Download as pptx, pdf, or txt
You might also like
- Freedom Food 1.0 Raw by Kate FlowersDocument86 pagesFreedom Food 1.0 Raw by Kate FlowersCoraIuliaAndrea100% (5)
- Case Study On MalariaDocument18 pagesCase Study On MalariaBie WeNna100% (4)
- Process Plant Layout - Seán Moran 1-2Document2 pagesProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
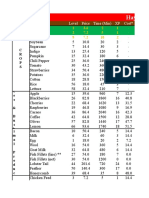
- Hay Day Price Profit AnalysisDocument112 pagesHay Day Price Profit AnalysisCunCunAlAndraNo ratings yet
- Hay Day Price Profit AnalysisDocument112 pagesHay Day Price Profit AnalysisCunCunAlAndraNo ratings yet
- IVF Table of Commonly Used IV SolutionsDocument3 pagesIVF Table of Commonly Used IV SolutionsKaloy KamaoNo ratings yet
- OSCE Manual 1Document35 pagesOSCE Manual 1Acess Meneses Reyes100% (2)
- Chronic DiarrheaDocument38 pagesChronic DiarrheaShujina ZainabNo ratings yet
- Chronic Diarrhea-HTKDocument63 pagesChronic Diarrhea-HTKcerenblgstrNo ratings yet
- Slide Kuliah Infectious DiareDocument75 pagesSlide Kuliah Infectious DiareFany Raihan PadilahNo ratings yet
- Small and Large IntestineDocument124 pagesSmall and Large IntestinemariahemnksNo ratings yet
- Infcetions Intestinal Protozoal InfectionsDocument40 pagesInfcetions Intestinal Protozoal InfectionsDr.P.NatarajanNo ratings yet
- Lecture Diarrhea and ConstipationDocument63 pagesLecture Diarrhea and ConstipationKrittin NaravejsakulNo ratings yet
- Week 7 - Pediatric GI DisturbancesDocument59 pagesWeek 7 - Pediatric GI DisturbancesLeyla GalyanoNo ratings yet
- Acute GastroenteritisDocument79 pagesAcute GastroenteritisZul Hisyam FikriNo ratings yet
- Dr. Arif Gunawan Teguh WDocument64 pagesDr. Arif Gunawan Teguh WarifgteguhNo ratings yet
- Acute GastroenteritisDocument39 pagesAcute Gastroenteritisslicvic169No ratings yet
- Communicable Disease Nursing Day2Document15 pagesCommunicable Disease Nursing Day2lindzy.amurao01No ratings yet
- Acute Gastroenteritis: DR Tjatur Winarsanto SPPDDocument34 pagesAcute Gastroenteritis: DR Tjatur Winarsanto SPPDMayiz Renata LimerseNo ratings yet
- 1 Approach To DiarrheaDocument37 pages1 Approach To DiarrheamusabNo ratings yet
- Pemicu 3 GITDocument143 pagesPemicu 3 GITMudita DewiNo ratings yet
- Gastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsDocument77 pagesGastrointestinal System Symptoms and Signs of Gastrointes Tinal ProblemsSindhu BabuNo ratings yet
- Acute Gastroenteritis in ChildrenDocument39 pagesAcute Gastroenteritis in ChildrenIra Mikkaella GenobisNo ratings yet
- Chronic Diarrhea Kuliah Pakar UnissulaDocument27 pagesChronic Diarrhea Kuliah Pakar UnissulaLuthfan HakimNo ratings yet
- Diarrhea: Dr. Ali A. Ramadhan M.B.CH.B., Fibms, Fkbms (G & H)Document27 pagesDiarrhea: Dr. Ali A. Ramadhan M.B.CH.B., Fibms, Fkbms (G & H)Ahmed NazarNo ratings yet
- Acute Gastroenteritis: An Approach: Paolo Aquino, M.D., M.P.HDocument24 pagesAcute Gastroenteritis: An Approach: Paolo Aquino, M.D., M.P.HNovandrew Selvian PNo ratings yet
- Disorders of Small IntestineDocument41 pagesDisorders of Small IntestineSamuel kuriaNo ratings yet
- Chronic Diarrhoea and MalabsorptionDocument25 pagesChronic Diarrhoea and MalabsorptionadelekeyusufNo ratings yet
- New Immunology FAE2016Document168 pagesNew Immunology FAE2016omarNo ratings yet
- Gastro Inflammatory Bowel DiseasesDocument39 pagesGastro Inflammatory Bowel DiseasesCherish Marie HurbodaNo ratings yet
- Case 2B (Group 8) Blok GITDocument74 pagesCase 2B (Group 8) Blok GITkheluwisNo ratings yet
- Acutegastroenteritispresentation Final 181205160545Document65 pagesAcutegastroenteritispresentation Final 181205160545DR MOHAMED HEALTH CHANNELNo ratings yet
- GlomerulonefritisDocument43 pagesGlomerulonefritisdian nofitaNo ratings yet
- CHRONIC DIRRHEA FinalDocument93 pagesCHRONIC DIRRHEA FinalAtifNo ratings yet
- Small & Large Bowel SlidesDocument17 pagesSmall & Large Bowel SlidesHunter ClontsNo ratings yet
- Kuliah Diare KronikDocument19 pagesKuliah Diare KronikMae Importers IncNo ratings yet
- Session 30 Bacillary Dysentery (Shigellosis)Document18 pagesSession 30 Bacillary Dysentery (Shigellosis)John MoshaNo ratings yet
- Acute Diarrhoea: - DefinitionDocument20 pagesAcute Diarrhoea: - DefinitionJam Knows RightNo ratings yet
- 112GIT BacteriologyDocument57 pages112GIT Bacteriologykane.20602No ratings yet
- Acute GastroenteritisDocument48 pagesAcute Gastroenteritisansam kamalNo ratings yet
- Diarrhea: Presented by Dwi Aprila Putri 12-083Document28 pagesDiarrhea: Presented by Dwi Aprila Putri 12-083Dwi Aprila PutriNo ratings yet
- Abdominal Mass/hepatosplenomegaly: David TateDocument10 pagesAbdominal Mass/hepatosplenomegaly: David TateYiddish hakeNo ratings yet
- DiarrheaDocument24 pagesDiarrheaash ashNo ratings yet
- CholeraDocument24 pagesCholeraLavanya Sivakumar100% (1)
- Diare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK UsuDocument37 pagesDiare Akut Pada Dewasa: Departemen Ilmu Penyakit Dalam FK Usuardi anharaksa yusuf100% (1)
- Acute Diarrhea (Replica)Document12 pagesAcute Diarrhea (Replica)najeebNo ratings yet
- Diarrhea: Group 4: Surya Patricya Serikat Niscaya Theresia Yuni Venggy Reylandhie Yustina NayDocument15 pagesDiarrhea: Group 4: Surya Patricya Serikat Niscaya Theresia Yuni Venggy Reylandhie Yustina NayvenggyNo ratings yet
- "Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForDocument84 pages"Gosh, Mrs. Doubtfire You Look Pale": Fire" in Television at The Emergency Departement You Worked ForAngela Kristiana IntanNo ratings yet
- Acute GastroEnteritisDocument27 pagesAcute GastroEnteritisRahul MandhanNo ratings yet
- Evaluation of Chronic DiarrhoeaDocument31 pagesEvaluation of Chronic Diarrhoeaadamu mohammadNo ratings yet
- Pead 3 - Abdominal Pain and VommitingDocument22 pagesPead 3 - Abdominal Pain and Vommitingbbyes100% (1)
- Inflammatory Bowel DiseaseDocument40 pagesInflammatory Bowel DiseaseSK TalkNo ratings yet
- PowerpointDocument29 pagesPowerpointpisces200910No ratings yet
- 07c. Non Neoplastic Disease of The Small and Large IntestineDocument49 pages07c. Non Neoplastic Disease of The Small and Large Intestine21701101016 - Juliana Ayu NugrahaNo ratings yet
- Junior Intern Review - Oral Revalida 2016Document170 pagesJunior Intern Review - Oral Revalida 2016Cyrus ZalameaNo ratings yet
- PA GI Tract Skuad Tandingan Elnineno!Document281 pagesPA GI Tract Skuad Tandingan Elnineno!Arsya AliNo ratings yet
- Chronic Diarrhea and MalabsorptionDocument77 pagesChronic Diarrhea and MalabsorptionDragosAurNo ratings yet
- 5.5 GI Disorders Dr. Jison 2022Document72 pages5.5 GI Disorders Dr. Jison 2022Monique BorresNo ratings yet
- GIT 2021 Lect17Document49 pagesGIT 2021 Lect17Nikkole PhalulaNo ratings yet
- DiarrhoeaDocument14 pagesDiarrhoeaNamun Sibora BoraNo ratings yet
- Diarrhea: Dr. Haifa Yagoub OsmanDocument23 pagesDiarrhea: Dr. Haifa Yagoub OsmanAlex SamNo ratings yet
- Report On AmoebiasisDocument36 pagesReport On Amoebiasisrhimineecat71No ratings yet
- Small Bowel and Large Bowel DisordersDocument43 pagesSmall Bowel and Large Bowel DisordersDanielle FosterNo ratings yet
- ICC-2 (172) History Taking and Symptomatology in Lower GIT DiseaseDocument23 pagesICC-2 (172) History Taking and Symptomatology in Lower GIT Diseaseabdulrhman essamNo ratings yet
- Disorders of The Genitourinary SystemDocument49 pagesDisorders of The Genitourinary SystemYemaya84No ratings yet
- Process Plant Layout - Seán Moran 3-4Document2 pagesProcess Plant Layout - Seán Moran 3-4CunCunAlAndraNo ratings yet
- DA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DEDocument14 pagesDA38 Safety Data Shett FAME (Fatty Acid Methyl Ester) V4 - en - DECunCunAlAndraNo ratings yet
- GF Signet 515 2536 Manual01Document1 pageGF Signet 515 2536 Manual01CunCunAlAndraNo ratings yet
- Management Gathering 0718 - Distribution - v5 CoverDocument1 pageManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraNo ratings yet
- Early Liver TransplantationDocument11 pagesEarly Liver TransplantationCunCunAlAndraNo ratings yet
- Problem 5 Git: Ivan MichaelDocument68 pagesProblem 5 Git: Ivan MichaelCunCunAlAndraNo ratings yet
- Breather Valve - Pressure-Vaccuem Relief ValveDocument2 pagesBreather Valve - Pressure-Vaccuem Relief Valvevphor85No ratings yet
- RicoDocument62 pagesRicoCunCunAlAndraNo ratings yet
- Syzygium Samarangese (Macopa) Fruit As A (SIP)Document76 pagesSyzygium Samarangese (Macopa) Fruit As A (SIP)Clarisse DacasinNo ratings yet
- Acute GastroenteritisDocument54 pagesAcute GastroenteritisVincent LaranjoNo ratings yet
- Assessment Using Functional Health Patterns: AppendixDocument16 pagesAssessment Using Functional Health Patterns: AppendixNalzaro Emyril89% (19)
- So My Cat Has Chronic Kidney DiseaseDocument2 pagesSo My Cat Has Chronic Kidney DiseaseNur Alisya Hasnul HadiNo ratings yet
- Drug Study CefuroximeDocument9 pagesDrug Study CefuroximeRio Ramon HilarioNo ratings yet
- 2016 Heat Stress CampaignDocument66 pages2016 Heat Stress CampaignGiridharan Venkatesh100% (2)
- Wildlife Emergency and Critical CareDocument14 pagesWildlife Emergency and Critical CareRayssa PereiraNo ratings yet
- Breast Mass Bilateral To Consider FibroadenomaDocument5 pagesBreast Mass Bilateral To Consider FibroadenomaYum CNo ratings yet
- NCP DehydrationDocument4 pagesNCP DehydrationYnah Sayoc100% (2)
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale EvaluationMiss GNo ratings yet
- Pediatic Case Presentation FinalDocument26 pagesPediatic Case Presentation FinalJyoti Prem UttamNo ratings yet
- Fluids and Electrolytes NotesDocument17 pagesFluids and Electrolytes NotesFaye G.No ratings yet
- A Randomized Trial To Assess The Potential of Different Beverages To Affect Hydration 2016 (Cafe)Document7 pagesA Randomized Trial To Assess The Potential of Different Beverages To Affect Hydration 2016 (Cafe)Cristian YanezNo ratings yet
- The Miracle Morning For Entrepreneurs Elevate Your SELF To Elevate Your BUSINESS (Hal Elrod, Cameron Herold)Document229 pagesThe Miracle Morning For Entrepreneurs Elevate Your SELF To Elevate Your BUSINESS (Hal Elrod, Cameron Herold)naziaNo ratings yet
- Survival 101 The Essential Guide To Saving Your Own Life in A Disaster, 2eDocument40 pagesSurvival 101 The Essential Guide To Saving Your Own Life in A Disaster, 2ehkcast100% (1)
- Physical Education and Health: Quarter 1-Module 3Document20 pagesPhysical Education and Health: Quarter 1-Module 3Jetrice TanguihanNo ratings yet
- Nausea and Vomiting PDFDocument8 pagesNausea and Vomiting PDFRoosita Arbaane SafitriNo ratings yet
- A Case Study On AGE Part 3Document2 pagesA Case Study On AGE Part 3pangee489No ratings yet
- Please, Take The Big 5 of The Most Disease That Occure in Your Workplace and Make A Resume From That SituationDocument8 pagesPlease, Take The Big 5 of The Most Disease That Occure in Your Workplace and Make A Resume From That Situationtrah starkNo ratings yet
- Psychiatric Nursing Diagnosis List Based On The Nanda-I Nursing Diagnoses (NDS)Document14 pagesPsychiatric Nursing Diagnosis List Based On The Nanda-I Nursing Diagnoses (NDS)Tania sharmaNo ratings yet
- Acute Diarrhea in ChildrenDocument53 pagesAcute Diarrhea in ChildrenKishore ChandkiNo ratings yet
- NCM 109 Case Study - Sir JesusDocument25 pagesNCM 109 Case Study - Sir JesusLance RaphaelNo ratings yet
- Perioperative Gyn Obs Fluid & Electrolytes ManagementDocument60 pagesPerioperative Gyn Obs Fluid & Electrolytes Managementzamurd76100% (1)
- Diarrhea Health Education FinaleeeeDocument12 pagesDiarrhea Health Education FinaleeeeSoumya RajeswariNo ratings yet
- Recording of Fluid Balance Intake-Output PolicyDocument7 pagesRecording of Fluid Balance Intake-Output PolicyRao Rizwan ShakoorNo ratings yet
- Nursing-Care-Plan-Template - PDF p2Document3 pagesNursing-Care-Plan-Template - PDF p2Franz keannu Libunao GonzalesNo ratings yet