Download as ppt, pdf, or txt
You might also like
- Emergency in OrthopaedicDocument41 pagesEmergency in Orthopaedicmade dollyNo ratings yet
- Access PortacathDocument3 pagesAccess Portacathbrigette_lagatNo ratings yet
- Sialadenitis: K.Abhinaya. Bds 3 YearDocument14 pagesSialadenitis: K.Abhinaya. Bds 3 YearAsline JesicaNo ratings yet
- Patofisiologi Nyeri Pada Kelainan BiliodigestifDocument25 pagesPatofisiologi Nyeri Pada Kelainan Biliodigestifbocah_britpopNo ratings yet
- Presentation 1Document25 pagesPresentation 1Nihar ShahNo ratings yet
- To Perforasi GasterDocument27 pagesTo Perforasi GasterPuthu BelegugNo ratings yet
- Primary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewDocument17 pagesPrimary and Secondary Survey-Dr. Joan Willy Ansar, Span - PPT NewPrabu Tirta AjiNo ratings yet
- 24 Olsen Variations ParotidectomyDocument33 pages24 Olsen Variations ParotidectomyAngga Witra NandaNo ratings yet
- Abdominal Distention inDocument45 pagesAbdominal Distention inArif Rahman DmNo ratings yet
- FOM STUDY GUIDE 3rd Block 1Document3 pagesFOM STUDY GUIDE 3rd Block 1Bernadine Cruz Par100% (1)
- Breast Cancer: Katherine Macgillivray & Melissa PoirierDocument62 pagesBreast Cancer: Katherine Macgillivray & Melissa PoirierJonathan Darell WijayaNo ratings yet
- PALATOPLASTYDocument14 pagesPALATOPLASTYretha_retha93No ratings yet
- Xanthogranulomatous PyelonephritisDocument14 pagesXanthogranulomatous PyelonephritisalaaNo ratings yet
- To HerniotomiDocument16 pagesTo HerniotomikawaishoneNo ratings yet
- Cervicofacial LymphangiomasDocument11 pagesCervicofacial LymphangiomasCharmila Sari100% (1)
- Craniotomy FlapsDocument41 pagesCraniotomy FlapsKaramsi Gopinath NaikNo ratings yet
- Penetrating Chest InjuryDocument33 pagesPenetrating Chest InjuryJARRIE BADJIENo ratings yet
- Cara Mengukur Tekanan IntrakompartemenDocument2 pagesCara Mengukur Tekanan Intrakompartemenfatimah putriNo ratings yet
- EGDT SepsisDocument8 pagesEGDT Sepsissiti fatmalaNo ratings yet
- Infeksi NosokomialDocument29 pagesInfeksi NosokomialAlunaficha Melody KiraniaNo ratings yet
- Tracheostomy: Indications and ProcedureDocument10 pagesTracheostomy: Indications and ProcedureAinur AbdrakhmanovaNo ratings yet
- Acute Scrotum 231016 PDFDocument50 pagesAcute Scrotum 231016 PDFDany Dias100% (1)
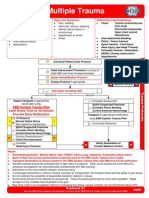
- Multiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationDocument1 pageMultiple Trauma: EMS System Trauma Plan Limit Scene Time To 10 Minutes Provide Early NotificationKelly JacksonNo ratings yet
- Trauma Stensen DuctDocument30 pagesTrauma Stensen DuctDenny SetyadiNo ratings yet
- Anatomy and Physiology of ThyroidDocument74 pagesAnatomy and Physiology of ThyroidSajid NadafNo ratings yet
- Tumor Buli BuliDocument6 pagesTumor Buli Buliputri wulandariNo ratings yet
- AdhesiolisisDocument22 pagesAdhesiolisisRisal WintokoNo ratings yet
- 2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesDocument11 pages2013 - Pancreaticoduodenectomy (Whipple Procedure) TechniquesOlteanu IonutNo ratings yet
- BPHDocument10 pagesBPHMichelle SalimNo ratings yet
- Foreign Body IN Oropharynx OR EsophagusDocument36 pagesForeign Body IN Oropharynx OR EsophagusDoodNo ratings yet
- HerniaDocument61 pagesHerniaAhmed HassanNo ratings yet
- Fraktur CollesDocument18 pagesFraktur CollesBerliana Kurniawati Nur HudaNo ratings yet
- Anal Fissure: BY Alisha SaleemDocument7 pagesAnal Fissure: BY Alisha Saleemashar khanNo ratings yet
- EmpyemaDocument17 pagesEmpyemadeo_gratias14No ratings yet
- Trauma BuliDocument32 pagesTrauma BulimoonlightsoantaNo ratings yet
- Chest TubeDocument8 pagesChest TubeTaufik Nur YahyaNo ratings yet
- Tracheostomy: Berlian Chevi A. 20184010030Document26 pagesTracheostomy: Berlian Chevi A. 20184010030Berlian Chevi e'Xgepz ThrearsansNo ratings yet
- Anal Stenosis and Mucosal EctropionDocument7 pagesAnal Stenosis and Mucosal EctropionpologroNo ratings yet
- ColostomyDocument45 pagesColostomydrqiekiNo ratings yet
- Wound de His Cence FinalDocument26 pagesWound de His Cence Finaldanil armandNo ratings yet
- Acute Abdomen and PeritonitisDocument17 pagesAcute Abdomen and PeritonitisAnisaPratiwiArumningsihNo ratings yet
- Otologic Manifestation of Systemic DiseaseDocument57 pagesOtologic Manifestation of Systemic DiseaseHERIZALNo ratings yet
- Ivc InjuryDocument17 pagesIvc InjuryAnishChowdhuryNo ratings yet
- Hernia UmbilikalisDocument16 pagesHernia UmbilikalisWibhuti EmrikoNo ratings yet
- Pterigium: Dr. Purnamanita Syawal, SPM, MarsDocument39 pagesPterigium: Dr. Purnamanita Syawal, SPM, Marsyayat muhammadNo ratings yet
- Harvesting STSG: I Gusti Ayu Putri PurwanthiDocument22 pagesHarvesting STSG: I Gusti Ayu Putri PurwanthiPutri PurwanthiNo ratings yet
- Differential Diagnosis Pain Right HypochondriumDocument35 pagesDifferential Diagnosis Pain Right HypochondriumDrArish Mahmood100% (1)
- DR - Bambang-Damage Control OrthopaedicsDocument37 pagesDR - Bambang-Damage Control OrthopaedicsbadliinaaNo ratings yet
- PCNDocument3 pagesPCNAzirah TawangNo ratings yet
- Nervus Laryngeus RecurrensDocument5 pagesNervus Laryngeus RecurrensAri Julian SaputraNo ratings yet
- Wound DehiscenceDocument3 pagesWound DehiscencesmileyginaaNo ratings yet
- Surgical Site Infection: Dr. Maryam. Surgical Unit 3Document22 pagesSurgical Site Infection: Dr. Maryam. Surgical Unit 3med stuNo ratings yet
- Bartholin's Cyst/AbscessDocument6 pagesBartholin's Cyst/AbscessJane NathaniaNo ratings yet
- Akut SkrotumDocument26 pagesAkut SkrotumToni PinemNo ratings yet
- Fraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapDocument26 pagesFraktur Tulang: Husnul Author Bag. Bedah RSUD CilacapUmi YatunNo ratings yet
- Systemic Lupus Eritematus Kuliah KlerkDocument76 pagesSystemic Lupus Eritematus Kuliah KlerkAnonymous y6NmP9NHkYNo ratings yet
- Odontogenic Maxillary Sinusitis. Etiology, Anatomy, Pathogenesis, Classification, Clinical Picture, Diagnostics, Treatment and ComplicationsDocument36 pagesOdontogenic Maxillary Sinusitis. Etiology, Anatomy, Pathogenesis, Classification, Clinical Picture, Diagnostics, Treatment and ComplicationsАлександр ВолошанNo ratings yet
- Dr. Moch. Syahroni Far, Spu, M.KesDocument38 pagesDr. Moch. Syahroni Far, Spu, M.KesNd EyeNo ratings yet
- Stenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandStenosing Tenosynovitis, (Trigger Finger) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Chronic Suppurative Otitis Media (CSOM)Document31 pagesChronic Suppurative Otitis Media (CSOM)Mimo HemadNo ratings yet