Download as pptx, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Writing DSM 5 DiagnosisDocument2 pagesWriting DSM 5 Diagnosiscristina83% (6)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- TB Case PresDocument5 pagesTB Case PresAlwina May Parojinog BarlisanNo ratings yet
- Constipation With Scylabous Stools, Intermittent: IncreasedDocument1 pageConstipation With Scylabous Stools, Intermittent: IncreasedAlwina May Parojinog BarlisanNo ratings yet
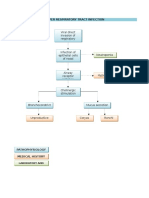
- Pathophysiology of Upper Respiratory Tract InfectionDocument1 pagePathophysiology of Upper Respiratory Tract InfectionAlwina May Parojinog BarlisanNo ratings yet
- Skin Grafts and Skin SubstitutesDocument5 pagesSkin Grafts and Skin SubstitutesAlwina May Parojinog BarlisanNo ratings yet
- Principles of ChemotherapyDocument31 pagesPrinciples of Chemotherapyigor100% (1)
- Pharmacoepidemiology Pharmacoepidemiology At3: Studies Using Automated Databases GDocument27 pagesPharmacoepidemiology Pharmacoepidemiology At3: Studies Using Automated Databases GRuth Vargas GonzalesNo ratings yet
- Relaxation Skills For Anxiety PDFDocument15 pagesRelaxation Skills For Anxiety PDFDomingo de Leon100% (1)
- Fdar Charting - Imh-1Document34 pagesFdar Charting - Imh-1Rekkusu MakeinuNo ratings yet
- DDH - Slide PresentationDocument28 pagesDDH - Slide PresentationSheilla RatnasariNo ratings yet
- Research Essay Final WeeblyDocument12 pagesResearch Essay Final Weeblyapi-519040910No ratings yet
- Trypophobia: Symptoms and CausesDocument5 pagesTrypophobia: Symptoms and CausesJessie Pasian Jr.No ratings yet
- How To Prescribe ENTRESTO To Your Patients: Dosing and Titration GuideDocument3 pagesHow To Prescribe ENTRESTO To Your Patients: Dosing and Titration GuideCorina DiaconescuNo ratings yet
- Patient Survey QuestionnaireDocument3 pagesPatient Survey QuestionnaireVivek DasNo ratings yet
- NSQHS Standards Sept2011Document80 pagesNSQHS Standards Sept2011Poonam Anala YeldandiNo ratings yet
- Toxic Shock SyndromeDocument10 pagesToxic Shock Syndromealice_lim01100% (1)
- Case File GERDDocument9 pagesCase File GERDMutiara Shifa100% (1)
- DermatomycosesDocument73 pagesDermatomycosessnylstlNo ratings yet
- Marine For Personal CareDocument4 pagesMarine For Personal CareDavid HungNo ratings yet
- Diabetes Mellitus Type 1Document310 pagesDiabetes Mellitus Type 1Shannon HopkinsNo ratings yet
- Cosmetic DentistryDocument52 pagesCosmetic DentistryPaul Chen60% (5)
- Self Assessment QuestionsDocument35 pagesSelf Assessment QuestionsAli QuwarahNo ratings yet
- Trauma Tapping Technique (TTT) : Purpose: Defuses and Desensitizes Traumatic Memories and ReDocument3 pagesTrauma Tapping Technique (TTT) : Purpose: Defuses and Desensitizes Traumatic Memories and ReMays Bags100% (1)
- Randomized Controlled TrialsDocument22 pagesRandomized Controlled TrialsJerome G ThampiNo ratings yet
- PANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstoneDocument44 pagesPANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstonePedro GouveiaNo ratings yet
- 059 ReikiDocument98 pages059 ReikiSanjay SoniNo ratings yet
- Consult QuestionnaireDocument2 pagesConsult Questionnairedmartin78No ratings yet
- Short Notes Sports MedicineDocument4 pagesShort Notes Sports MedicinesidorthoNo ratings yet
- Swach BharatDocument6 pagesSwach Bharatsoukumar8305No ratings yet
- Stress Management: By: Jun Flores Mark Ryan MacatuladDocument51 pagesStress Management: By: Jun Flores Mark Ryan MacatuladMark Ryan F. MacatuladNo ratings yet
- Urea Cycle DefectsDocument12 pagesUrea Cycle DefectsAleksandra RadonjićNo ratings yet
- Petronas Environment ManagementDocument10 pagesPetronas Environment ManagementCyril Angki100% (1)
- Internship Manual Pharm AideDocument6 pagesInternship Manual Pharm AideEspañola EloiseNo ratings yet
- 10 Myths About SchizophreniaDocument11 pages10 Myths About SchizophreniaQuennie Marie Moreno VillanuevaNo ratings yet