Download as pptx, pdf, or txt
You might also like
- Ophthalmology Clerks Revalida Review 2017Document94 pagesOphthalmology Clerks Revalida Review 2017Mara Medina - Borleo100% (1)
- OphthalmologyDocument144 pagesOphthalmologyrosaririsNo ratings yet
- CONJUNCTIVITISDocument67 pagesCONJUNCTIVITISNauli Panjaitan86% (7)
- Eye Problems: Dr. Gitalisa Andayani, SPMDocument88 pagesEye Problems: Dr. Gitalisa Andayani, SPMhasanajNo ratings yet
- When We Give Topical Ed in Red EyeDocument23 pagesWhen We Give Topical Ed in Red EyetaniamaulaniNo ratings yet
- Common Eye ProblemsDocument33 pagesCommon Eye ProblemsrobyalfNo ratings yet
- Special Senses 2014 - 1Document91 pagesSpecial Senses 2014 - 1Winz DolleteNo ratings yet
- Pterygium: Case Report By: Kiki Rizki Elvandari, S.Ked Preceptor: Dr. Rahmat SyuhadaDocument22 pagesPterygium: Case Report By: Kiki Rizki Elvandari, S.Ked Preceptor: Dr. Rahmat SyuhadaAnonymous prFao6No ratings yet
- Ophtha Case PresentationDocument51 pagesOphtha Case PresentationmailninakonNo ratings yet
- L2E Red EyeDocument39 pagesL2E Red EyeazraNo ratings yet
- The Red EyeDocument42 pagesThe Red EyeDenise CarbonellNo ratings yet
- SMF Mata Rsud DR - Hi. Abdoel Moeloek Bandar LampungDocument6 pagesSMF Mata Rsud DR - Hi. Abdoel Moeloek Bandar LampungNurulia AstriNo ratings yet
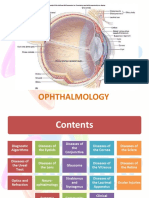
- Opt Halm OlogyDocument1 pageOpt Halm OlogyAnonymous q16bp7No ratings yet
- ConjungtivitisDocument86 pagesConjungtivitisIvo AfianiNo ratings yet
- Phase 4 Ophthalmology 2021-22Document62 pagesPhase 4 Ophthalmology 2021-22Olivia Genevieve El JassarNo ratings yet
- Prista Examination OpthalmologyDocument7 pagesPrista Examination OpthalmologyLamhotFarmaPurbaNo ratings yet
- Kelainan Kelopak Mata DKKDocument28 pagesKelainan Kelopak Mata DKKbinto akturusianoNo ratings yet
- Clinical App Red Eye Without Blurred VisionDocument38 pagesClinical App Red Eye Without Blurred VisionPriskila SamanthaNo ratings yet
- Uveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077Document23 pagesUveitis: Preceptor: Dr. Rahmad Syuhada, SP.M Wulandari, S.Ked 17360077widya melianitaNo ratings yet
- EedDocument70 pagesEedzihniyya471No ratings yet
- Ophthalmology NotesDocument79 pagesOphthalmology NotesWise AmroNo ratings yet
- Red EyeDocument54 pagesRed EyeT786 kharNo ratings yet
- # Diseases of ConjunctivaDocument4 pages# Diseases of Conjunctivaameerabest100% (1)
- CR Glaukoma Sek Ec UADocument12 pagesCR Glaukoma Sek Ec UAtiffanyalmndNo ratings yet
- Case of A.D.G.: San Beda University - College of Medicine Bautista, Bayona, Boñula Ophthalmology RotationDocument18 pagesCase of A.D.G.: San Beda University - College of Medicine Bautista, Bayona, Boñula Ophthalmology RotationRonel MarkNo ratings yet
- Differential Diagnosis of The Red Eye PDFDocument19 pagesDifferential Diagnosis of The Red Eye PDFAjeng PuspitasariNo ratings yet
- OphthoDocument27 pagesOphthoYavani KulasinghamNo ratings yet
- Conjunctivitis 120201025034 Phpapp02Document34 pagesConjunctivitis 120201025034 Phpapp02Ilham RafisNo ratings yet
- L3 Conjunctival DiseaseDocument70 pagesL3 Conjunctival DiseaseAlhNo ratings yet
- KalazionDocument21 pagesKalazioninh studioNo ratings yet
- Emergency Department Report: Thursday, August 15, 2019 AYU / DIM / RAT/ YD.,MD.,Opthal. ConsultDocument27 pagesEmergency Department Report: Thursday, August 15, 2019 AYU / DIM / RAT/ YD.,MD.,Opthal. ConsultdimasbudihartoNo ratings yet
- Case of Papillary Conjunctival ReactionDocument49 pagesCase of Papillary Conjunctival ReactionArlene FernandezNo ratings yet
- D.D of Red EyeDocument116 pagesD.D of Red Eyehassan daacadNo ratings yet
- Uvea (Hira fj'23)Document15 pagesUvea (Hira fj'23)Minahil ShahidNo ratings yet
- Case Resume 19 Jan Edit 2Document33 pagesCase Resume 19 Jan Edit 2Anangga AristantyoNo ratings yet
- Keratitis Ec Infiltrat OS: Case Presentation IDocument30 pagesKeratitis Ec Infiltrat OS: Case Presentation IAnonymous LxoYFc4mk9No ratings yet
- Uveitis Presentation Ridge HospitalDocument40 pagesUveitis Presentation Ridge Hospitalgideon A. owusuNo ratings yet
- RedEyescut3 PDFDocument46 pagesRedEyescut3 PDFriantimuharromiNo ratings yet
- Keratitis: By: Eriska Ratnawati 18360196Document14 pagesKeratitis: By: Eriska Ratnawati 18360196Diana Ulfah RahmanahNo ratings yet
- Important Points To Diagnose Scenarios of OphthalmologyDocument57 pagesImportant Points To Diagnose Scenarios of OphthalmologyHadra NuviNo ratings yet
- Diseases of The ConjunctivaDocument80 pagesDiseases of The ConjunctivaRatu CarissaNo ratings yet
- Diseases of The Uveal Tract 09Document24 pagesDiseases of The Uveal Tract 09somebody_ma100% (7)
- Mata Merah Visus TurunDocument27 pagesMata Merah Visus TurunErinNo ratings yet
- Lecture 3 Dreaded Red EyeDocument8 pagesLecture 3 Dreaded Red EyedrunkenwukongNo ratings yet
- Ocular Emergencies-Sept2013 PDFDocument22 pagesOcular Emergencies-Sept2013 PDFKaramsi Gopinath NaikNo ratings yet
- Friday Conference: Pediatrics Department, Songkhla HospitalDocument60 pagesFriday Conference: Pediatrics Department, Songkhla HospitalToutew ChanapatNo ratings yet
- James B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011Document9 pagesJames B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011qisthiNo ratings yet
- Ophthalmology Case Profoma - AgamDocument8 pagesOphthalmology Case Profoma - AgamHarshitha ANo ratings yet
- Differential Diagnosis Of: " Red Eye "Document41 pagesDifferential Diagnosis Of: " Red Eye "Ayu Permata SariNo ratings yet
- Ospe Ophthalmology CorrectedDocument55 pagesOspe Ophthalmology CorrectedGgah Vgggagagsg100% (1)
- Conjunctival Disorders OghreDocument59 pagesConjunctival Disorders Oghreteamtruth50No ratings yet
- The Red Eye: by DR Jawad Ahmad KhanDocument15 pagesThe Red Eye: by DR Jawad Ahmad KhanNabil AhmedNo ratings yet
- Red EyeDocument10 pagesRed Eyekopebe4040No ratings yet
- Ettinger CH 11 - Ophthalmic Manifestations of Systemic DiseaseDocument6 pagesEttinger CH 11 - Ophthalmic Manifestations of Systemic Diseasehalf_frozen_cho6435No ratings yet
- KatarakDocument19 pagesKatarakUtami WahyulianaNo ratings yet
- Ocular EmergDocument61 pagesOcular EmergKBR RS UNHAS100% (1)