
Pharmacodynamics: Dr. Bayu Lestari Pharmacology Laboratory Medical Faculty of Brawijaya University
Pharmacodynamics: Dr. Bayu Lestari Pharmacology Laboratory Medical Faculty of Brawijaya University
You might also like
- BIOSCI 203 - 2021 Semester Two - Course OutlineDocument6 pagesBIOSCI 203 - 2021 Semester Two - Course OutlineFatemeh ArefianNo ratings yet
- The Science of TasteDocument107 pagesThe Science of TasteAnonymous U9aZZmeNrENo ratings yet
- Signal Transduction FinalDocument46 pagesSignal Transduction FinalTanvir FahimNo ratings yet
- PharmacodynamicsDocument13 pagesPharmacodynamicsNURUL AFIQAH IZZATI BINTI ROSLANNo ratings yet
- Pharmacodynamics: DR Narendra KumarDocument76 pagesPharmacodynamics: DR Narendra Kumarperala vinaykumarNo ratings yet
- Unacademy 3 PDFDocument24 pagesUnacademy 3 PDFANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- Pharmacodynamics: DR Narendra KumarDocument76 pagesPharmacodynamics: DR Narendra KumarsivaNo ratings yet
- Pharmaco DynamicsDocument65 pagesPharmaco Dynamicsorogadejulius5050No ratings yet
- Metabotropic: The Second Major Type of Neurotransmitter ReceptorDocument17 pagesMetabotropic: The Second Major Type of Neurotransmitter ReceptorChian WrightNo ratings yet
- Receptor MechanismsDocument2 pagesReceptor Mechanismsnawafalghamdi20No ratings yet
- PharmacodynamicsDocument93 pagesPharmacodynamicsRuby Ann DimayugaNo ratings yet
- Lecture 2Document28 pagesLecture 2Ushan KabirNo ratings yet
- Pharmacodynamics - Receptors 2016 Membrane ReceptorsDocument25 pagesPharmacodynamics - Receptors 2016 Membrane ReceptorsLilian EdeniNo ratings yet
- Unacademy 2 PDFDocument26 pagesUnacademy 2 PDFANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- ReceptorsDocument44 pagesReceptorsAbiy AliyeNo ratings yet
- PharmacoDocument62 pagesPharmacoVaibhav KaroliyaNo ratings yet
- GPCR 160211124029Document83 pagesGPCR 160211124029JuhiJahan AmanullahNo ratings yet
- Govt. Digvijay Autonomous P. G. College Raj-Nandgaon (C. G.)Document27 pagesGovt. Digvijay Autonomous P. G. College Raj-Nandgaon (C. G.)oliver senNo ratings yet
- Mechanism of Hormone ActionDocument54 pagesMechanism of Hormone ActionDr. Tapan Kr. Dutta100% (1)
- Receptors Ionchannel TransporterDocument58 pagesReceptors Ionchannel TransporterDeepu Vijay100% (1)
- G-Protein Coupled ReceptorsDocument8 pagesG-Protein Coupled ReceptorsHyunji KimNo ratings yet
- Module 5Document108 pagesModule 5alshalabinezardonia96No ratings yet
- Receptors and Determinants of Biologic ResponseDocument38 pagesReceptors and Determinants of Biologic Responsedhainey100% (1)
- 4.2 Mechanism of Action of Hormones-40Document39 pages4.2 Mechanism of Action of Hormones-40Namomsa W.No ratings yet
- ACyMSC - 03-Surface ReceptorsDocument54 pagesACyMSC - 03-Surface ReceptorsEsther NavarroNo ratings yet
- Cell SignallingDocument37 pagesCell SignallingSreekarWunnava100% (1)
- Receptors Its TypesDocument33 pagesReceptors Its TypesjunaidkhanhassNo ratings yet
- Pharmacodynamics 2023 2Document44 pagesPharmacodynamics 2023 2SristeeNo ratings yet
- Cell SignalingDocument75 pagesCell SignalingjhanvisNo ratings yet
- FarmakodinamikDocument44 pagesFarmakodinamikHarri HardiNo ratings yet
- A Seminar Presentation On Mechanism of Drug ActionDocument40 pagesA Seminar Presentation On Mechanism of Drug Actionbellatrix aliaNo ratings yet
- Cell SignalingDocument26 pagesCell SignalingJasir KhanNo ratings yet
- SignalingDocument54 pagesSignalingMaria LippertNo ratings yet
- Receptor EnzymeDocument29 pagesReceptor EnzymeA1606SucithaNo ratings yet
- BBM CellSignaling Lect 04-Ch03Document32 pagesBBM CellSignaling Lect 04-Ch03mimo el crackNo ratings yet
- Chemical Signal: Hormone 1: Biosignaling (WEEK 2)Document27 pagesChemical Signal: Hormone 1: Biosignaling (WEEK 2)Fenny Aulia SugianaNo ratings yet
- 037 - Endocrinology Physiology) Receptor PathwaysDocument4 pages037 - Endocrinology Physiology) Receptor Pathwaysیوسف رمضانNo ratings yet
- Pharmacodynamics 1Document65 pagesPharmacodynamics 1Kavya SivakarthikeyanNo ratings yet
- DR Dewi Farmakologi Pada Gangguan Neurologi - Maret 2021 DewiDocument81 pagesDR Dewi Farmakologi Pada Gangguan Neurologi - Maret 2021 DewiclarissaNo ratings yet
- Class 14. Signal Transduction: A Cascade of Events Within A Cell Translates Signals Into Cellular ResponsesDocument7 pagesClass 14. Signal Transduction: A Cascade of Events Within A Cell Translates Signals Into Cellular ResponsesLuis David Morocho PogoNo ratings yet
- Receptors: Receptor Tyrosine Kinases (RTK)Document5 pagesReceptors: Receptor Tyrosine Kinases (RTK)Safiya JamesNo ratings yet
- Molecular Pharmacology of Cell SignlingDocument100 pagesMolecular Pharmacology of Cell SignlingMohanad Al-BayatiNo ratings yet
- ميحرلا نمحرلا ﷲ مسب In the name of Allah the most Gracious and the most mercifulDocument32 pagesميحرلا نمحرلا ﷲ مسب In the name of Allah the most Gracious and the most mercifulAsmaa El SawyNo ratings yet
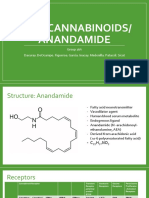
- Endocannabinoids/ Anandamide: Group 16A Dacuray. Deocampo. Figueroa. Garcia. Inacay. Medenilla. Patacsil. SicatDocument10 pagesEndocannabinoids/ Anandamide: Group 16A Dacuray. Deocampo. Figueroa. Garcia. Inacay. Medenilla. Patacsil. SicatJustin Garcia100% (1)
- F22 MCB 2050 Lecture 10 - Signal TransductionDocument28 pagesF22 MCB 2050 Lecture 10 - Signal TransductionNO VIDEOSNo ratings yet
- Cell and Molecular Biology: Gerald KarpDocument53 pagesCell and Molecular Biology: Gerald Karppat ongNo ratings yet
- Pharmacodynamics Mechanisms of Drug ActionDocument47 pagesPharmacodynamics Mechanisms of Drug ActioneciNo ratings yet
- Types of Signalling Pathway GPCR Pathway Normal and DysregulatedDocument78 pagesTypes of Signalling Pathway GPCR Pathway Normal and Dysregulatedapi-251915360No ratings yet
- General Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalDocument58 pagesGeneral Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalYashasv BhatnagarNo ratings yet
- SignalingDocument44 pagesSignalingMOCHILNo ratings yet
- Pharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDocument64 pagesPharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDigvijayaNo ratings yet
- NeurotransmittersDocument36 pagesNeurotransmittersmk5370096No ratings yet
- Day 22 Signaling 1: General Concepts and cAMP Pathway: - You Should Be Able To ExplainDocument20 pagesDay 22 Signaling 1: General Concepts and cAMP Pathway: - You Should Be Able To Explainshouq huusainNo ratings yet
- Chapter 1 - Hormones and Hormone ActionDocument42 pagesChapter 1 - Hormones and Hormone Action張宏軒No ratings yet
- Lehninger - PPT - ch12 AllDocument93 pagesLehninger - PPT - ch12 Allmissoni0408No ratings yet
- Prinsip Aksi ObatDocument49 pagesPrinsip Aksi ObatyulinarsihNo ratings yet
- Signal Transduction Pathways: Pratt & Cornely, Chapter 10Document23 pagesSignal Transduction Pathways: Pratt & Cornely, Chapter 10Brother GeorgeNo ratings yet
- Transmembrane and Kinase ReceptorsDocument20 pagesTransmembrane and Kinase ReceptorssasqiaNo ratings yet
- MD ch5Document27 pagesMD ch5malake.a13cj7No ratings yet
- Chapter 9 BIO 1510Document26 pagesChapter 9 BIO 1510Chachi CNo ratings yet
- L20 Signal Transduction and Mechanism of Hormone ActionDocument51 pagesL20 Signal Transduction and Mechanism of Hormone Actionyebadem228No ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- Apoptosis Lecture 2023 2024Document115 pagesApoptosis Lecture 2023 2024Thái AnNo ratings yet
- Syllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesDocument92 pagesSyllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesAubal ShaubalNo ratings yet
- 2010 A Level H2 Biology P2 AnsDocument8 pages2010 A Level H2 Biology P2 AnsImagreenbucklegirl SGNo ratings yet
- 59c566785b913 PEMFhowitworksDocument20 pages59c566785b913 PEMFhowitworksWalter SchmittNo ratings yet
- Regulatory Network of Genes Associated With Stimuli Sensing Signal Transduction and Physiological Transformation of Appressorium in Magnaporthe Oryzae PDFDocument13 pagesRegulatory Network of Genes Associated With Stimuli Sensing Signal Transduction and Physiological Transformation of Appressorium in Magnaporthe Oryzae PDFAmalNo ratings yet
- Legend PlexDocument12 pagesLegend Plexkike1790No ratings yet
- Acquisition of A Hybrid E M State Is Essential For Tumorigenicity of Basal Breast Cancer CellsDocument12 pagesAcquisition of A Hybrid E M State Is Essential For Tumorigenicity of Basal Breast Cancer CellsgangligonNo ratings yet
- Functions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1Document33 pagesFunctions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1rayanahfedanNo ratings yet
- Second Messenger SystemsModDocument49 pagesSecond Messenger SystemsModganotNo ratings yet
- M.Sc. - Molecular Human GeneticsDocument32 pagesM.Sc. - Molecular Human GeneticsSiman SimanNo ratings yet
- R J Epstein-Human Molecular Biology - An Introduction To The Molecular Basis of Health and Disease-Cambridge University Press (2002)Document655 pagesR J Epstein-Human Molecular Biology - An Introduction To The Molecular Basis of Health and Disease-Cambridge University Press (2002)Libros a Color ConceNo ratings yet
- Apoptosis Cancer Signaling PathwaysDocument1 pageApoptosis Cancer Signaling PathwayssyafikaNo ratings yet
- General Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalDocument58 pagesGeneral Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalYashasv BhatnagarNo ratings yet
- Semester 1 Rev 2019Document33 pagesSemester 1 Rev 2019Anthony WilsonNo ratings yet
- Gpcrs and CancervistaDocument45 pagesGpcrs and CancervistapriyaaNo ratings yet
- Gpat 2023Document11 pagesGpat 2023Bobi JiNo ratings yet
- G Protein Coupled Receptor (GPCR) Adenylyl Cyclase: Ligand BindingDocument3 pagesG Protein Coupled Receptor (GPCR) Adenylyl Cyclase: Ligand BindingPanda DaoNo ratings yet
- Syndecans in Inflammation at A Glance: Sandeep GopalDocument8 pagesSyndecans in Inflammation at A Glance: Sandeep GopalYeni PuspitasariNo ratings yet
- Lecture-Cell Membranes and SignalingDocument64 pagesLecture-Cell Membranes and SignalingDiabyNo ratings yet
- Inflammation Panel ContentDocument2 pagesInflammation Panel ContentBogdan A. GireadăNo ratings yet
- Endocrine Physiology: Felix E. Grissom, Ph.D. 2219 Adams Building Howard University Tel. (202) 806-4512Document30 pagesEndocrine Physiology: Felix E. Grissom, Ph.D. 2219 Adams Building Howard University Tel. (202) 806-4512Inis LeahyNo ratings yet
- Physical Exercise and Epigenetic Modifications in Skeletal MuscleDocument15 pagesPhysical Exercise and Epigenetic Modifications in Skeletal MuscleAmin AminiNo ratings yet
- B.Sc. Cardiac Perfusion Technology FinalDocument32 pagesB.Sc. Cardiac Perfusion Technology FinalTanisha ShaikhNo ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- Cancer Drug Discovery - Science and History-Springer Netherlands (Libro-2016)Document286 pagesCancer Drug Discovery - Science and History-Springer Netherlands (Libro-2016)ELMERNo ratings yet
- Funcional Analysis of PTHIR Variants Found in Primary Failure of EruptionDocument8 pagesFuncional Analysis of PTHIR Variants Found in Primary Failure of EruptionvivgaitanNo ratings yet
- Cytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014Document101 pagesCytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014ANJU0709No ratings yet
- Pharmacology of Central Nervous SystemDocument20 pagesPharmacology of Central Nervous SystemAngelic khan100% (1)






















































































Download as pptx, pdf, or txt
You might also like
- BIOSCI 203 - 2021 Semester Two - Course OutlineDocument6 pagesBIOSCI 203 - 2021 Semester Two - Course OutlineFatemeh ArefianNo ratings yet
- The Science of TasteDocument107 pagesThe Science of TasteAnonymous U9aZZmeNrENo ratings yet
- Signal Transduction FinalDocument46 pagesSignal Transduction FinalTanvir FahimNo ratings yet
- PharmacodynamicsDocument13 pagesPharmacodynamicsNURUL AFIQAH IZZATI BINTI ROSLANNo ratings yet
- Pharmacodynamics: DR Narendra KumarDocument76 pagesPharmacodynamics: DR Narendra Kumarperala vinaykumarNo ratings yet
- Unacademy 3 PDFDocument24 pagesUnacademy 3 PDFANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- Pharmacodynamics: DR Narendra KumarDocument76 pagesPharmacodynamics: DR Narendra KumarsivaNo ratings yet
- Pharmaco DynamicsDocument65 pagesPharmaco Dynamicsorogadejulius5050No ratings yet
- Metabotropic: The Second Major Type of Neurotransmitter ReceptorDocument17 pagesMetabotropic: The Second Major Type of Neurotransmitter ReceptorChian WrightNo ratings yet
- Receptor MechanismsDocument2 pagesReceptor Mechanismsnawafalghamdi20No ratings yet
- PharmacodynamicsDocument93 pagesPharmacodynamicsRuby Ann DimayugaNo ratings yet
- Lecture 2Document28 pagesLecture 2Ushan KabirNo ratings yet
- Pharmacodynamics - Receptors 2016 Membrane ReceptorsDocument25 pagesPharmacodynamics - Receptors 2016 Membrane ReceptorsLilian EdeniNo ratings yet
- Unacademy 2 PDFDocument26 pagesUnacademy 2 PDFANUPAM ANAND KUMAR PANDEY MBA-INo ratings yet
- ReceptorsDocument44 pagesReceptorsAbiy AliyeNo ratings yet
- PharmacoDocument62 pagesPharmacoVaibhav KaroliyaNo ratings yet
- GPCR 160211124029Document83 pagesGPCR 160211124029JuhiJahan AmanullahNo ratings yet
- Govt. Digvijay Autonomous P. G. College Raj-Nandgaon (C. G.)Document27 pagesGovt. Digvijay Autonomous P. G. College Raj-Nandgaon (C. G.)oliver senNo ratings yet
- Mechanism of Hormone ActionDocument54 pagesMechanism of Hormone ActionDr. Tapan Kr. Dutta100% (1)
- Receptors Ionchannel TransporterDocument58 pagesReceptors Ionchannel TransporterDeepu Vijay100% (1)
- G-Protein Coupled ReceptorsDocument8 pagesG-Protein Coupled ReceptorsHyunji KimNo ratings yet
- Module 5Document108 pagesModule 5alshalabinezardonia96No ratings yet
- Receptors and Determinants of Biologic ResponseDocument38 pagesReceptors and Determinants of Biologic Responsedhainey100% (1)
- 4.2 Mechanism of Action of Hormones-40Document39 pages4.2 Mechanism of Action of Hormones-40Namomsa W.No ratings yet
- ACyMSC - 03-Surface ReceptorsDocument54 pagesACyMSC - 03-Surface ReceptorsEsther NavarroNo ratings yet
- Cell SignallingDocument37 pagesCell SignallingSreekarWunnava100% (1)
- Receptors Its TypesDocument33 pagesReceptors Its TypesjunaidkhanhassNo ratings yet
- Pharmacodynamics 2023 2Document44 pagesPharmacodynamics 2023 2SristeeNo ratings yet
- Cell SignalingDocument75 pagesCell SignalingjhanvisNo ratings yet
- FarmakodinamikDocument44 pagesFarmakodinamikHarri HardiNo ratings yet
- A Seminar Presentation On Mechanism of Drug ActionDocument40 pagesA Seminar Presentation On Mechanism of Drug Actionbellatrix aliaNo ratings yet
- Cell SignalingDocument26 pagesCell SignalingJasir KhanNo ratings yet
- SignalingDocument54 pagesSignalingMaria LippertNo ratings yet
- Receptor EnzymeDocument29 pagesReceptor EnzymeA1606SucithaNo ratings yet
- BBM CellSignaling Lect 04-Ch03Document32 pagesBBM CellSignaling Lect 04-Ch03mimo el crackNo ratings yet
- Chemical Signal: Hormone 1: Biosignaling (WEEK 2)Document27 pagesChemical Signal: Hormone 1: Biosignaling (WEEK 2)Fenny Aulia SugianaNo ratings yet
- 037 - Endocrinology Physiology) Receptor PathwaysDocument4 pages037 - Endocrinology Physiology) Receptor Pathwaysیوسف رمضانNo ratings yet
- Pharmacodynamics 1Document65 pagesPharmacodynamics 1Kavya SivakarthikeyanNo ratings yet
- DR Dewi Farmakologi Pada Gangguan Neurologi - Maret 2021 DewiDocument81 pagesDR Dewi Farmakologi Pada Gangguan Neurologi - Maret 2021 DewiclarissaNo ratings yet
- Class 14. Signal Transduction: A Cascade of Events Within A Cell Translates Signals Into Cellular ResponsesDocument7 pagesClass 14. Signal Transduction: A Cascade of Events Within A Cell Translates Signals Into Cellular ResponsesLuis David Morocho PogoNo ratings yet
- Receptors: Receptor Tyrosine Kinases (RTK)Document5 pagesReceptors: Receptor Tyrosine Kinases (RTK)Safiya JamesNo ratings yet
- Molecular Pharmacology of Cell SignlingDocument100 pagesMolecular Pharmacology of Cell SignlingMohanad Al-BayatiNo ratings yet
- ميحرلا نمحرلا ﷲ مسب In the name of Allah the most Gracious and the most mercifulDocument32 pagesميحرلا نمحرلا ﷲ مسب In the name of Allah the most Gracious and the most mercifulAsmaa El SawyNo ratings yet
- Endocannabinoids/ Anandamide: Group 16A Dacuray. Deocampo. Figueroa. Garcia. Inacay. Medenilla. Patacsil. SicatDocument10 pagesEndocannabinoids/ Anandamide: Group 16A Dacuray. Deocampo. Figueroa. Garcia. Inacay. Medenilla. Patacsil. SicatJustin Garcia100% (1)
- F22 MCB 2050 Lecture 10 - Signal TransductionDocument28 pagesF22 MCB 2050 Lecture 10 - Signal TransductionNO VIDEOSNo ratings yet
- Cell and Molecular Biology: Gerald KarpDocument53 pagesCell and Molecular Biology: Gerald Karppat ongNo ratings yet
- Pharmacodynamics Mechanisms of Drug ActionDocument47 pagesPharmacodynamics Mechanisms of Drug ActioneciNo ratings yet
- Types of Signalling Pathway GPCR Pathway Normal and DysregulatedDocument78 pagesTypes of Signalling Pathway GPCR Pathway Normal and Dysregulatedapi-251915360No ratings yet
- General Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalDocument58 pagesGeneral Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalYashasv BhatnagarNo ratings yet
- SignalingDocument44 pagesSignalingMOCHILNo ratings yet
- Pharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDocument64 pagesPharmacodynamics: Digvijaya Lecturer School of Medical & Allied Sciences GD Goenka UniversityDigvijayaNo ratings yet
- NeurotransmittersDocument36 pagesNeurotransmittersmk5370096No ratings yet
- Day 22 Signaling 1: General Concepts and cAMP Pathway: - You Should Be Able To ExplainDocument20 pagesDay 22 Signaling 1: General Concepts and cAMP Pathway: - You Should Be Able To Explainshouq huusainNo ratings yet
- Chapter 1 - Hormones and Hormone ActionDocument42 pagesChapter 1 - Hormones and Hormone Action張宏軒No ratings yet
- Lehninger - PPT - ch12 AllDocument93 pagesLehninger - PPT - ch12 Allmissoni0408No ratings yet
- Prinsip Aksi ObatDocument49 pagesPrinsip Aksi ObatyulinarsihNo ratings yet
- Signal Transduction Pathways: Pratt & Cornely, Chapter 10Document23 pagesSignal Transduction Pathways: Pratt & Cornely, Chapter 10Brother GeorgeNo ratings yet
- Transmembrane and Kinase ReceptorsDocument20 pagesTransmembrane and Kinase ReceptorssasqiaNo ratings yet
- MD ch5Document27 pagesMD ch5malake.a13cj7No ratings yet
- Chapter 9 BIO 1510Document26 pagesChapter 9 BIO 1510Chachi CNo ratings yet
- L20 Signal Transduction and Mechanism of Hormone ActionDocument51 pagesL20 Signal Transduction and Mechanism of Hormone Actionyebadem228No ratings yet
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- Apoptosis Lecture 2023 2024Document115 pagesApoptosis Lecture 2023 2024Thái AnNo ratings yet
- Syllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesDocument92 pagesSyllabus For 5-Years Integrated M. Sc. Degree: UM-DAE Centre For Excellence in Basic SciencesAubal ShaubalNo ratings yet
- 2010 A Level H2 Biology P2 AnsDocument8 pages2010 A Level H2 Biology P2 AnsImagreenbucklegirl SGNo ratings yet
- 59c566785b913 PEMFhowitworksDocument20 pages59c566785b913 PEMFhowitworksWalter SchmittNo ratings yet
- Regulatory Network of Genes Associated With Stimuli Sensing Signal Transduction and Physiological Transformation of Appressorium in Magnaporthe Oryzae PDFDocument13 pagesRegulatory Network of Genes Associated With Stimuli Sensing Signal Transduction and Physiological Transformation of Appressorium in Magnaporthe Oryzae PDFAmalNo ratings yet
- Legend PlexDocument12 pagesLegend Plexkike1790No ratings yet
- Acquisition of A Hybrid E M State Is Essential For Tumorigenicity of Basal Breast Cancer CellsDocument12 pagesAcquisition of A Hybrid E M State Is Essential For Tumorigenicity of Basal Breast Cancer CellsgangligonNo ratings yet
- Functions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1Document33 pagesFunctions of p21 in Cell Cycle, Apoptosis and Transcriptional Regulation After DNA Damage-1rayanahfedanNo ratings yet
- Second Messenger SystemsModDocument49 pagesSecond Messenger SystemsModganotNo ratings yet
- M.Sc. - Molecular Human GeneticsDocument32 pagesM.Sc. - Molecular Human GeneticsSiman SimanNo ratings yet
- R J Epstein-Human Molecular Biology - An Introduction To The Molecular Basis of Health and Disease-Cambridge University Press (2002)Document655 pagesR J Epstein-Human Molecular Biology - An Introduction To The Molecular Basis of Health and Disease-Cambridge University Press (2002)Libros a Color ConceNo ratings yet
- Apoptosis Cancer Signaling PathwaysDocument1 pageApoptosis Cancer Signaling PathwayssyafikaNo ratings yet
- General Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalDocument58 pagesGeneral Pharmacology: Pharmacodynamics: Dr. Sahil Kumar NautiyalYashasv BhatnagarNo ratings yet
- Semester 1 Rev 2019Document33 pagesSemester 1 Rev 2019Anthony WilsonNo ratings yet
- Gpcrs and CancervistaDocument45 pagesGpcrs and CancervistapriyaaNo ratings yet
- Gpat 2023Document11 pagesGpat 2023Bobi JiNo ratings yet
- G Protein Coupled Receptor (GPCR) Adenylyl Cyclase: Ligand BindingDocument3 pagesG Protein Coupled Receptor (GPCR) Adenylyl Cyclase: Ligand BindingPanda DaoNo ratings yet
- Syndecans in Inflammation at A Glance: Sandeep GopalDocument8 pagesSyndecans in Inflammation at A Glance: Sandeep GopalYeni PuspitasariNo ratings yet
- Lecture-Cell Membranes and SignalingDocument64 pagesLecture-Cell Membranes and SignalingDiabyNo ratings yet
- Inflammation Panel ContentDocument2 pagesInflammation Panel ContentBogdan A. GireadăNo ratings yet
- Endocrine Physiology: Felix E. Grissom, Ph.D. 2219 Adams Building Howard University Tel. (202) 806-4512Document30 pagesEndocrine Physiology: Felix E. Grissom, Ph.D. 2219 Adams Building Howard University Tel. (202) 806-4512Inis LeahyNo ratings yet
- Physical Exercise and Epigenetic Modifications in Skeletal MuscleDocument15 pagesPhysical Exercise and Epigenetic Modifications in Skeletal MuscleAmin AminiNo ratings yet
- B.Sc. Cardiac Perfusion Technology FinalDocument32 pagesB.Sc. Cardiac Perfusion Technology FinalTanisha ShaikhNo ratings yet
- My Cheat SheetDocument3 pagesMy Cheat SheetTenzin KyizomNo ratings yet
- Cancer Drug Discovery - Science and History-Springer Netherlands (Libro-2016)Document286 pagesCancer Drug Discovery - Science and History-Springer Netherlands (Libro-2016)ELMERNo ratings yet
- Funcional Analysis of PTHIR Variants Found in Primary Failure of EruptionDocument8 pagesFuncional Analysis of PTHIR Variants Found in Primary Failure of EruptionvivgaitanNo ratings yet
- Cytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014Document101 pagesCytokines, Cytokine Receptors and Chemokines: Sept. 11, 2014ANJU0709No ratings yet
- Pharmacology of Central Nervous SystemDocument20 pagesPharmacology of Central Nervous SystemAngelic khan100% (1)