Partum Hemorhage Dan Management in Clinical Emergency - Sragen 2014-1Document59 pagesPost Partum Hemorhage Dan Management in Clinical Emergency - Sragen 2014-1Ndan Rahma100% (2)
- Ostpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)Document70 pagesOstpartum Hemorrhage: Dr. Patiyus Agustiansyah, Spog (K)JoNo ratings yet
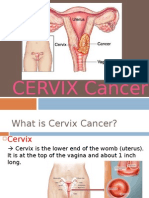
- Cervical CancerDocument30 pagesCervical Cancerhuhknee100% (1)
- Lung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHDocument61 pagesLung Collapse: A Review: Dr. Girish Kukade Radiology Department, AFHkukadegirishNo ratings yet
- Health and MedicineDocument2 pagesHealth and MedicinePARAELBLOG1No ratings yet
- Obsgin - Dr. Dr. Freddy W. Wagey, SpOG-KDocument26 pagesObsgin - Dr. Dr. Freddy W. Wagey, SpOG-KDedy SupriadiNo ratings yet
- Hellp Syndrome: DR Tonny Ertiatno SP Og (K)Document42 pagesHellp Syndrome: DR Tonny Ertiatno SP Og (K)Fazella KiraraNo ratings yet
- Hypertensive Disorder in Pregnancy Untuk KuliahDocument78 pagesHypertensive Disorder in Pregnancy Untuk Kuliah404notfoundNo ratings yet
- Hemorragic CystDocument14 pagesHemorragic CystNyoman TapayanaNo ratings yet
- Presentasi Perdarahan Post PartumDocument37 pagesPresentasi Perdarahan Post PartumFegana SutrisnoNo ratings yet
- MOET AlgorithmDocument1 pageMOET AlgorithmAli AlisonNo ratings yet
- Anemia & HemobionDocument56 pagesAnemia & HemobionMar'atus SholikahNo ratings yet
- Kardiotokografi Ppds (DR - JKS)Document68 pagesKardiotokografi Ppds (DR - JKS)Aditya PrabawaNo ratings yet
- Gangguan Siklus MenstruasiDocument26 pagesGangguan Siklus MenstruasiMardoni EfrijonNo ratings yet
- Vital Signs: Dono Indarto, DR., Mbiotechst - AifmDocument19 pagesVital Signs: Dono Indarto, DR., Mbiotechst - AifmdrgayuhNo ratings yet
- PartografDocument31 pagesPartografrovi wilmanNo ratings yet
- Sirkulasi UteroplasentaDocument16 pagesSirkulasi UteroplasentaPriscilla BudhipramonoNo ratings yet
- Dr. Kruvilla - Hyperthyroidism in PregnancyDocument38 pagesDr. Kruvilla - Hyperthyroidism in PregnancyjarvantaraNo ratings yet
- Perdarahan Post PartumDocument52 pagesPerdarahan Post PartumSeptyan Putra YusandyNo ratings yet
- 2012 Utrogestan Natural Micronized Progesterone - From Luteal Phase Defect To Preterm BirthDocument48 pages2012 Utrogestan Natural Micronized Progesterone - From Luteal Phase Defect To Preterm BirthRachel Paredes100% (1)
- Overview Antenatal CareDocument54 pagesOverview Antenatal CareRizky Dwidya AmirtasariNo ratings yet
- Gestational Trophoblastic DiseasesDocument37 pagesGestational Trophoblastic DiseasesEdwin OkonNo ratings yet
- Hymen ImperforataDocument7 pagesHymen ImperforataAdeTriansyahEmsilNo ratings yet
- LP Rupture UteriDocument17 pagesLP Rupture UteriMemancing KerusuhanNo ratings yet
- Case PreeklamsiDocument98 pagesCase Preeklamsinovika100% (1)
- Interna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityDocument46 pagesInterna Medicine Case Report Prof. Dr. W. Z. Johannes Hospital AUGUST 2019 Medical Faculty Nusa Cendana UniversityErni JawaNo ratings yet
- REFERAT - Ppt.solusio Plasenta ItaDocument18 pagesREFERAT - Ppt.solusio Plasenta ItaMochammad Adam EldiNo ratings yet
- Abnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008Document17 pagesAbnormal Uterine Bleeding: District 1 ACOG Medical Student Education Module 2008ninachayank0% (1)
- DK Endokrin Mola OgieDocument51 pagesDK Endokrin Mola OgiehariogieNo ratings yet
- Anemia Prenatal Care - DR - Rima IrwindaDocument43 pagesAnemia Prenatal Care - DR - Rima IrwindaHari SandiNo ratings yet
- Lapsus Ab Inkom Ahmad BaihaqiDocument30 pagesLapsus Ab Inkom Ahmad BaihaqiAhmad BaihaqiNo ratings yet
- Kanker Serviks Ed BimoDocument69 pagesKanker Serviks Ed BimoRr.Fara LuthfitaNo ratings yet
- Deteksi Dini Kanker RahimDocument10 pagesDeteksi Dini Kanker Rahimdr.gendisNo ratings yet
- Balans Cairan & Elektrolit RSTDocument59 pagesBalans Cairan & Elektrolit RSTMuhamad Agung SupriyantoNo ratings yet
- Perdarahan Pasca SalinDocument36 pagesPerdarahan Pasca SalinbennyrolandnababanNo ratings yet
- I. Skenario B Blok 17Document37 pagesI. Skenario B Blok 17Kadek MarthaNo ratings yet
- Dr. Ilham - AFLP - ISSHP 2017 BandungDocument40 pagesDr. Ilham - AFLP - ISSHP 2017 BandungMegaSariDewiNo ratings yet
- Algoritma EklampsiaDocument1 pageAlgoritma EklampsiaTheresia ChesarNo ratings yet
- Sarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalDocument2 pagesSarawak Thromboprophylaxis Risk Assessment Form: NAME: HOSPITAL: Risk Factors: Tick Score AntenatalTan Chin AunNo ratings yet
- Biophysical Profile, Ultrasound: IMS Murah-ManoeDocument39 pagesBiophysical Profile, Ultrasound: IMS Murah-ManoeBernardus Mario VitoNo ratings yet
- Stress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentDocument16 pagesStress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentJufri NstNo ratings yet
- (PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFDocument157 pages(PESERTA) PEDIATRI 2 - MANTAP Februari 2017 PDFmarcelinaNo ratings yet
- 10 Preeklampsia PDFDocument50 pages10 Preeklampsia PDFFithriani Sri UtamiNo ratings yet
- Preeklamsia Amp - dm18Document32 pagesPreeklamsia Amp - dm18Noni Minty BelantricNo ratings yet
- Mola HidatidosaDocument53 pagesMola HidatidosaJeanyanty Yoesteyn DjaranjoeraNo ratings yet
- Ekstraksi Forceps Vacuum Mahasiswa Fkui TK ViDocument19 pagesEkstraksi Forceps Vacuum Mahasiswa Fkui TK ViCiiezz BunciiezzNo ratings yet
- Sectio CaesareaDocument13 pagesSectio CaesareaDavid ZamrilNo ratings yet
- Anaemia in PregnancyDocument28 pagesAnaemia in PregnancyUsman G. HingoroNo ratings yet
- Tatalaksana Malaria Terkini Pada AnakDocument61 pagesTatalaksana Malaria Terkini Pada Anakretno adijayaNo ratings yet
- Dr. Herbert Situmorang, SpOG - (K) FER - Hyperemesis GravidarumDocument16 pagesDr. Herbert Situmorang, SpOG - (K) FER - Hyperemesis GravidarumDonutz RiNo ratings yet
- Acute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalDocument73 pagesAcute Abdominal Pain in Pregnancy: Diagnosis and Management Conservative vs. SurgicalIgnatov OanaNo ratings yet
- Pre Eclampsia: DR Kauser Mansoor Mrcog, Frcog Consultant & HODDocument46 pagesPre Eclampsia: DR Kauser Mansoor Mrcog, Frcog Consultant & HODRokr125No ratings yet
- Jadwal Pit (Fetomaternal Room)Document3 pagesJadwal Pit (Fetomaternal Room)Dwi Adi NugrohoNo ratings yet
- Solusio Plasenta: M.Thamrin TanjungDocument20 pagesSolusio Plasenta: M.Thamrin Tanjungashry909No ratings yet
- Perdarahan Pasca Persalinan: Sources: William, Obstetrics Illustrated, Buku Merah, Panduan Pelayanan IbuDocument25 pagesPerdarahan Pasca Persalinan: Sources: William, Obstetrics Illustrated, Buku Merah, Panduan Pelayanan IbuFirdinia Gafuri DohamidNo ratings yet
- Amenore PrimerDocument40 pagesAmenore PrimerMaksum Pandelima0% (1)
- Amnioinfusion - LEODocument16 pagesAmnioinfusion - LEOtapayanaNo ratings yet
- CA CervixDocument14 pagesCA CervixIphie Ivanna Octaviani100% (1)
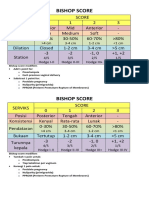
- Bishop ScoreDocument2 pagesBishop ScoreRskia Sadewwa Yogyakarta100% (1)
- Beta BlockersDocument70 pagesBeta BlockersIrina Cabac-PogoreviciNo ratings yet
- Efficacy of Beta - Blockers For First - Line Antihypertensive All Beta - Blockers Same?Document70 pagesEfficacy of Beta - Blockers For First - Line Antihypertensive All Beta - Blockers Same?Kishan Seth100% (1)
- Pacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPacemaker Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Goljan Transcribed NotesDocument59 pagesGoljan Transcribed NotesJiyeon JeonNo ratings yet
- Mapeh-10 Quater 1 ExamDocument5 pagesMapeh-10 Quater 1 ExamKIRBY ANN GALABINNo ratings yet
- Activity 9 Conducting Community Assessment (Designated Groups)Document5 pagesActivity 9 Conducting Community Assessment (Designated Groups)YongNo ratings yet
- Novilyn C. Pataray BSN - Ii Conjunctivitis: St. Paul College of Ilocos SurDocument1 pageNovilyn C. Pataray BSN - Ii Conjunctivitis: St. Paul College of Ilocos SurCharina Aubrey100% (2)
- IndianJPatholMicrobiol 2021 64 4 732 328590Document4 pagesIndianJPatholMicrobiol 2021 64 4 732 328590Shalini MalhotraNo ratings yet
- DDDT 124034 Bioequivalence Study of A New Sildenafil 100 MG Orodispersib - 041117Document10 pagesDDDT 124034 Bioequivalence Study of A New Sildenafil 100 MG Orodispersib - 041117firda maulidta hadadNo ratings yet
- Vitamin and Mineral DeficienciesDocument3 pagesVitamin and Mineral DeficienciesWeng Maesa Montemayor0% (1)
- Psychedelics Essay Final FinalDocument13 pagesPsychedelics Essay Final Finalapi-609530374No ratings yet
- Help Pedsurgeryafrica38Document6 pagesHelp Pedsurgeryafrica38madalinamihailescuNo ratings yet
- CCR3 4 831 PDFDocument7 pagesCCR3 4 831 PDFArmareality ArmarealityNo ratings yet
- Summative Test in Health (Drug Education) - 2019Document2 pagesSummative Test in Health (Drug Education) - 2019Melody Joy Amosco100% (2)
- Onsent To Hiropractic Reatment: BenefitsDocument2 pagesOnsent To Hiropractic Reatment: BenefitsRajender BishtNo ratings yet
- CyclophosphamideDocument3 pagesCyclophosphamideChen Boon TeyNo ratings yet
- Cvs Adjustments During Exercise by DR Sadia ZafarDocument23 pagesCvs Adjustments During Exercise by DR Sadia ZafarMudassar RoomiNo ratings yet
- Milk Borne Disease 2 (Eng) - 2012Document46 pagesMilk Borne Disease 2 (Eng) - 2012seviandha100% (1)
- The Power of Music - Musical Therapy To Treat AutismDocument1 pageThe Power of Music - Musical Therapy To Treat AutismMuh EminNo ratings yet
- Developmental DelayDocument79 pagesDevelopmental DelayNaveen KumarNo ratings yet
- NCM 112 Lesson3Document6 pagesNCM 112 Lesson3Trisha LopezNo ratings yet
- Stem CellDocument8 pagesStem Cellapi-220278259No ratings yet
- Pelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationDocument28 pagesPelvic Fractures: Part 1. Evaluation, Classification, and ResuscitationRiven OktavianNo ratings yet
- CVPDocument33 pagesCVPbharti PatelNo ratings yet
- Good BookDocument22 pagesGood BookWaqasAliNo ratings yet
- Modifying Adult IopaDocument2 pagesModifying Adult IopaPramodh PillaiNo ratings yet
- Corelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaDocument25 pagesCorelation of The Changes Between The Iridocorneal - Angle and Other Paramet E Rs at The Neovascular GlaucomaAJVAZI100% (1)
- Phenytoin: 100mg/2mL Injection, 30mg/5mL Oral MixtureDocument4 pagesPhenytoin: 100mg/2mL Injection, 30mg/5mL Oral MixturesindutrianaarifeniNo ratings yet
- SIGN Data Collection SheetsDocument6 pagesSIGN Data Collection Sheetsasi basseyNo ratings yet